
Recommended
Recommended
More Related Content
Similar to Examining the role of parental factors on depression amongUr
Similar to Examining the role of parental factors on depression amongUr (20)
More from BetseyCalderon89
More from BetseyCalderon89 (20)
Recently uploaded
Recently uploaded (20)
Examining the role of parental factors on depression amongUr
- 1. Examining the role of parental factors on depression among Urban African American youth living in public housing Anthony T. Estreet a,b, Dawn Thurmana, Sapphire Goodmana,b, M. Taqi Tirmazia,b, Takisha J. Cartera, and Von Nebbittc aSchool of Social Work, Morgan State University, Baltimore, Maryland, USA; bHealth & Addiction Research Training Lab, Morgan State University, Baltimore, Maryland, USA; cGeorge Warren Brown School of Social Work, Washington University in St. Louis, St. Louis, Missouri, USA ABSTRACT This study examined the potential risk and protective parental factors associated with depression among African American youth living in public housing. Utilizing a community-based participatory research approach, 239 African-American youth surveys were collected during 2013–2014 in two urban public housing developments with low socioeconomic profiles. Over half (52.3%) of the sample was in high school and female (58%). 65.3% reported living with their mother while 38% reported being employed. Bivariate analysis revealed sig- nificant correlations between depression and maternal substance abuse, paternal monitoring, parent-child relationship, and family
- 2. time. Results from the regression analyses indicated that higher depression scores were significantly associated with youth who reported poor parent-child relationships, low levels of paternal super- vision and high levels of maternal drug abuse. These findings provide support for claims about the importance of parent-child relationship and paternal monitoring as a protective factor for depressive symp- toms, particularly during adolescence. Moreover, findings suggest that interventions which are targeted towards urban African American youth should address parental factors as a pathway to decrease depression among this population. KEYWORDS Depression; risk factors; protective factors; African American; youth Introduction Depression among African Americans youth is a major public health concern that has been linked to substance use, heightened sex-risk and suicidal behaviors (i.e., ideation and attempts) (Breland-Noble, Burriss, & Poole, 2010; Okwumabua, Okwumabua, & Wong, 2014). Although there has been a slight increase in focus on depression among African American youth over the last decade, this group remains understudied in mental health research (Matlin, Molock, & Tebes, 2011). Evidence suggests that parents and family play a critical role in the lives of their adolescent and emerging adult
- 3. children (Lindsey, Joe, & Nebbitt, 2010). It is reasonable to postulate, therefore, that parental factors are related to the emotional well-being of urban African American youth. Using a sample of 239 African American youth living in urban public housing, this paper contributes to the gap in CONTACT Anthony T. Estreet [email protected] School of Social Work, Morgan State University, 1700 East Cold Spring Lane, Baltimore, MD 21251, USA. JOURNAL OF HUMAN BEHAVIOR IN THE SOCIAL ENVIRONMENT 2018, VOL. 28, NO. 4, 494–508 https://doi.org/10.1080/10911359.2018.1430647 © 2018 Taylor & Francis http://orcid.org/0000-0002-2413-6311 https://crossmark.crossref.org/dialog/?doi=10.1080/10911359.2 018.1430647&domain=pdf&date_stamp=2018-06-21 knowledge by assessing how, or whether, parental factors are related to depressive symptoms in this vulnerable population. Epidemiology of depression African American youth According to the recent findings, approximately 2.5 million U.S. youth ages 12–17 had a major depressive episode (MDE) in the previous year. Of those with MDE, approximately
- 4. nine percent represented African American youth who were diagnosed during the same period (SAMHSA, 2015). Additionally, an estimated 5.8 million young adults (18–25) were diagnosed with major depressive episodes during that same period (SAMHSA, 2015). According to the National survey for drug use and health, rates of major depressive episodes have significantly increased among youth since 2005 (SAMHSA, 2016). Research has indicated that African American youth who reside in high-risk environments (increased levels of violence, substance abuse, and poverty) such as public housing settings have shown increased rates of depression (Nebbitt & Lombe, 2007; Nebbitt, Williams, Lombe, McCoy, Stephens, 2014). Comparatively, past research on African American youth and depression has resulted in mixed findings. For example, a recent study found lower rates of depression among African American young people when compared to their white counterparts (Breland et al., 2014). Conversely, a few studies have indicated that African Americans experience depression at greater rates than other ethnic groups (Lopez et al., 2017; Yip, 2015). While others found no racial difference in depression between African American and White youth (Schraedly, Gotlib, & Hayward, 1999). Research is inconclusive on age and gender differences among youth with depression. Previous research suggests that girls are twice as likely as boys to develop depression and symptoms of depression increase with age (Maughan,
- 5. Collishaw, & Stringaris, 2013). Other studies found no associations between depression and age (Bryant, 2008; Shaffer, Forehand, Kotchick, 2002) or depression and gender among a sample of urban African American youth (Nebbitt & Lombe, 2007). Youth in urban environments Research has also identified a myriad of social determinants of depression among African American youth (Respress, Morris, Gary, Lewin, & Francis, 2013). In addition to its impact on education, self-esteem, and anxiety, depression has been linked to substance use, sexually risky and suicidal behaviors (i.e., ideation and attempts) (Busby, Lambert, Ialongo, 2013; Jackson, Seth, Diclemente, Lin, 2015; Ofonedu, Percy, Harris-Britt, Belcher, 2012; Okwumabua, Okwumabua, Wong, 2014). Despite an increase in attention to depression among African American youth over the last decade, this group remains underrepresented in mental health research, which addresses depression and other mood disorders (Breland-Noble, Al-Mateen, Singh, 2016). Several researchers who have explored depressi on among African American youth sought to examine parental and familial risk and protective factors (Agerup, Lydersen, Wallander, & Sund, 2014; Boyd & Waanders, 2013; Campbell - Grossman et al., 2016; Carter, Dellucci, Turek, & Mir, 2015; Chen, 2013; Cooper, Brown, Metzger, Clinton, & Guthrie, 2013; Hurd, Stoddard, & Zimmerman, 2013). Additional studies have found a decrease in depression
- 6. JOURNAL OF HUMAN BEHAVIOR IN THE SOCIAL ENVIRONMENT 495 among African American youth who have an optimistic outlook during stressful situations as well as those who perceive to have a support system (Chen, 2013). Financial stressors were also positively associated with depressive symptoms (Taylor, Budescu, Gebre, & Hodzic, 2014). African American youth are more likely to live in urban communities marked by residential segregation and concentrated poverty (U.S. Census Bureau, 2010). The chal- lenges of living in urban communities may be exacerbated for young people living in and around public housing (Nebbitt, 2015). Urban public housing developments are often epicenters of crime, violence, and alternative drug markets (Nebbitt, 2015). Furthermore, budget cuts and closure of key social services has led to a weaker form of social safety net and greater hardships among urban communities like public housing. Despite living in challenging environments and under foreboding circumstances, many youth in these communities can graduate high school, go to college and gain employment, and become healthy productive adults (Nebbitt, 2009). Indeed, it must be extremely difficult to navigate these harsh environments while simultaneously managing challenges that come with the developmental phase of adolescence.
- 7. Theorists (Nebbitt, Sanders-Phillips, & Rawlings, 2015) have suggested that minority families adapt to life in harsh environments by forming stronger familial ties and networks to protect children and youth. Parents and family may serve as primary support systems in harsh environments and especially during youth. The important roles that parents play in the lives of minority youth have been well documented. Parental factors such as parent- child relationship, parental encouragement, and parental supervision have been found to be protective factors against depressive symptoms (Henricson & Roker, 2000; Lindsey, Joe, & Nebbit, 2010; Nebbitt, Lombe, & Lindsey, 2007; Tandon & Solomon, 2010). Parental factors and depression Several risk and protective factors have been identified in the literature as follows: alcohol use, cannabis use, dieting, coping strategies, other illicit drug use, sleep, tobacco use and weight (Cairns, Yap, Pilkington, & Jorm, 2014). Emerging research on risk and protective factors associated with depression include dating during adolescence, media use, physical activity, relationships with positive peers, self-disclosure to parents and sports (Cairns et al., 2014). Similarly, Lindsey and colleagues suggest that parents and family play a critical role in the lives of their youth and emerging adult children (Lindsey et al., 2010). It is reasonable to postulate, therefore, that parental factors are related to the emotional well- being of urban African American youth.
