Focus on women's Health: the Pelvic floor and bladder2001

Pelvic floor and bladder health information and exercises for exercise teachers Functions of the Pelvic Floor The pelvic floor is the inferior and integral component of the abdominal wall. As such it forms an outlet for the pelvis for urination, defecation, enabling emptying of the bladder and bowel, and enables vaginal opening for childbirth. Contraction of the muscles enables the continence of urine and faeces. The pelvic floor also counteracts changes in abdominal pressure caused by coughing, sneezing, nose blowing, forced expiration and vomiting. Reflex activity enables rapid action when required. The conscious contraction of the pelvic floor can improve sexual enjoyment during penetrative sex. On the downside, some women experience involuntary excessive contraction of the pelvic floor prior to or during penetrative sex, prohibiting sexual intercourse, or making it very painful. This usually requires referral to specialist psychosexual services. A strong pelvic floor is also instrumental in preventing a ‘prolapse’. The muscles also support the contents of the pelvis and abdomen. Pelvic floor exercises are therefore a vital component of any fitness programme. Perhaps because results are not immediately evident, this area has, until recently, received comparatively little attention. One inhibiting factor for teachers may be the concept of naming the vagina, urethra and anus in a generally acceptable manner, and so the language and atmosphere for including the pelvic floor in a programme of exercise can make all the difference.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Focus on women's Health: the Pelvic floor and bladder2001
Similar to Focus on women's Health: the Pelvic floor and bladder2001 (20)
More from Barbara Hastings-Asatourian
More from Barbara Hastings-Asatourian (20)
Recently uploaded
Recently uploaded (20)
Focus on women's Health: the Pelvic floor and bladder2001
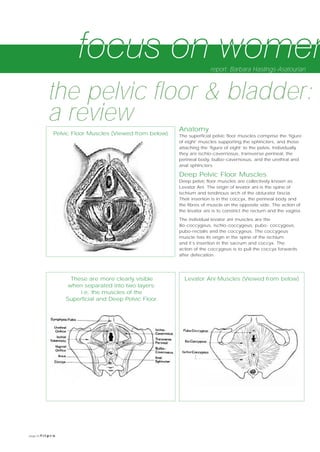
- 1. page 8 f i t p r o Anatomy The superficial pelvic floor muscles comprise the ‘figure of eight’ muscles supporting the sphincters, and those attaching the ‘figure of eight’ to the pelvis. Individually they are ischio-cavernosus, transverse perineal, the perineal body, bulbo-cavernosus, and the urethral and anal sphincters Deep Pelvic Floor Muscles Deep pelvic floor muscles are collectively known as Levator Ani. The origin of levator ani is the spine of ischium and tendinous arch of the obturator fascia. Their insertion is in the coccyx, the perineal body and the fibres of muscle on the opposite side. The action of the levator ani is to constrict the rectum and the vagina. The individual levator ani muscles are the ilio-coccygeus, ischio-coccygeus, pubo- coccygeus, pubo-rectalis and the coccygeus. The coccygeus muscle has its origin in the spine of the ischium and it’s insertion in the sacrum and coccyx. The action of the coccygeus is to pull the coccyx forwards after defecation. the pelvic floor & bladder: a review report: Barbara Hastings-Asatourian Pelvic Floor Muscles (Viewed from below) These are more clearly visible when separated into two layers: i.e. the muscles of the Superficial and Deep Pelvic Floor. Levator Ani Muscles (Viewed from below)
- 2. f i t p r o page 9 Functions of the Pelvic Floor The pelvic floor is the inferior and integral component of the abdominal wall. As such it forms an outlet for the pelvis for urination, defecation, enabling emptying of the bladder and bowel, and enables vaginal opening for childbirth. Contraction of the muscles enables the continence of urine and faeces. The pelvic floor also counteracts changes in abdominal pressure caused by coughing, sneezing, nose blowing, forced expiration and vomiting. Reflex activity enables rapid action when required. The conscious contraction of the pelvic floor can improve sexual enjoyment during penetrative sex. On the downside, some women experience involuntary excessive contraction of the pelvic floor prior to or during penetrative sex, prohibiting sexual intercourse, or making it very painful. This usually requires referral to specialist psychosexual services. A strong pelvic floor is also instrumental in preventing a ‘prolapse’. The muscles also support the contents of the pelvis and abdomen. Pelvic floor exercises are therefore a vital component of any fitness programme. Perhaps because results are not immediately evident, this area has, until recently, received comparatively little attention. One inhibiting