- 8. Sagrestano and colleagues (2003) explain that most studies assessing depression among African American youth tend to examine the association between depression and exter- nalizing problem behaviors. However, researchers have found a positive relationship between parental factors and depression. For example, several studies have found an inverse relationship between family cohesion and warmth and depressive symptoms (Bond, Toumbourou, Thomas, Catalano, & Patton, 2005; Sagrestano et al., 2003). In addition, researchers (Lindsey et al., 2010; Matlin, Molock, & Tebes, 2011) have examined the role of parental support and depression. For example, Zimmerman and colleagues (2000) found parental support serves as a protective factor on depressive symptomology. Similarly, Holt and Espelage (2005) reported that maternal social support can moderate the relationship between victimization and depressive symptoms among African American 496 A. T. ESTREET ET AL. males. Literature on the moderating effect of parental support on gender is inconsistent. Meadows (2007) and colleagues (Bean, Barber, & Crane 2006) report a stronger associa- tion between parental support and depression among girls rather than boys. In other studies, gender failed to moderate the effect of parental support on depression (Chester,
- 9. Jones, Zalot, & Sterrett, 2007; Gutman & Eccles, 2007). Tandon and Solomon (2009) found that living with an adult with substance abuse problems, greater exposure to violence, and delinquent peers were related to higher depressive symptoms among African American youth. However, research on maternal and paternal history of substance abuse, parent-child relationships and depression is limited. This study aims to examine the association between parental factors and depres- sion among a sample of African American living in and near the public housing development. Purpose and hypothesis of present study Given the current knowledge of risk and protective factors associated with depressive symptoms, this study examined paternal drug use, maternal drug use, maternal encour- agement, maternal supervision, paternal encouragement, and paternal supervision as potential parental factors associated with depressive symptoms among African American youth. Moreover, family time and parent-child relationship were examined as family factors. The aim of this study was to examine parent and family risk and protective variables for their potential association with youth depression. The hypotheses for this study were: (a) higher reporting of paternal and maternal drug use will be related to higher levels of depressive symptoms; (b) higher reporting of family time, maternal supervision
- 10. and parent-child relationship will be related to lower levels of depressive symptoms, and c) higher reporting of maternal and paternal encouragement will be related to lower levels of depressive symptoms. Methods The current study is part of a larger cross-sectional study which utilized a Community- Based Participatory Research approach in examining the sociocultural correlates of psy- chological functioning and behavioral health of African American youth living in public housing and neighboring communities in North West Baltimore. Community representa- tives including parents and youth were primary participants selecting variables under investigation. Participants Participants were 239 youth selected from 2 urban public housing developments and neighboring catchment areas in Baltimore with approximately 70% of children living below the poverty line (Baltimore Neighborhood Indicators Alliance, 2014). They were in high school (52.3%), graduated high school (29.3%), and enrolled in college (14.3%). The majority of participants were female (58%) with ages ranging from 13 to 24. The sample was drawn from predominantly African American communities where 96.4% of the students enrolled in public schools were African American students and 89.5% of
- 11. JOURNAL OF HUMAN BEHAVIOR IN THE SOCIAL ENVIRONMENT 497 people in the community were African-Americans (Baltimore Neighborhood Indicators Alliance, 2014). The median family income was $14,105 and 67.2% of families had an annual income less than $25,000 (Baltimore Neighborhood Indicators Alliance, 2014). Instruments Parent/child relationship was assessed using two subscales from the National Youth Survey (NYS), (Elliot, 1987). The first subscale is composed of 4-item from the Quality of Parental Relationship Scale. The 4-item subscale assesses a youth’s perception of the quality of their relationship with her parents. Participants were asked, for example: “How satisfied are you with your relationship with your parents?” Responses range from “very dissatisfied = 1” to “very satisfied = 5.” Another item asked, for example, “How much warmth and affection do you receive from your parents?” Responses range from “very little = 1” to “a great deal = 5.” The subscale demonstrated acceptable internal consistency with the current sample (α = .79). The second subscale included 4-items that assessed the quality of time spent with parents. Participants were asked, for example, “My parents or the adult who has taken care of me or takes care of me spends time just talking
- 12. with me.” Responses range from “almost never = 1 to few times a day = 4”. The subscale demonstrated acceptable internal consistency with the current sample (α = .71). Each subscale is summed so that higher scores represent a higher quality parent-child relationship. Caregiver’s status was assessed using two items. The first item states, In my household the person I consider to be my MOTHER is: A biological mother (e.g., your natural mother who had you) = 1, my stepmother = 2, a relative (e.g., uncle, grandmother) = 4, an adult who is not related to me (e.g., foster parent, or none of the people I live with) = 4, I live alone = 4. The second item states, In my household the person I consider to be my FATHER is: My biological father (e.g., your natural father) = 1, my stepfather = 2, a relative (e.g., uncle, grandfather) = 3, an adult who is not related to me (e.g., foster parent) = 4, I live alone = 5. Parental Alcohol and Drug Use was assessed using four items. The first two items ask, “How often does your father use the drugs?” The second item asked, “How often does your mother use drugs?” Responses range from “none of the time” to “once a month” to “once a week” to “a few times a month” to “few times a week” to “every day”. The choices of drugs were marijuana, crack/cocaine, PCP, heroin, prescription medication (i.e. Oxycontin, Vicodin, Valium, Percocet). The next two items ask “How often does your
- 13. father drink alcohol?” and “How often does your mother drink alcohol?” Responses ranged from “none of the time” to “once a month” to “once a week” to “a few times a month” to “few times a week” to “every day”. Parental supervision and support To assess parental supervision and support, youth completed the Parental Attitude Measure (PAM) (Lamborn, Mounts, Steinberg, & Dornbusch, 1991). PAM is a 12-item scale that measures two latent constructs: parental supervision (5-items) and parental encouragement (7-items). In the current study, we modified the 12-item scale to assess paternal supervision/encouragement and maternal supervision/encouragement separately. Following are examples of an item on the original parental supervision subscale: “How much does your parent or the adult who takes care of you really know who your friends 498 A. T. ESTREET ET AL. are?” We modified this item to read: “How much does your mother or the adult female who takes care of you really know who your friends are?” and “How much does your father or the adult male who takes care of you really know who your friends are?” Items are scored on a four-point Likert scale ranging from “doesn’t know = 1” to “know exactly = 4.” The five-item subscales demonstrated acceptable paternal and maternal reliability
- 14. with the current sample. Parental encouragement An example of an item on the original parental encouragement subscale reads: “Does your father/mother, stepfather/stepmother or the adult man/woman who takes care of you push you to do your best in whatever you do?” We modified this item to read: “Does your mother, stepmother or the adult woman who takes care of you push you to do your best in whatever you do?” and “Does your father, stepfather or the adult man who takes care of you push you to do your best in whatever you do?” Items are scored on a four - point Likert scale ranging from “never = 1” to “always = 4.” The 7-item subscales demonstrated acceptable maternal and paternal reliability, respectively, with the current sample. PAM is scored by summing the items with higher values indicating higher levels of supervision and encouragement. Depressive symptoms were assessed using the Center for Epidemiologic Studies Depression Scale (CES-D). CES-D has extensive use in assessing depression and psychia- tric epidemiology. The CES-D is a 20-item scale that assesses mood, somatic complaints, social interactions with others, and motor functioning. Responses are rated on a 4-point Likert scale ranging from “rarely or none of the time (less than one day)” = 0 to “most or all of the time (5–7 days)” = 3. The final score spans from 0 to 60, with a higher score indicating greater impairment. Respondents with a score of 16 or higher are at greater risk
- 15. for clinical depression. Researchers have used various cut-off scores ranging from 12 to 24 for youth (Stockings et al., 2015). Among community samples, internal consistency estimates range from .80 to .90 (Nebbitt & Lombe, 2007; Stockings et al., 2015). The CES-D demonstrated acceptable reliability with the current youth sample (α = .82). Procedure Approval for this study was obtained from Morgan State University Institutional Review Board. Participants under 18 years of age were given an informed consent form that needed to be signed by parents as well as an assent form before participating in the study. Participants 18 years of age and older were allowed to sign the consent form on the day of the data collection. The study utilized a self-administered survey technique both individually and in small groups of 5. The survey took between 30 – 45 minutes to complete. Participants were given a target gift card for participating in the study. Consent forms and assent forms were collected before data collection. Youth were recruited in the public housing developments, outside recreation centers and social services agencies in the community. Recruitment consisted of flyers and announcements at local community centers. Members of the research team, agency liaisons, and community liaisons posted flyers in the housing
- 16. developments, in commu- nity centers and in agencies around the housing developments. In addition, recruitment cards were distributed to youth living in the communities. The flyers and recruitment JOURNAL OF HUMAN BEHAVIOR IN THE SOCIAL ENVIRONMENT 499 cards included a brief overview of the study, the date and location for data collection, and contact information for the PI and RA. In addition, respondent- driven sampling techni- que was utilized to recruit participants for the study. Community engagement involved a consistent, malleable, and sensitive plan. The consistency of the plan involved a methodological process that required community ties and that reliably culminated with the successful collection of data. The malleability of the plan involved a willingness to make slight modifications to accommodate the unique characteristics of the public housing development and catchment areas. The sensitivity of the plan involved an awareness that public housing communities are not monolithic; that is, an understanding that each housing site is a unique context in its own right; and within each context, cultural norms may differ. Using a Community Based Participatory Research (CBPR) approach allowed a greater buy-in from the community as members of the community took
- 17. part in all phases of the study. Community engagement, honesty, and transparency are salient to a successful com- munity-based participatory research project. The researcher fostered genuine rapport with residents and asked for their involvement in all phases of the research project. Residents are considered primary stakeholders because their involvement is a necessary and sufficient condition to the success of CBPR within public housing developments and neighboring catchment areas. It is our position that without their support and buy-in, research in public housing and neighboring catchments areas would be extremely challenging. Analytic strategy In preparation for regression analysis, several inferential statistics were used to examine the bivariate relationships between parent and family factors and youth depression and to assess gender and age differences. These analyses were conducted in order to eliminate variables in the regression analyses that did not have significant correlations with youth depression. Univariate statistics, Pearson’s correlations, independent t-tests, and one-way ANOVAs were conducted as part of our preliminary analysis. Our primary analysis included an ordinary least squared regression. Prior to conducting the analysis, data were evaluated for missing observations and normality. Missing cases and skewed variables were within the acceptable range. Descriptive statistics and graphs (e.g.,
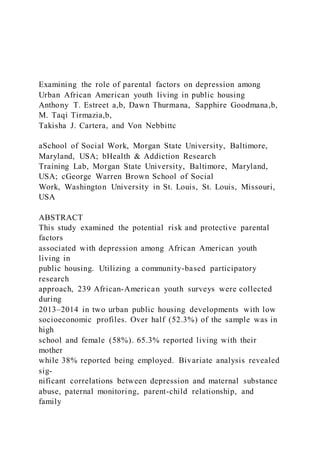
- 18. measures of skewness and kurtosis, histograms, Q-Q plots, and scatterplots) were also generated and confirmed that regression assumptions (normality, linearity, and homoscedasticity) were met. In addition, variance inflation factors (VIF) and tolerance values were also generated and showed no multicolli- nearity among the variables. Stepwise linear regression was the primary analytic procedure. Results Sample characteristics Participants in the study ranged in age from 13 to 24 years of age with a mean age of 18.2 years. Females composed 58% sample. Over half (52.3%) of the participants were in high school, 29.3% had graduated high school and 14.3% were enrolled in college. Almost three-fourths (74.1%), of the sample lived with their parents, 21.3% living alone, and the remaining 5% were living with relatives and/or friends. Sixty- five percent of the sample 500 A. T. ESTREET ET AL. reported their mother lived in the household and 37.2% reported their father lived in the household. Lastly, 38.1% of the participants were employed at the time of data collection. Sample characteristics are presented in Table 1. Pearson correlations were conducted to determine the
- 19. associations between parent/ family factors and depression. The results of the Pearson correlation test are presented in Table 2. The results show a statistically significant positive correlation between depression and maternal drug use (r = .16, p < .01). Additionally, there was a statistically significant negative correlation between family time (r = -.12, p < .01), parent-child relationship (r = -.27, p < .01), paternal supervision (r = -.16, p < .05) and youth depression. Findings from the t-test reveal no differences in regard to gender and ANOVA revealed no difference in depressive symptoms among early youth (13 – 15), middle youth (16 – 19), and later youth (20 – 24). Parental factors Participants reported an average of 15.11 (SD = 7.96) on paternal encouragement and average of 11.59 (SD = 5.25) paternal supervision. Participants reported an average of 20.50 (SD = 8.89) on maternal encouragement and an average of 14.52 (SD = 6.05) on maternal supervision. Lastly, 28.1% of the participant’s mothers had problems with Table 1. Sample characteristics. Female (58%) Male (42%) Total Variable n % n % N % Early Adolescence 44 18.4 44 18.4 88 36.8 Middle Adolescence 45 18.8 37 15.5 82 34.3 Later Adolescence 49 20.5 20 8.4 69 28.9 In H.S. 77 32.2 48 20.1 125 52.3
- 20. Graduated H.S. 47 19.7 28 11.7 75 31.4 In-College 28 11.7 11 4.6 39 16.3 Living Situation Living with parents 102 42.7 86 36.0 188 78.7 Living alone 36 15.1 15 6.3 51 21.3 Caregiver Status Mother in-home 86 36.0 70 29.3 156 65.3 Father in-home 45 18.8 44 18.4 89 37.2 Employed 48 20.1 43 18.0 91 38.1 Table 2. Pearson correlations. Pearson Correlations 1 2 3 4 5 6 7 8 9 1. Paternal Drugs — 2. Maternal Drugs .539** — 3. Family Time −.106 −.180** — 4. Parent-Child Relationship −.066 −.043 .503** — 5. Maternal Encouragement .056 −.036 .207** .252** — 6. Maternal Monitoring −.030 −.001 .253** .313** .370** — 7. Paternal Encouragement −.020 −.140* .191** .137* .261** .354** — 8. Paternal Monitoring −.003 .050 .017 −.009 .072 .180** .243** — 9. Depression (CESD) .071 .161** −.121* −.266** −.020 −.102 −.103 −.155** — Means .66 .51 9.01 13.99 20.50 14.52 15.11 11.59 10.85 **. Correlation is significant at the 0.01 level (1-tailed). *. Correlation is significant at the 0.05 level (1-tailed). JOURNAL OF HUMAN BEHAVIOR IN THE SOCIAL ENVIRONMENT 501
- 21. alcohol/drug use and 39.3% of the participant’s fathers had problems with alcohol/ drug use. Family factors Participants reported an average of 13.99 (SD = 4.73) on family child relationship and an average of 9.01 (SD = 3.04) on family time. Depressive symptoms Participants reported an average depression score of 10.85 with a standard deviation of 8.65. However, 28.9% of the participants had a score of < 16 and 17.6% had a score < 24. Using the suggested cutoff score of 24 (Nebbitt & Lombe, 2007), a little over 17% of participants reported minimal to mild symptoms. There were no statistical differences in regard to gender and age among the sample. Predictors of depression The results of the stepwise multiple regression analysis are presented in Table 3. Of the 4 factors entered in the regression analysis, three emerged as significant predictors of levels of depression (F= 5.35, p< .005). With a beta of -.266 (p< .01), parent-child relationship emerged as the strongest predictor of depression accounting for 7.1% of the variance in depression. The second strongest factor was paternal supervision (β= .152, p < .01) accounting for an additional 2.3% of the variance in depression. The third strongest factor was maternal drug use (β=
- 22. .142, p < .05) accounting for a modest 2.0% of the variance in depression. These results indicate that presence of depressive symptoms among African American is a function of a weak parent-child relationship, paternal supervision, and history of maternal drug use. Overall, this predicted regression model explains a modest 11.4% of the total variance in levels depression. Therefore, a little over 88% of the variance is unexplained. Discussion Understanding the relationship between depressive symptoms and protective factors is critical for advancing our knowledge of depression among African American youth. The current study sought to examine potential risk and protective factors. Results from the study suggest depressive symptoms among African American youth are associated with higher maternal drug use, family time, paternal supervision and the parent-child relationship. We hypothesized that higher reporting of paternal and maternal drug use will be related to higher levels of depressive symptoms. This w as partially supported. Higher levels of maternal drug use were related to higher levels of depressive symptoms. This finding was consistent with a study that suggests examining the relationship between Table 3. Stepwise regression model: depression. Model R R2 F p β t p
- 23. Parent-Child Relationship .266 .067 18.10 .000 −.266 4.900 .000 Paternal Monitoring .307 .094 6.05 .015 −.152 3.865 .000 Maternal Drug Use .338 .114 5.35 .022 .142 2.252 .000 502 A. T. ESTREET ET AL. parental alcohol and drug use and depressive symptoms (Tandon & Solomon, 2010). Our hypothesis regarding the relationship between paternal drug use and depressive symptoms was not supported. This could be explained by the fact that over 70% of African American youth households within our study were single-parent homes in which the mother was the primary caregiver. The absence of a substance-abusing father in the home may buffer the impact of youth developing depression. Parental factors need to be considered when exploring depressive symptomology among urban African American youth. As expected, key parental factors (child-family relationship, paternal supervision, and maternal drug abuse) were associated with depres- sion in our study. However, only partial hypothesis was found to be true in the study, as paternal and maternal encouragement, maternal supervision, and paternal drug use did not have statistically significant relationships. The findings of this study affirm previous studies with urban African American youth, which found an association between parental
- 24. factors and depressive symptoms (Barton et al., 2015; Agerup et al., 2014; Garthe, Sullivan, & Kliewer, 2015). Likewise, findings from this study were consistent with previous literature, which found a positive relationship between child family relationship and depressive symptoms (Choe, Stoddard, & Zimmerman, 2014; Hunt, Caldwell, & Assari, 2015; Taylor, Budescu, & Gebre, 2016). Findings also support previous research, which suggests that lack of parental supervision can lead to increased depressive symptomology among African-American youth (Hamza & Willoughby, 2011; Yap, Pilkington, Ryan, & Jorm, 2014). Moreover, a systemic review of the literature found a relationship between maternal drug abuse and depressive symptoms (Yap et al., 2014). The results reported in this study offer a glimpse of the relationship among parental factors and depressive symptoms among urban African American youth living in and adjacent to public housing developments. Parent-child relationships and parental super- vision play a critical role in buffering the mental health risk of African American youth in urban communities. Findings from the study suggest that interventions addressing depres- sive symptoms among urban African American youth should be targeted to address parental factors that contribute to depression. In addition, future research studying depression among urban African Americans should include comparative samples to
- 25. examine the difference regarding ethnicity. Given the importance of parents in the lives of children and youth, parental factors across ethnic backgrounds should be explored. Also, due to the complexities in the lives of urban African American youth, longitudinal studies should be conducted to explore the difference in depressive symptoms across time. Although measures to gauge youth depression have become more established over time, we need to utilize multiple measures and techniques to gauge depressive symptoms targeted to urban youth to ensure we are able to accurately capture depressive sympto- mology among this population. While the findings of this study partially supported the hypothesis between parental factors and depression, future studies should aim to include psychological functioning and behavioral health. The presence of parental substance abuse has been found to be correlated with sexual risk-taking behavior, behavioral health, and food insecurity (Lombe, Nebbitt, Chu, Saltzman, & Tirmazi, 2017; Nebbitt et al., 2015; Lombe, Nebbitt, Sinha, & Reynolds, 2016). JOURNAL OF HUMAN BEHAVIOR IN THE SOCIAL ENVIRONMENT 503 Strengths and limitations A strength of this study is its examination of key protective factors related to parents. The study’s approach to dichotomize parental factors into maternal
- 26. encouragement and monitoring and paternal encouragement and monitoring is critical to examining differences in maternal and paternal factors regarding depressive symptoms among youth. Although limited in its general- izability, the information provided is useful for researchers , educators, and practitioners. Given the relatively low to moderate level of depressive symptoms, future research should aim to further explore protective factors and strategies utilized by urban African American youth in combating stress. Due to the cultural nuances of urban communities, multiple techniques and measures to gauge depressive symptoms should be incorporated. The cross-sectional design limits this study’s ability to establish causal inferences. In addition, the accuracy of the data collected is limited due to response error as participants recall and self-report their feelings, perceptions, and behaviors. Also, numerous risk factors such as discrimination, exposure to violence, delinquent behaviors, and drug use were not included in the analysis and may influence depressive symptoms among the sample. Furthermore, findings of this study are limited in its generalizability as the data were collected in and adjacent to housing developments in North West Baltimore. Generalizing to other urban communities and African American youth should be done with caution. Lastly, using a community based participatory research approach blended with a community action research approach may be critical in developing trust, rapport, and a collective research approach to address both community
- 27. and academic inquiry. Conclusion This study contributes to literature examining depressive symptoms among a sample of urban African American youth in and adjacent to public housing developments (Breland- Noble, Burriss & Poole, 2010; Lindsey et al., 2010; McMahon, Coker, & Parnes, 2013; Nebbitt et al., 2014; Tandon & Soloman, 2010). These findings provide support for claims about the importance of parent-child relationship and paternal monitoring as a protective factor for depressive symptoms, particularly during adolescence. While maternal drug use serves as a risk factor for depressive symptoms among this population of urban youth, paternal drug use does not. Our understanding of the samples demographic could play a tremendous role in the findings. Considering most of the study participants (65.3%) reside with their mother, it stands to reason their exposure to her substance use would have a greater impact as compared to paternal substance use. That is not to say that the role of the father is insignificant. Our research suggests that paternal monitoring has a greater effect on youth depressive symptoms than maternal monitoring. Intervention efforts aimed at parents of depressed youth may consider educating fathers on the protective role of their presence in their child’s life. Acknowledgment
- 28. At the time of this publication, Dr. Anthony Estreet was a Scholar with the HIV/AIDS, Substance Abuse, and Trauma Training Program (HA-STTP), at the University of California, Los Angeles; supported through an award from the National Institute on Drug Abuse (R25 DA035692). 504 A. T. ESTREET ET AL. Disclosure Statement There is no financial interest held by any of the authors related to this research or publication Funding U.S. Department of Health and Human Services, Health and Resources Services Administration Grant # G02HP27946 ORCID Anthony T. Estreet http://orcid.org/0000-0002-2413-6311 References Agerup, T., Lydersen, S., Wallander, J., & Sund, A. M. (2014). Longitudinal course of diagnosed depression from ages 15 to 20 in a community sample: Patterns and parental risk factors. Child Psychiatry and Human Development, 45(6), 753–764. doi:10.1007/s10578-014-0444-8 Baltimore Neighborhood Indicators Alliance. (2014). Baltimore
- 29. neighborhood statistical profiles: United States Census 2014. Baltimore, MD: Baltimore Neighborhood Indicators Alliance. Retrieved from http://bniajfi.org/ Barton, A. W., Beach, S. R., Kogan, S. M., Fincham, F. D., Stanley, S. M., Hurt, T. R., & Brody. (2015). Prevention effects of trajectories of African American adolescents’ exposure to interpar- ental conflict and depressive symptoms. Journal of Family Psychology, 29(2). doi:10.1037/ fam0000073 Bean, R. A., Barber, B. K., & Crane, D. R. (2006). Parental support, behavioral control, and psychological control among African American youth: The relationships to academic grades, delinquency, and depression. Journal of Family Issues, 27(10), 1335–1355. Bond, L., Toumbourou, J. W., Thomas, L., Catalano, R. F., & Patton, G. (2005). Individual, family, school, and community risk and protective factors for depressive symptoms in adolescents: A comparison of risk profiles for substance use and depressive symptoms. Prevention Science, 6(2), 73–88. Boyd, R. C., & Waanders, C. (2013). Protective factors for depression among African American children of predominantly low-income mothers with depression. Journal of Child and Family Studies, 22(1), 85–95. doi:10.1007/s10826-012-9588-y Breland, D. J., McCarty, C. A., Zhou, C., McCauley, E., Rockhill, C., Katon, W., & Richardson, L. P.