factor for teachers may be the concept of naming the vagina, urethra and anus in a generally acceptable manner, and so the language and atmosphere for including the pelvic floor in a programme of exercise can make all the difference. A word of caution: all that goes wrong with the urinary system does not originate in the pelvic floor. Advice offered therefore needs to be considered in that context (Overstall and Castleden 1998) The Bladder The bladder is made up of three layers of smooth muscle called the detrusor. The urethra comprises both smooth and striated muscle. The smooth muscle is continuous with the detrusor. The first striated muscle fibres are slow twitch and are involved in maintaining continence at rest. The second striated muscle is the peri-urethral part of levator ani, which is separated from the external urethral sphincter. These are fast twitch and are involved in maintaining continence under stress. The mucosa of the urethra is lined by epithelium (skin cells). The structure of these epithelial cells is under the influence of oestrogen, and therefore changes throughout the lifecycle, particularly peri- and post-menopausally. Women approaching or experiencing the effects of the menopause may find it reassuring that their fitness leader is concerned about optimizing the function of the whole body, including the bladder and urethra at this time. Sometimes the problem is chronic urinary infection. But sometimes apparently urinary symptoms are in fact caused by vaginal or cervical infection. Some people have detrusor instability, others lose all bladder control after illness or injury (reflex bladder). People on diuretics (‘water tablets’) often complain of urge incontinence, and those who take too much caffeine, fizzy drinks and alcohol may get bladder irritation. Whilst the role of the fitness leader is not to diagnose, try to fix or assume any role for which they have insufficient training, there is still essentially practical advice the fitness leader could give at appropriate times that might save discomfort later. Urine tests carried out via the General Practitioner or NHS walk in clinic will quickly determine whether the problem is infection. Advice regarding sufficient fluid intake and avoidance of irritants for re-hydration can prevent considerable discomfort and complication. Demonstrating knowledge of the options available reinforces that the problem is important and should be taken seriously by early referral. Invariably, the earlier the treatment, the more likely it is to be successful. Stress incontinence There are several proposed theories of stress incontinence (Monger and Phillips, 2000): 1. Bladder Neck Hypermobility, where the neck of the bladder falls below the pelvic floor 2. Intrinsic Sphincter Deficiency, reduced urethral tone caused by neuromuscular or vascular insufficiency, for example from reduced oestrogen levels, radiotherapy or surgery. 3. Mid-urethral support: the hammock hypothesis Pubo-urethral ligaments support the pelvic fascia, which forms an aponeurotic plate over the urethra. These ligaments become continuous with the ligaments of the clitoris. The endopelvic fascia forms a fibrous band running from the pubis to the ischial spine. When there is a rise in intra-abdominal pressure, continence is maintained by compression of the urethra against the anterior vaginal wall and its endo-pelvic fascia. This is attached to the levator ani muscles. The levator ani muscles have slow-twitch fibres to maintain constant tone. At rest levator ani contract constantly, relaxing only during emptying of the bowel and bladder. This keeps the bladder neck in position at rest. Stress incontinence is brought on by apparently unrelated expulsive actions such as coughing, sneezing and laughing. It is only true stress incontinence if its origin is in a weakened or damaged pelvic floor, and therefore affects people physically, emotionally, socially and sexually. Barbara Hastings-Asatourian has had 26 years of experience since first achieving her Bachelor of Nursing from Manchester University. It’s now 21 years since she qualified as a midwife at Tameside General Hospital, nearly 10 years since she gained her teaching certificate from Huddersfield and began to work in Higher Education teaching nurses, and 5 years since she achieved her M.Sc. from Salford. Having since become a qualified exercise teacher, she has been teaching ‘Heart and Soul’ her own holistic balance of aerobic activity, mind/body conditioning and deep relaxation techniques.