- 30. (2014). Determinants of mental health service use among depressed adolescents. General Hospital Psychiatry, 36(3), 296–301. doi:10.1016/j.genhosppsych.2013.12.003 Breland-Noble, A., Burriss, A., & Poole, K. H. (2010). Engaging depressed African American adolescents in treatment: Lesson from the AAKOMA project. Journal of Clinical Psychology, 66 (8), 868–879. Breland-Noble, A. M., Al-Mateen, C. S., & Singh, N. N. (2016). Handbook of Mental Health in African American Youth. doi:10.1007/978-3-319-25501-9 Breland-Noble, A. M., Burriss, A., & Poole, H. K. (2010). Engaging depressed African American adolescents in treatment: Lessons from the AAKOMA PROJECT. Journal of Clinical Psychology, 66(8), 868–879. Bryant, D. N. (2008). Psychosocial correlates of depressive symptoms among African-American children. (Doctoral dissertation). Howard University, Washington, D. C. Busby, D. R., Lambert, S. F., & Ialongo, N. S. (2013). Psychological symptoms linking exposure to community violence and academic functioning in African American adolescents. Journal of Youth and Adolescence, 42(2), 250–262. doi:10.1007/s10964- 012-9895-z JOURNAL OF HUMAN BEHAVIOR IN THE SOCIAL ENVIRONMENT 505
- 31. http://dx.doi.org/10.1007/s10578-014-0444-8 http://bniajfi.org/ http://dx.doi.org/10.1037/fam0000073 http://dx.doi.org/10.1037/fam0000073 http://dx.doi.org/10.1007/s10826-012-9588-y http://dx.doi.org/10.1016/j.genhosppsych.2013.12.003 http://dx.doi.org/10.1007/978-3-319-25501-9 http://dx.doi.org/10.1007/s10964-012-9895-z Cairns, K. E., Yap, M. B., Pilkington, P. D., & Jorm, A. F. (2014). Risk and protective factors for depression that adolescents can modify: A systematic review and meta-analysis of longitudinal studies. Journal of Affective Disorders, 169, 61–75. doi:10.1016/j.jad.2014.08.006 Campbell-Grossman, C., Hudson, D. B., Kupzyk, K. A., Brown, S. E., Hanna, K. M., & Yates, B. C. (2016). Low-income, African American, adolescent mothers’ depressive symptoms, perceived stress, and social support. Journal of Child and Family Studies, 25(7), 2306–2314. doi:10.1007/ s10826-016-0386-9 Carter, J. S., Dellucci, T., Turek, C., & Mir, S. (2015). Predicting depressive symptoms and weight from adolescence to adulthood: Stressors and the role of protective factors. Journal of Youth and Adolescence, 44(11), 2122–2140. doi:10.1007/s10964-015- 0301-5 Center for Behavioral Health Statistics and Quality. (2015). Behavioral health trends in the United States: Results from the 2014 National Survey on Drug Use and Health. Retrieved from https://
- 32. www.samhsa.gov/data/sites/default/files/NSDUH-FRR1- 2014/NSDUH-FRR1-2014.htm Center for Behavioral Health Statistics and Quality. (2016). Key substance use and mental health indicators in the United States: Results from the 2015 national survey on drug use and health. Retrieved from https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR1- 2015/NSDUH- FFR1-2015/NSDUH-FFR1-2015.htm Chen, H. (2013). Robust protective factors for African American youths who have a parent with depression. Social Work Research, 37(12), 121–134. doi:10.1093/swr/svs026 Chester, C., Jones, D. J., Zalot, A., & Sterrett, E. (2007). The psychosocial adjustment of African American youth from single mother homes: The relative contribution of parents and peers. Journal of Clinical Child and Adolescent Psychology, 36(3), 356–366. doi:10.1080/ 15374410701444306 Choe, D. E., Stoddard, S. A., & Zimmerman, S. A. (2014). Developmental trajectories of African American adolescents’ family conflict: Differences in mental health problems in young adult- hood. Developmental Psychology, 50(4), 1226–1232. doi:10.1037/a0035199 Cooper, S. M., Brown, C., Metzger, I., Clinton, Y., & Guthrie, B. (2013). Racial discrimination, African American adolescents’ adjustment: Gender variation in family and community social
- 33. support, promotive and protective factors. Journal of Child and Family Studies, 22, 15–29. doi:10.1007/s10826-012-9608-4 Elliot, D. (1987). National Youth Survey [United States]: Wave VII, 1987 (ICPSR 6542). Retrieved from https://www.icpsr.umich.edu/icpsrweb/ICPSR/studies/6542. Garthe, R. C., Sullivan, T., & Kliewer, W. (2015). Longitudinal relations between adolescent and parental behaviors, parental knowledge, and internalizing behaviors among urban adolescents. Journal of Youth and Adolescence, 44(4), 819–832. doi:10.1007/s10964-014-0112-0 Gutman, L. M., & Eccles, J. S. (2007). Stage-environment fit during adolescence: Trajectories of family relations and adolescent outcomes. Developmental Psychology, 43(2), 522–537. doi:10.1037/0012-1649.43.2.522 Hamza, C. A., & Willoughby, T. (2011). Perceived parental monitoring, adolescent disclosure, and adolescent depressive symptoms: A longitudinal examination. Journal of Youth and Adolescence, 40(7), 902–915. doi:10.1007/s10964-010-9604-8 Henricson, C., & Roker, D. (2000). Support for the parents of adolescents: A review. Journal of Adolescence, 23(6), 763–783. doi:10.1006/jado.2000.0358 Holt, M., & Espelage, D. (2005). Social support as a moderator between dating violence victimiza- tion and depression/anxiety among African American and caucasian adolescents. School
- 34. Psychology Review, 34(3), 309–328. Hunt, T. K., Caldwell, C. H., & Assari, S. (2015). Family economic stress, quality of paternal relationship, and depressive symptoms among African American adolescent fathers. Journal of Child and Family Studies, 24(10), 3067–3078. doi:10.1007/s10826-015-0112-z Hurd, N. M., Stoddard, S. A., & Zimmerman, M. A. (2013). Neighborhoods, social support, and African American adolescents’ mental health outcomes: A multilevel path analysis. Child Development, 84(3), 858–874. doi:10.1111/cdev.2013.84.issue- 3 Jackson, J. M., Seth, P., Diclemente, R. J., & Lin, A. (2015). Association of depressive symptoms and substance use with risky sexual behavior and sexually transmitted infections among African 506 A. T. ESTREET ET AL. http://dx.doi.org/10.1016/j.jad.2014.08.006 http://dx.doi.org/10.1007/s10826-016-0386-9 http://dx.doi.org/10.1007/s10826-016-0386-9 http://dx.doi.org/10.1007/s10964-015-0301-5 https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1- 2014/NSDUH-FRR1-2014.htm https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1- 2014/NSDUH-FRR1-2014.htm https://www.samhsa.gov/data/sites/default/files/NS DUH-FFR1- 2015/NSDUH-FFR1-2015/NSDUH-FFR1-2015.htm https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR1- 2015/NSDUH-FFR1-2015/NSDUH-FFR1-2015.htm http://dx.doi.org/10.1093/swr/svs026
- 35. http://dx.doi.org/10.1080/15374410701444306 http://dx.doi.org/10.1080/15374410701444306 http://dx.doi.org/10.1037/a0035199 http://dx.doi.org/10.1007/s10826-012-9608-4 https://www.icpsr.umich.edu/icpsrweb/ICPSR/studies/6542 http://dx.doi.org/10.1007/s10964-014-0112-0 http://dx.doi.org/10.1037/0012-1649.43.2.522 http://dx.doi.org/10.1007/s10964-010-9604-8 http://dx.doi.org/10.1006/jado.2000.0358 http://dx.doi.org/10.1007/s10826-015-0112-z http://dx.doi.org/10.1111/cdev.2013.84.issue-3 American female adolescents seeking sexual health care. American Journal of Public Health, 105 (10), 2137–2142. doi:10.2105/ajph.2014.302493 Lamborn, S., Mounts, N., Steinberg, L., & Dornbusch, S. (1991). Patterns of competence and adjustment among adolescents from authoritative, authoritarian, indulgent, and neglectful homes. Child Development, 62(5), 1049–1065. doi:10.2307/1131151 Lindsey, M., Joe, S., & Nebbitt, V. (2010). Family matters: The role of mental health stigma and social support on depressive symptoms and subsequent help seeking among African American boys. Journal of Black Psychology, 36(4), 458–482. doi:10.1177/0095798409355796 Lombe, M., Nebbitt, V. E., Chu, Y., Saltzman, L., & Tirmazi, T. (2017). Household adversity and food security: The case of youth in public housing neighborhoods. Journal of Children and Poverty, 23(2), 1–16. doi:10.1080/10796126.2017.1288610
- 36. Lombe, M., Nebbitt, V. E., Sinha, A., & Reynolds, A. (2016). Examining effects of food insecurity and food choices on health outcomes in households in poverty. Social Work In Health Care, 55 (6), 440–460. Lopez, C. M., Andrews, A. R., III, Chisolm, A. M., De Arellano, M. A., Saunders, B., & Kilpatrick, D. G. (2017). Racial/ethnic differences in trauma exposure and mental health disorders in adoles- cents. Cultural Diversity and Ehnic Minority Psychology, 23(3), 382. doi:10.1037/cdp0000126 Matlin, S. L., Molock, S. D., & Tebes, J. K. (2011). Suicidality and depression among African American adolescents: The role of family and peer support and community connectedness. American Journal of Orthopsychiatry, 81(1), 108–117. Matlin, S. L., Molock, S. D., & Tebes, J. K. (2011). Suicidality and depression among African American adolescents: The role of family and peer support and community connectedness. American Journal of Orthopsychiatry, 81(1), 108. doi:10.1111/j.1939-0025.2010.01078.x Maughan, B., Collishaw, S., & Stringaris, A. (2013). Depression in Childhood and Adolescence. Journal of Canadian Academy of Child & Adolescent Psychiatry, 22(1), 30–35. McMahon, S. D., Coker, C., & Parnes, A. L. (2013). Environmental stressors, social support, and internalizing symptoms among African American youth. Journal of Community Psychology, 41
- 37. (5), 615–630. doi:10.1002/jcop.21560 Meadows, S. O. (2007). Evidence of parallel pathways: Gender similarity in the impact of social support on adolescent depression and delinquency. Social Forces, 85(3), 1143–1167. doi:10.1353/ sof.2007.0048 Nebbitt, V. (2009). Self-efficacy in African American adolescent males living in urban public housing. Journal of Black Psychology, 35(3), 295–316. doi:10.1177/0095798409333616 Nebbitt, V., & Lombe, M. (2007). Environmental correlates of depressive symptoms among African American adolescents living in public housing. Journal of Human Behavior in the Social Environment, 15, (2/3). doi:10.1300/J137v15n02_24 Nebbitt, V. E. (2015). Adolescents in public housing: Addressing psychological and behavioral health. New York, NY: Columbia University Press. Nebbitt, V. E., Lombe, M., & Lindsey, M. A. (2007). Perceived parental behavior and peer affilia- tions among Urban African American adolescents. Social Work Research, 31(3), 163–169. doi:10.1093/swr/31.3.163 Nebbitt, V. E., Sanders-Phillips, K., & Rawlings, L. R. (2015). An integrated model of adolescent development in public housing neighborhoods. Adolescents i n Public Housing. doi:10.7312/ columbia/9780231148580.003.0003 Nebbitt, V. E., Williams, J. H., Lombe, M., McCoy, H., &
- 38. Stephens, J. (2014). Descriptive analysis of individual and community factors among African American youths in urban public housing. Social Work, 59(3), 231–241. doi:10.1093/sw/swu024 Ofonedu, M. E., Percy, W. H., Harris-Britt, A., & Belcher, H. M. (2012). Depression in inner city African American youth: A phenomenological study. Journal of Child and Family Studies, 22(1), 96–106. doi:10.1007/s10826-012-9583-3 Okwumabua, J. O., Okwumabua, T. M., & Wong, S. P. (2014). Anger expression mode, depressive symptoms, hopelessness, and decision coping among African American adoles- cents. Journal of Human Behavior in the Social Environment, 24(6), 666–677. doi:10.1080/ 10911359.2014.922813 JOURNAL OF HUMAN BEHAVIOR IN THE SOCIAL ENVIRONMENT 507 http://dx.doi.org/10.2105/ajph.2014.302493 http://dx.doi.org/10.2307/1131151 http://dx.doi.org/10.1177/0095798409355796 http://dx.doi.org/10.1080/10796126.2017.1288610 http://dx.doi.org/10.1037/cdp0000126 http://dx.doi.org/10.1111/j.1939-0025.2010.01078.x http://dx.doi.org/10.1002/jcop.21560 http://dx.doi.org/10.1353/sof.2007.0048 http://dx.doi.org/10.1353/sof.2007.0048 http://dx.doi.org/10.1177/0095798409333616 http://dx.doi.org/10.1300/J137v15n02_24 http://dx.doi.org/10.1093/swr/31.3.163 http://dx.doi.org/10.7312/columbia/9780231148580.003.0003 http://dx.doi.org/10.7312/columbia/9780231148580.003.0003