- 3. possible. This is not impossible as the exercises can be performed anywhere and in any position: standing, sitting, lying, at work, during leisure time or during sex. Regular pelvic floor exercises as described above over a period of several weeks after childbirth should begin to have a positive effect in weeks. In the event of little or no improvement referral to a physiotherapist may be required and the addition of vaginal weights or cones may then be taught (Versi and Christmas 1998). If there is no improvement referral to urodynamics may then follow, to assess if this is true stress incontinence or detrusor muscle instability (Overstall & Castleden 1998). Detrusor instability responds to drug treatment, rather than pelvic floor exercises. Sometimes biofeedback at a specialist unit, using video helps women to identify and isolate contractions. Imaging techniques (ultrasound and MRI scanning) have also helped understanding. The problem may need to be resolved by uro-gynaecological surgery (Versi and Christmas 1998), for example if there is a ‘prolapse’, and if there is a weakness of the vaginal walls (rectocoele or cystocoele). Recovery from surgery may be another area where knowledge, information and a planned approach to collaborative care will improve the quality of clients’ recovery period. Finally the ‘information giving’ role for the fitness industry can be optimised through the gathering of resources such as self help groups, library resources, and web sites. This information can be posted on walls, noticeboards and Web sites, for maximum exposure. Three have been included below for future reference. References & Organisations The Continence Foundation has a telephone help-line (020 7831 9831) which provides information, leaflets, videos and a support network. Their Web site address is: www.continencefoundation.org.uk For a detailed reference and recommended reading list, send requests to Michelle Roberts, Publishing Manager at the Fitpro office. page 10 f i t p r o Causes •Hormonal changes (menstrual cycle, pregnancy, menopause) •Pregnancy and childbirth (a long labour, instrumental delivery e.g. forceps) •Prolonged immobility, where muscles are inactive and wastage occurs. •Obesity, (leading to an increase in pressure on the abdomen and its contents) Stress incontinence caused by pregnancy and childbirth Surveys carried out over the last 10 years (Mori 1993, Mayne 1995, Marshall 1996 cited in Woodham 1998) are in agreement that about a quarter of new mothers suffer from stress incontinence in the first 3 months of their baby’s life, for some (estimated at 15%) this continues well into the first year. Approximately 4% of new mothers suffer from faecal incontinence. True stress incontinence benefits from pelvic floor exercises, when they are performed regularly. The following is a routine that could be incorporated into any exercise programme. A simple leaflet of this information with diagrams will provide reinforcement to aid compliance with a regular daily programme. A Basic Pelvic Floor Exercise Routine • Sit, stand or lie with legs slightly apart. • Try to avoid clenching buttocks and thighs together as the pelvic floor requires isolating from the gluteal and adductor muscles (Isolation takes practice and may not happen at first). • Try to relax the abdominal muscles at first, to feel the difference between superficial and deep contractions. • Breathe in to prepare, then breathe out to begin contracting. • Pull up and close the urethra (front passage for urine) • Extend this contraction to include the vagina (middle passage) breathing normally, not holding the breath. • Extend this contraction to include the anal sphincter (back passage). Breathing normally, not holding the breath. • Then relax. • Alternatively, start by contracting back to front, to help isolate the sphincter muscles from behind. Using Visualisation Techniques 1.The Lift Visualising the pelvic floor on two levels, pull further upwards to the second floor to engage the deeper pelvic floor muscles. Then relax. 2.The Flower Visualise the openings of the pelvic floor like flowers influenced by sunlight. Imagine the pelvic floor tightening up like the head of a daisy at night, and then relax like a flower opening in the midday sun. To engage both fast and slow twitch fibres the routine should include slow and fast rhythmic contractions. Play with the timing. Do 5 slow then 10 fast. Build up the number and frequency, and then build into daily routine (for life). Practise with different terminology until it becomes both comfortable and fun. Kitzinger (1978) describes several other variations of Pelvic Floor Exercises for pregnancy and childbirth, Robinson et al (2000) provide three visualization ideas to facilitate the process. Older literature may suggest practising whilst passing urine, but this is no longer recommended as a regular strengthening activity, since it may cause urinary reflux.It can, however, be used occasionally in order to identify the pelvic floor. Performing Pelvic Floor Exercises The exercises above are sometimes referred to as Kegel exercises, after the Californian doctor who described them. They are not useful if only performed occasionally. They need to become part of life to ensure maintenance of tone, preferably several times daily, as frequently as •Obesity, (leading to an increase in pressure on the abdomen and it’s contents) •Actions that cause persistent pressure such as coughing (i.e., uncontrolled asthma or chronic bronchitis) or constipation. •Occupations or leisure activities that cause persistent pressure (e.g. athletics, parachuting, standing work, heavy lifting)