- 39. http://dx.doi.org/10.1093/sw/swu024 http://dx.doi.org/10.1007/s10826-012-9583-3 http://dx.doi.org/10.1080/10911359.2014.922813 http://dx.doi.org/10.1080/10911359.2014.922813 Respress, B. N., Morris, D. L., Gary, F. A., Lewin, L. C., & Francis, S. A. (2013). Social determinants of adolescent depression: An examination of racial differences. Issues in Mental Health Nursing, 34(7), 539–549. doi:10.3109/01612840.2012.758206 Sagrestano, L. M., Paikoff, R. L., Holmbeck, G. N., & Fendrich, M. (2003). A longitudinal examina- tion of familial risk factors for depression among inner-city African American adolescents. Journal of Family Psychology, 17(1), 108–120. doi:10.1037/0893-3200.17.1.108 Schraedley, P. K., Gotlib, I. H., & Hayward, C. (1999). Gender differences in correlates of depressive symptoms in adolescents. Journal of Adolescent Health, 25(2), 98–108. doi:10.1016/S1054-139X (99)00038-5 Shaffer, A., Forehand, R., & Kotchick, B. (2002). A longitudinal examination of correlates of depressive symptoms among inner-city African-American children and adolescents. Journal of Child and Family Studies, 11(2), 151–164. doi:10.1023/A:1015121424404 Stockings, E., Degenhardt, L., Lee, Y. Y., Mihalopoulos, C., Liu, A., Hobbs, M., & Patton, G. (2015). Symptom screening scales for detecting major depressive disorder in children and adolescents: A
- 40. systematic review and meta-analysis of reliability, validity and diagnostic utility. Journal of Affective Disorders, 174, 447–463. doi:10.1016/j.jad.2014.11.061 Tandon, D. S., & Solomon, B. S. (2009). Risk and protective factors for depressive symptoms in urban African American adolescents. Youth & Society, 41(1), 80–99. Tandon, D. S., & Solomon, B. S. (2010). Risk and protective factors for depressive symptoms in urban African American adolescents. Youth and Society, 41(1), 80–99. doi:10.1177/ 0044118X08327520 Taylor, R. D., Budescu, M., & Gebre, A. (2016). Distressing mother-adolescent relations and psycho- logical wellbeing in low income African American families: Moderating effects of demanding kin relations. Journal of Child and Family Studies, 25(2), 678–690. doi:10.1007/s10826-015-0252-1 Taylor, R. D., Budescu, M., Gebre, A., & Hodzic, I. (2014). Family financial pressure and maternal and adolescent socioemotional adjustment: Moderating effects of kin social support in low income African American families. Journal of Child and Family Studies, 23(2), 242–254. U.S. Census Bureau. (2010). U.S. census 2000. Retrieved from https://www.census.gov/main/www/ cen2000.html Yap, M. B., Pilkington, P. D., Ryan, S. M., & Jorm, A. F. (2014). Parental factors associated with
- 41. depression and anxiety in young people: A systematic review and meta-analysis. Journal of Affective Disorders, 156, 8–23. doi:10.1016/j.jad.2013.11.007 Yip, T. (2015). The effects of ethnic/racial discrimination and sleep quality on depressive symptoms and self-esteem trajectories among diverse adolescents. Journal of Youth and Adolescence, 44(2), 419–430. doi:10.1007/s10964-014-0123-x Zimmerman, M. A., Ramirez0-Valles, J., Zapert, K. M., & Maton, K. I. (2000). A longitudinal study of stress-buffering effects for urban African American male adolescent problem behaviors and mental health. Journal of Community Psychology, 28(1), 17–33. doi:10.1002/(SICI)1520-6629 (200001)28:1<17::AID-JCOP4>3.0.CO;2-I 508 A. T. ESTREET ET AL. http://dx.doi.org/10.3109/01612840.2012.758206 http://dx.doi.org/10.1037/0893-3200.17.1.108 http://dx.doi.org/10.1016/S1054-139X(99)00038-5 http://dx.doi.org/10.1016/S1054-139X(99)00038-5 http://dx.doi.org/10.1023/A:1015121424404 http://dx.doi.org/10.1016/j.jad.2014.11.061 http://dx.doi.org/10.1177/0044118X08327520 http://dx.doi.org/10.1177/0044118X08327520 http://dx.doi.org/10.1007/s10826-015-0252-1 https://www.census.gov/main/www/cen2000.html https://www.census.gov/main/www/cen2000.html http://dx.doi.org/10.1016/j.jad.2013.11.007 http://dx.doi.org/10.1007/s10964-014-0123-x http://dx.doi.org/10.1002/(SICI)1520- 6629(200001)28:1%3C17::AID-JCOP4%3E3.0.CO;2-I http://dx.doi.org/10.1002/(SICI)1520-
- 42. 6629(200001)28:1%3C17::AID-JCOP4%3E3.0.CO;2-I Copyright of Journal of Human Behavior in the Social Environment is the property of Taylor & Francis Ltd and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. 1Clini C, et al. BMJ Open 2019;9:e025465. doi:10.1136/bmjopen-2018-025465 Open access Assessing the impact of artistic and cultural activities on the health and well-being of forcibly displaced people using participatory action research Clelia Clini,1 Linda J M Thomson,2 Helen J Chatterjee2 To cite: Clini C, Thomson LJM, Chatterjee HJ. Assessing the impact of artistic and cultural activities on the health and well-being of forcibly displaced people using participatory action research. BMJ Open 2019;9:e025465. doi:10.1136/ bmjopen-2018-025465
- 43. ► Prepublication history for this paper is available online. To view these files please visit the journal online (http:// dx. doi. org/ 10. 1136/ bmjopen- 2018- 025465). Received 18 July 2018 Revised 14 December 2018 Accepted 17 December 2018 1Institute for Media and Creative Industries, Loughborough University London, London, UK 2Genetics, Evolution and Environment, UCL Biosciences, University College London, London, UK Correspondence to Professor Helen J Chatterjee; h. [email protected] ucl. ac. uk Research © Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ. AbstrACt Objective Drawing on a growing body of research suggesting that taking part in artistic and cultural activities benefits health and well-being, the objective was to develop a participatory action research (PAR) method for assessing the impact of arts interventions on
- 44. forcibly displaced people, and identify themes concerning perceived benefits of such programmes. Design A collaborative study following PAR principles of observation, focus groups and in-depth semistructured interviews. setting London-based charity working with asylum seekers and refugees. Participants An opportunity sample (n=31; 6 males) participated in focus groups comprising refugees/asylum seekers (n=12; 2 males), volunteers (n=4; 1 males) and charity staff (n=15; 3 males). A subset of these (n=17; 3 males) participated in interviews comprising refugees/ asylum seekers (n=7; 1 males), volunteers (n=7; 1 males) and charity staff (n=3; 1 males). results Focus group findings showed that participants articulated the impact of creative activities around three main themes: skills, social engagement and personal emotions that were explored during in-depth interviews. Thematic analysis of interviews was conducted in NVivo 11 and findings showed that artistic and cultural activities impacted positively by helping participants find a voice, create support networks and learn practical skills useful in the labour market. Conclusions The study expanded on arts and well-being research by exploring effects of cultural and creative activities on the psychosocial well-being of refugees and asylum seekers. By focusing on the relationship between arts, well-being and forced displacement, the study was instrumental in actively trying to change the narrative surrounding refugees and asylum seekers, often depicted in negative terms in the public sphere. IntrODuCtIOn The recent All-Party Parliamentary Group on Arts Health and Well-being Inquiry Report shows a growing acknowledgement of the
- 45. impact of arts and creative practices, stating ‘arts engagement has a beneficial effect upon health and wellbeing and therefore has a vital part to play in the public health arena’ (APPGAHW, p11).1 Consensus among prac- titioners defines well-being as ‘the dynamic process that gives people a sense of how their lives are going through the interac- tion between their circumstances, activi- ties and psychological resources or mental capital’ (NEF, p3).2 Rather than depending on a single factor, well-being is seen as the result of interplay between different elements, distinguishing personal well-being (positive emotion, life satisfaction, vitality, resilience and self-esteem) from social well- being (supportive relationships, trust and belonging).3 Other authors emphasise ‘resil- ience and flourishing, rather than just surv iving’ (Ander et al, p243),4 a crucial point when investigating the situation of forc- ibly displaced people who often survive in extreme conditions and whose experience is often discussed in terms of dehumanisa- tion.5 6 Research conducted in the field of forced displacement and mental health shows that ‘asylum seekers and displaced people report high rates of pre-migration trauma’ (Vaughan-Williams, p275),6 and typically display significant levels of depression, anxiety, posttraumatic stress disorder (PTSD) and non-affective psychoses.7–11 Refugees and asylum seekers often encounter postmigra-
- 46. tion living difficulties, such as socioeconomic disadvantage, employment barriers, social and emotional isolation, racism and hostility, strengths and limitations of this study ► Focus on collaborative research. ► Different cultural and artistic activities studied. ► Researcher spent 5 months in research setting. ► Greater number of female than male participants. ► Focus groups attracted relatively low numbers of refugees/asylum seekers. o n M a y 1 9 , 2 0 2 2 b y g u e st. P ro te
- 48. e n : first p u b lish e d a s 1 0 .1 1 3 6 /b m jo p e n -2 0 1
- 50. d e d fro m http://bmjopen.bmj.com/ http://dx.doi.org/10.1136/bmjopen-2018-025465 http://dx.doi.org/10.1136/bmjopen-2018-025465 http://dx.doi.org/10.1136/bmjopen-2018-025465 http://crossmark.crossref.org/dialog/?doi=10.1136/bmjopen- 2018-025465&domain=pdf&date_stamp=2019-04-04 http://bmjopen.bmj.com/ 2 Clini C, et al. BMJ Open 2019;9:e025465. doi:10.1136/bmjopen-2018-025465 Open access experience of detention and uncertainty related to the asylum application process.7–9 12 If, as authors suggest,13–17 there is a strong link between mental health and socioeco- nomic conditions in terms of employability, income and housing, then the mental health of unemployed asylum seekers living on low incomes in poor quality housing is likely to be worse than that of the general population. Arts-and-health practitioners believe that ‘aesthetics act upon our senses to make us feel more, hear more and see more than we otherwise might… feelings are intertwined with mental, physical, spiritual and social health’ (Prior, p4).18 Several studies explored the relationship between arts, health and well-being and a growing body of evidence
- 51. suggests that cultural participation (including music, art making, theatre, dance, museum and heritage activities) enhances human health and well-being.1 19–27 Research conducted in museums-and-health, for example, suggests that ‘museum and art gallery encounters can help with a range of health issues, enhance wellbeing, and build social capital and resilience’ (Chatterjee and Noble, p286).27 According to research conducted in Norway with over 50 000 adults,28 participation in both receptive/ passive and creative/active cultural activities was signifi- cantly associated with good health, life satisfaction, and low anxiety and depression. Findings demonstrated how manual creative practices such as knitting had a positive impact on people suffering from depression and posttrau- matic stress disorder because ‘the movements involved in knitting are bilateral, rhythmic, repetitive, and auto- matic’ (Cuypers et al, p40).28 The authors attributed the positive mood of knitters to enhanced production of serotonin resulting from repeated movements, and that bilateral processes appeared to engage brain capacity and facilitate a meditative-like state more readily than unilateral ones. Although creative activities are seen to provide major benefits for refugees and asylum seekers, researchers have become ‘increasingly conscious of the value of recording and analysing what has been happenin g’ (Robjant et al, p1).8 The current study was conducted in the light of mental health and arts-in-health/museums-in-health evidence, and the large number of organisations that engage migrants, refugees and asylum seekers in the arts, with nearly 200 of these in the UK.29 The current research was conducted at the Helen Bamber Founda- tion (HBF), a charity offering support to refugees and asylum seekers as victims of torture and human rights violations. HBF adopts a holistic approach to support
- 52. its clients that includes cultural activities within a three- phase model of integrated care comprising stabilisation (medical and legal support), intervention (trauma-fo- cussed therapy and general psychological care) and inte- gration (attending the creative, computing and English classes, and interacting with other clients). The model is based on the needs of refugee/asylum seekers who often require assistance on several fronts (eg, psychological support might not be effective if a person does not have a place to sleep or lives in a dangerous situation, though giving people a place to sleep is not enough to overcome trauma). Their creative arts programme (CAP) led by volunteers includes art (painting and drawing), photog- raphy, textiles (dressmaking and knitting) and singing, and is attended by c.100 clients. The study took the view that arts participation would enhance the sense of wel l- being by allowing participants to form meaningful rela- tionships based on trust and mutual support (improving social well-being) and enhance self-esteem and self-confi- dence (increasing personal well-being). To provide voice and agency for participants, the study used a collaborative approach to explore client experi - ences of creative activities with HBF clients, staff and volunteers acting as coresearchers. The research was operationalised according to the principles of partic- ipatory action research (PAR)30 31 as a ‘way of opening up space for dialogue and conversation’ (Nicolaidis and Raymaker, p28),32 aiming to ‘understand and also improve a particular situation’ ,32 both pertinent aspects when working with displaced people. The PAR approach encourages an active contribution in the production of knowledge within a collaborative framework, empha- sising ‘equal partnerships’ (Daykin and Stickley, p167),33 and the ‘role of the participant in the design, implemen-
- 53. tation, and dissemination of the research’ (Vaughn and Jacquez, p78).34 The collaborative character of PAR is grounded in efforts to ‘democratise the research process’ (Blumenthal, p3),35 so ‘equal weight and consideration is given to the contributions of both the community and academic partners’ (Braun and Clarke, p170)36 again valuable for everyone involved but specifically refugees/ asylum seekers. One of the pillars of PAR, especially when community-based is ownership.37 By offering equal weight to client contributions focusing on the relationship between forced displace- ment and arts participation, the study aimed to empower participants by developing their sense of ownership in the project. Through collaborative working between the charity, displaced people and academics, the purpose of the research was to codevelop a methodological approach to address the needs of refugees/asylum seekers and to coproduce interview questions that could be applied in the UK and international settings. The objectives were to expand on arts-in-health and collab- orative research approaches by exploring the benefits of engagement in cultural and creative activities on the health and well-being of forcibly displaced people and contribute to the current debate on migration and public health. MethOD Design Qualitative research conducted comprised observation, focus groups and one-to-one semistructured interviews with clients, volunteers and staff as coresearchers within a collaborative PAR approach.38 o n
- 54. M a y 1 9 , 2 0 2 2 b y g u e st. P ro te cte d b y co p yrig h t. h ttp
- 55. ://b m jo p e n .b m j.co m / B M J O p e n : first p u b lish e d a s 1
- 57. F e b ru a ry 2 0 1 9 . D o w n lo a d e d fro m http://bmjopen.bmj.com/ 3Clini C, et al. BMJ Open 2019;9:e025465. doi:10.1136/bmjopen-2018-025465 Open access
- 58. Participants The study recruited an opportunity sample of volunteer participants through information leaflets and contact details in reception. Clients were approached by the researcher using two recruitment criteria: (i) clients had received therapy for at least 2 years prior to the research and had entered the integration stage of the model of integrated care; this meant that though still vulnerable, clients had established a therapeutic relationship of trust enabling them to form safe relationships in the wider community and move forward with their lives; and (ii) they had attended at least one of four CAP groups (art, photography, singing and textiles) for around 2 years. All participants spoke English sufficiently well to partic- ipate having attended English classes for about 2 years as part of integrated care. In total, 31 (6 males) partic- ipants volunteered for the study and attended focus group comprising 12 (2 males) refugees/asylum seekers, 4 (1 males) volunteers and 15 (3 males) charity staff. Of these, 17 (3 males) participated in interviews comprising 7 (1 males) refugees/asylum seekers, 7 (1 males) volun- teers and 3 (1 males) staff. Patient and public involvement HBF staff were instrumental in the application for research funding and collaborated with the researcher to deter- mine the study’s objectives. HBF clients were involved in the recruitment process by recommending that other clients join them in the research, though the researcher ensured that they matched recruitment criteria (above). In keeping with PAR, research questions and outcome measures concerning the effects of cultural and creative activities on the psychosocial well-being of refugees/ asylum seekers were determined by coresearchers (HFB clients, volunteers and staff) with differing involvement
- 59. depending on their role at the charity. Focus groups and interviews gave voice to clients’ priorities and preferences but, due to their vulnerability, no personal information was requested as the process of remembering could have been difficult.7 10 Although some participants mentioned personal issues and experiences, they were not encouraged to do so. Data generated by coresearcher involvement in the research collaboration informed focus groups, in turn focus group outcomes led to the development of ques- tions for the in-depth interviews to follow. In addition to participation in focus groups and interviews, a core group of seven coresearchers (three clients, two volunteers, two staff, with one male per category) were involved in design of the interview guides, discussion of emerging themes and dissemination of the research findings to other partic- ipants for verification and comments, in accordance with PAR principles.33 The results of the research were fed back to everyone involved with HBF through ongoing commu- nication with the researcher, an internal report lodged at the charity, and an end-of-project event. Data collection Data collection carried out by the location-based researcher consisted of three stages: stage 1 (months 1–2) participant observation; stage 2 (months 3–4) focus groups and stage 3 (month 5) semistructured interviews. In stage 1, participant observation was used as a starting point ‘for studying how organisations work, the roles played by different staff and the interaction between staff and clients’ (Pope et al, p32).38 The researcher attended creative classes for clients and spent a day a week working from HBF (12–15 hours per week) to determine the nature of focus groups. In stage 2, four focus groups were held, first and final with clients (n=8, n=4, respec- tively), second with volunteers (n=4), and third with staff
- 60. (n=15). In the focus groups, participants were asked to discuss research questions (box 1) involving ways of gath- ering information on the impact of creative activities, and reasons for attending groups (or in the case of volunteers and staff, reasons for involvement). All focus groups were organised informally to facilitate development of discus- sion among participants and allow an exchange of experi - ences and ideas. Ideas that emerged during focus groups laid the basis for first drafts of interview questions, tailored to clients, volunteers or staff (box 2). In line with the collaborative ethos, drafts were circulated to receive feed- back from coresearchers prior to the interview stage, and volunteers and staff were consulted and asked to provide comments and suggestions for interview questions. For stage 3, clients (n=7), volunteers (n=7) and staff (n=3) participated in interviews with the researcher using a semistructured format to allow free expression within the research constraints and limit potential research bias.30 39 Data analysis A first informal thematic analysis was conducted by the researcher while writing field notes consisting of a chronicle of descriptive rather than analytic events both observed and provided by coresearchers as the ‘raw mate- rial of the research’ (Kemmis et al, p38).30 The process box 1 Focus group questions Clients 1. Why do you like the Helen Bamber Foundation (HBF) creative arts programme? 2. How would you gather information or evidence about the benefits
- 61. of artistic activities? 3. Which creative arts classes have a positive impact on the lives of refugees? Circle the option(s) that you think work best or add another one. Arts and Crafts Drawing Films Knitting Photography Singing Textiles. Volunteers 1. Why do you volunteer at the HBF? 2. How do you think your group benefits clients? 3. How would you collect evidence on the effects of participating in artistic activities? staff 1. Why do you recommend clients to attend creative arts groups? 2. What do you think are the benefits of attending arts groups? 3. How would you collect evidence on the effects of participating in artistic activities? o n M a y 1 9 , 2 0
- 62. 2 2 b y g u e st. P ro te cte d b y co p yrig h t. h ttp ://b m jo p e n .b
- 63. m j.co m / B M J O p e n : first p u b lish e d a s 1 0 .1 1 3 6 /b
- 65. 0 1 9 . D o w n lo a d e d fro m http://bmjopen.bmj.com/ 4 Clini C, et al. BMJ Open 2019;9:e025465. doi:10.1136/bmjopen-2018-025465 Open access of transcribing notes was used to identify key points connected to the research question. This preliminary analysis informed focus group topics where points were discussed more in detail. After the first round of focus groups, all notes were compiled into a word document and repeatedly read by the researcher and coresearchers to search for recurring topics and themes. Thematic analysis of focus group outcomes were explored in detail
- 66. during interviews. All interviews were recorded and transcribed to become familiar with the data and begin the coding process.37 All details in the transcripts were recorded verbatim (eg, sighs, laughter, silences and tears) as their exclusion could have changed the meaning expressed.30 Transcriptions were uploaded into NVivo11 box 2 Interview questions Clients 1. How long have you been attending the creative arts programme (CAP) classes for? 2. Which groups do you attend? 3. Why did you choose this/these groups(s)? 4. What do you like the most about these groups? 5. Is there anything about the groups that you find difficult? 6. Anything you would like to change? 7. Is there a group you prefer? Which one? Why? 8. How do you feel when you attend this group? 9. Do you think there are benefits of attending these groups? If so what are they? 10. During our previous meeting, it emerged that participants feel that groups allow them to learn new or improve already acquired skills. Do you agree? Have you learnt any new skill? And what do you think about the possibility of learning new skills? (How does that impact your life?) 11. Another element which emerged during our meeting is that
- 67. people enjoy the social aspect of these groups: meeting people and finding new friends. What do you think about this? [supporting questions: do you like being around other people? Why? What happens when you attend a session? Have you made new friends? How do you feel about that?] 12. Among all of the reasons why you enjoy attending the creative arts group, which one is the one that you feel strongest about? 13. Why do you keep attending? 14. If you could compare the way you were feeling before joining any of these activities and the way you feel now, would you say you feel any different? Explain. 15. Creative activities of course are part of the support that Helen Bamber Foundation (HBF) offers to its clients. Do you think that you would feel the same about yourself today even without attending these creative activities groups? Why? 16. Do you think that taking part in these creative activities has had any influence on the way you see yourself? And the way you see yourself in London? 17. If you were to recommend someone to join a group, what
- 68. would you say? Volunteers 1. What do you teach? 2. How long have you been volunteering for? 3. Why did you decide to volunteer? 4. How did you learn about the HBF? 5. What do you think your group offers clients? 6. What are the main challenges you face/have faced as a volunteer? 7. Do you find it difficult to engage clients in the activity you coordi- nate? What do you think clients like about the way you (and your colleagues) handle the sessions? Is there anything that clients do not like? 8. How would you describe a typical session? 9. What do you think people like the most about your group? 10. Do you ever discuss emotions with clients? Or their personal situation? 11. Look at the notion of well-being defined by NEF (New Economics Foundation): Well-being as ‘the dynamic process that gives people a sense of how their lives are going through the interaction between their circumstanc- es, activities and psychological resources or mental capital.’ (NEF 2008,
- 69. p3) Continued box 2 Continued According to the NEF, there are different components to well - being, such as: ‘Personal wellbeing (emotional wellbeing, satisfying life, vitality, resil- ience, self-esteem and positive functioning) and social wellbeing, in- cluding supporting relationships and trust and belonging.’ (NEF 2009) 12. Do you think that the activity you lead has any impact on the well-being of clients? Elaborate. 13. If you were asked to recruit people for your group, what would you say to convince them to join? 14. Would you use different words to promote your group with men and women? Why? 15. Do you think that your group makes a difference in the lives of clients? How? Why? 16. And what about your own life? What is the impact of your volunteer activity on your own life? staff
- 70. 1. How long have you been working at HBF for? 2. Why did you decide to work here? 3. What is your role? 4. As part of your work, do you have any direct contact with clients? 5. Could you say a few words on your relationship with clients? 6. How would you describe your own experience at HBF so far? 7. What are the main challenges that you face/have faced in your position? 8. Do you think that your own gender influences the ways in which clients relate to you? 9. In your position, do you discuss clients’ personal situations and feelings? 10. If so, do you think that the cultural background of clients affects the way in which you discuss emotions? If it does, how and why? 11. What are the main challenges of discussing emotions with clients? 12. Could you say a few words on the Model of Integrated Care? Do you think it works? And if so, why? 13. Do you recommend clients to attend any of the CAP groups? What do you say in this case? 14. What role do you think cultural and creative activities play in the
- 71. recovery of clients? 15. Are there any particular activities that, in your opinion, are more popular with clients? 16. Would you say that the programme makes a difference in the lives of clients? If yes, please elaborate. 17. Have you witnessed clients benefiting from their own participation in the creative arts programmes? If yes, in what ways? o n M a y 1 9 , 2 0 2 2 b y g u e st. P ro te
- 73. e n : first p u b lish e d a s 1 0 .1 1 3 6 /b m jo p e n -2 0 1
- 75. d e d fro m http://bmjopen.bmj.com/ 5Clini C, et al. BMJ Open 2019;9:e025465. doi:10.1136/bmjopen-2018-025465 Open access to produce nodes from coding-relevant concepts. NVivo’s word frequency query facilitated the search for keywords (including stem words and synonyms) grouped under the same theme. The text search query provided a compre- hensive analysis of data. After coding of data into initial themes,37 a review of themes followed to refine the analysis. results Focus groups Focus group data were analysed using thematic analysis (NVivo11). Findings showed consistenc y in the way all HBF participants (clients, volunteers and staff) articulated their reflections on the impact of creative activities. The benefits of creative activities were highlighted in clusters emerging from around three main overarching themes: ‘skills’, ‘social aspects/friendships’ and ‘mood-personal sphere’; the latter subdivided into ‘brain’ (creative thought processes), ‘routine’, self-expression’ and ‘confi- dence’. During focus groups, coresearchers were asked
- 76. to write answers to the questions posed, and a collective discussion followed. Clients responded consistently about benefits of the creative programmes. One client listed ‘Activities help my brain think about other stuff and keep me busy and relaxed. You can’t think about bad things. To learn more skills. I can use skills to help others’. Learning new or improving existing skills was a key theme emerging out of focus groups, as skill development appeared to change clients’ perceptions of their status; as a female volunteer at HBF for 2 years suggested ‘partici- pants do not feel assessed as clients, they are just learners or artists. These groups paved the way for identifications different from being a victim, a refugee or an asylum seeker’. Clients also mentioned how acquiring new skills was an important factor in improving self-esteem; one client wrote about attending CAP ‘Give me confidence. Make me feel good and useful. Change my mood. Learn new things and meet people. Improve my skills. Give me hope to lead a better life’. Learning new skills was a benefit connected to the second theme that emerged during focus groups, the social aspect. It allowed people to meet others in similar situations and create friendships and/or a support network; as a client wrote ‘Allows me to feel included. Safe environment. Improves my mood. Learn new skills. Gets me out of the house. Meet new people’. Staff too recognised the social aspect of activities as a major benefit, with one suggesting ‘in these groups, clients learn to have balanced, reciprocal relationships, which they have not experienced before or for a long time given their expe- rience of violence (trafficking). They provide clients with an alternative identity, that is, they are not simply victims here, they are learners, artists, dressmakers, etc.’ Similar themes emerged in the volunteer focus group
- 77. during which a relatively new male volunteer involved of 4 months was impressed by the solidarity between clients, emphasising the benefits of the ‘feeling of belonging to a group’ and ‘strong support that people receive from other members’. The third and final theme that emerged when discussing the benefits of CAP the mood-personal sphere. Staff commented on the mood enhancing benefits of CAP for people with PTSD; one staff member observed ‘creative activities allow clients to momentarily leave out their problems or memories, by focusing on a particular activity they cannot think about anything else’. The focus group with staff emphasised that being busy in the company of others allowed clients to feel safe and not to dwell on their own situation. In concentrating on learning new skills, clients blocked out (although for short periods) memories of the past. Importantly, responses illustrated that focus group participants perceived their involvement as beneficial at multiple and overlapping levels. Enhance- ment of mood appeared to derive from not only meeting new people, forging meaningful relationships and feeling part of a group but also connected to a growing self-con- fidence and self-esteem experienced as clients acquired new skills. Interviews During interviews, clients elaborated on practical and social skills, and commented on the positive effect of attendance on their mood and emotion: Practical skills: learning new practical skills or improving those previously learnt emerged strongly among asylum seekers without the right to work. As a client pointed out:
- 78. I have learned a lot of skills: I’ve learned sewing, now I’m learning art, I can do better, before I didn’t know how to draw a person, to mix colours, you know such things… so you keep on learning, slowly by slowly, then in the end you find yourself, you’re a profes- sional, so that is very great… to me… I like to come, always and attend, and listen to what they tell me, and I do it. Or, as another client explained: I’ve learned new skills […] and you can never waste your time learning new skills. New skills always help you in your life, always. So, everything I’ve learned will help me. You think like ‘film club, learning how to edit, etc.’. People pay people on YouTube to edit their films, and I’m, like, I could just do my own, if I wanted to have a YouTube channel, I can do my own. Skill improvement provided a sense of achievement and improved self-confidence, talking about learning new skills, one client observed: When you are in this situation it feels like life has, in a way, stopped. And you can’t do anything to change it. But by doing all this activity you feel, or I felt … it was like, you know, that I was learning something in my life, rather than just waiting.[…] For instance, if I go for a job somewhere, where you have to write what skills you have, so I could include all of this. I mean I o n M a
- 79. y 1 9 , 2 0 2 2 b y g u e st. P ro te cte d b y co p yrig h t. h ttp ://b m
- 80. jo p e n .b m j.co m / B M J O p e n : first p u b lish e d a s 1 0 .1
- 82. b ru a ry 2 0 1 9 . D o w n lo a d e d fro m http://bmjopen.bmj.com/ 6 Clini C, et al. BMJ Open 2019;9:e025465. doi:10.1136/bmjopen-2018-025465 Open access don’t have a certificate or, like, proper qualifications, but I’ve all those skills, so I feel like, it is, in a way,
- 83. impressive? Because you feel like, you know, rather than just waiting and not doing anything, you have been learning. The sense of self-improvement associated with learning skills was linked to the perception that by learning, clients were preparing themselves for a new life when they would be allowed to live and work in the UK, countering the perception that life for them had stopped and giving them something to look forward to. The process of skills learning was not simply a vertical one; peer learning was equally important, stressing the importance of social aspects. Social skills: the opportunity to overcome social isola- tion and create a social network emerged as one of the benefits of creative engagement. As one client indicated: The groups changed me because you know when I come, I feel lonely and doesn’t have anybody. I was lonely I don’t even know whether there will be a home from morning to live in. But when I started coming these groups, I told you I feel active, I feel coming to see people, that I speak to. I don’t even know how to communicate with people before. I told you because of my coming here I now feel to communicate to peo- ple. Before I never communicate to people, I don’t know how to do it. And I don’t know how to play with people. But these groups make me now taught me: play with people, to meet me. The client expressed the difficulties of establishing new relationships and the feeling that the group was a place in which they could regain this ability to connect with other people. The social aspect was an important point reiterated in all interviews; fellow clients were described
- 84. as ‘friends’ but also as ‘brothers and sisters’. Arts activities allowed clients to create a community characterised by solidarity, as one client explained: If you’re in a situation where you’ve been completely isolated from people for a while and you just don’t know who to trust, or to be around people, it’s one of those spaces where you can get to meet people, socialise, and actually make friends.[…] And these friendships do last. A life-time, because you under- stand what the person has gone through, you don’t have to explain a lot, you know, they just know that you’ve been through something terrible.[…] So, it’s easier when you have people here who just under- stand what you’ve possibly been through. This remark connects with the observation that ‘engage- ment in participative creative arts activities in communi - ties can help to build social capital, address loneliness and social isolation, and build personal confidence and a sense of empowerment’ (Staricoff, p32).25 The awareness of experiencing similar situations makes clients feel free to share their own experiences with one another but also not to, if they did not feel like opening up: There is a sense of community: you know you go there, you know there are people like you in the same situation you’re not going to be judged, so it’s that sense of community: we know what’s going on, we don’t have to talk about it.[…] It’s a distraction from immigration and we know we are all going through it, but we don’t have to talk about it. There are other things going on in life, and we talked about, for ex- ample in the art group, the works we produced and what we could do, what we could achieve and get in-
- 85. spired by each other’s work. Again, this remark introduced the third broad theme which emerged out of the interview analysis, which was the impact of creative arts on personal mood and emotion. Mood and emotion: learning or improving skills while forging long-lasting relationships in a context of deep social isolation (outside of HBF), inevitably had a substantial impact on mood and emotion. In discussing this aspect of creative arts, interviewees focused particu- larly on how groups allowed them to have a routine, a ‘luxury’ one client said ‘when you can’t do nothing but waiting for the government to decide on your right to stay in the country’. Routine combined with skills learning/ improving was thought to have a positive impact on clients’ mental health; ‘having something to do’ and ‘something to look forward to’ were recurrent expres- sions during interviews. As one client noted: I used to come here every day of my life: Monday, Tuesday, Wednesday… because I don’t have anywhere to go, so I just come here, and I attached myself to the groups, we met, we talk, we… then I’ve gone to knit, I’ve gone to do computer, reading, many things I learnt here, so I just like it. Another client elaborated further: It’s something that I look forward to. One thing you have to bear in mind is that I am not working, and I am not studying, you know, so it was the only thing that I would look forward to because it was something to do, otherwise I would just be at home, doing noth- ing, you know, feeling very sorry for myself, getting upset all the time. I mean I still feel that way but at
- 86. least there’s something to look forward to, when you don’t have hope or something to look forward to, it increases your depression levels, so for me it’s helped me greatly. This statement describes the social and emotional isolation as part of postmigration living difficulties. The routine of classes, together with an awareness that others in similar situations would attend, provided comfort to clients, countering feelings of isolation: There is nothing else for you and it’s also a way of, like, using your time wisely, ‘cause at the end of the o n M a y 1 9 , 2 0 2 2 b y g u e st. P ro
- 88. e n : first p u b lish e d a s 1 0 .1 1 3 6 /b m jo p e n -2 0 1
- 90. a d e d fro m http://bmjopen.bmj.com/ 7Clini C, et al. BMJ Open 2019;9:e025465. doi:10.1136/bmjopen-2018-025465 Open access day most of the time you’re just sitting down doing nothing, and doing nothing slowly begins to affect your mind, your brain, you know you become lazy, you know you literally are just in a four-squared room[…] The benefits of a routine were increased by inclusion of creative activities that according to clients and volunteers, had a positive impact on mood because they exercised the brain and allowed clients to find a new language to express themselves. As a client stated: [Attending creative groups] gives you a lot of confi- dence, you know. And it allows your brain to think outside of the box because I think we are just in that box and… but when you attend these classes, your mind, you know, opened and you learn new things and you want to then learn other things as well. This comment highlights an important link between
- 91. arts and feelings; as another stated: It is more of expressing, more of letting go, it’s like getting a spirit out of you, and you don’t have nec- essarily have to tell someone ‘I’ve done this because of that and that, and this’, you know. Because some- times you just don’t find the voice to talk about it and, I, as a person am really shy and, you know, I feel easily embarrassed, you know.[…] So… that’s why I’m into arts, yes I’m doing arts really. Clients agreed that the possibility of self-expressing without having to articulate their feelings, helped them grow emotionally and gain confidence. It was not only clients who benefited from CAP; findings also pointed to the positive impact on volunteers, a point stressed by all volunteers when discussing personal experiences. DIsCussIOn Creative and cultural activities were observed over a sustained period of 5 months. Clients participating in the activities had reached the integration stage of the model of integrated care consequently had been taking part in CAP activities for 2 plus years prior to the research. Activ- ities provided refugees and asylum seekers with new skills, including practical and technical skills, and social and life skills involving language acquisition obtained partly through informal peer learning and mutual support. Learning new skills contributed to the sense of well-being and empowerment experienced by HBF clients. The time spent by the researcher at the HBF was vital for familiari - sation with the context, getting to know people involved in the organisation and explaining the research to recruit participants from among clients, volunteers and staff. The fact that several clients attended more than one group per week (2–4) made it possible to forge trusting
- 92. relationships and recruit coresearchers, allowing them to feel comfortable in speaking their mind. A possible issue here was that the number of groups attended by clients was not accounted for, so it was not evident as to whether increased participation furthered benefits at a higher/ faster level. Once recruited, participants remained with the study in their coresearcher roles and continued to attend activities on a weekly basis for the 5 months (except for rare absences due to illness). Activities appeared to positively enhance mood and emotion both for clients and volunteers facilitating CAP groups. Although passive participation was not compared,28 active and creative participation in the groups specifically benefited the clients. A key reason was that asylum seeker status in the UK would not have permitted alternative occupation or employment, so clients might not have otherwise left their homes or met people on a regular basis. In keeping with previous research, participants reported that participation in cultural and social activities contributed to their social health,18 and aligned with a growing body of evidence1 to suggest that creative activities enhanced mental well - being,19–27 helping clients to develop self-confidence and resilience.21 Client preferences for activities indi - cated that singing was their favourite group, followed by photography, art and textiles. Singing was regarded as beneficial because it allowed people to meet socially and work collaboratively, aspects considered important in countering loneliness. Findings aligned with a recent qualitative study indicating that choral singing promoted improvements in social, emotional, physical and cogni- tive functioning and that benefits were experienced simi - larly irrespective of age, gender and nationality.40 In the current study, photography, art and textiles were praised
- 93. by clients for the skills taught and although social aspects were relevant, skills that allowed participants to continue activities at home (eg, sewing and drawing) were highly valued. Interviewed staff were asked to comment on the popularity of activities, and although the order was the same as that of clients, they were not asked their opinion on which were most beneficial. The current study bridged the gap between two research disciplines: arts-in-health and forced displacement and mental health. It contributed to existing literature by demonstrating beneficial effects of creative activities on the well-being of refugees/asylum seekers and showed that PAR was an appropriate and ‘democratic’ means of collaboration between displaced communities and academics (Bradbury, p3).39 In contrast with traditional research where ‘academics benefit from the research, but often the people involved hear very little if anything from the researcher again’ (Daykin and Stickley, p78),33 a core element of PAR is that research should be meaningful and have tangible outcomes for coresearchers as they work together to bring about significant change within their community or society at large. In the current study, client involvement in the research and their decision to organise a public exhibition to showcase their artwork was a means for them to interact with wider society and actively rewrite the narrative around asylum seekers and refugees, often depicted in negative terms in the public sphere.41 o n M a y 1
- 94. 9 , 2 0 2 2 b y g u e st. P ro te cte d b y co p yrig h t. h ttp ://b m jo
- 95. p e n .b m j.co m / B M J O p e n : first p u b lish e d a s 1 0 .1 1
- 97. ru a ry 2 0 1 9 . D o w n lo a d e d fro m http://bmjopen.bmj.com/ 8 Clini C, et al. BMJ Open 2019;9:e025465. doi:10.1136/bmjopen-2018-025465 Open access Adopting a PAR approach is important when working with immigrant communities as it ensures that the research question is of ‘genuine importance’ (Vaughn and Jacquez,