
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Right ventricular MI
Similar to Right ventricular MI (20)
Recently uploaded
Recently uploaded (20)
Right ventricular MI
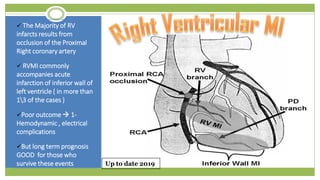
- 1. The Majority of RV infarcts results from occlusion of the Proximal Right coronary artery RVMI commonly accompanies acute infarction of inferior wall of left ventricle ( in more than 13 of the cases ) Poor outcome 1- Hemodynamic , electrical complications But long term prognosis GOOD for those who survive these events Up to date 2019
- 2. m Right Coronary Artery (RCA ( 1- Right atrium 2- Right ventricle Area involved in Inferior and RV infarcts 1- SA node 2-AV node Branch posterior Descending (PD) posterior left-infero 31posterior,ventricle of the septum Left coronary artery (LCA) anterior surface of the left ventricle Area involved in Anterior infarcts anterior 23 of the septum Circumflex : 1- left atrium 2-lateral wall of the left ventricle Area involved in lateral infarcts Up to date 2019
- 3. Electrical ConsequencesHemodynamic consequencesCulprit lesion site Ischaemia ± activation of cardioinhibitory reflexes SA ,AV nodal dysfunction Bradycardia depends on 1 or both : Extent of RV dysfunction , Extent of LV dysfunction ** Monitor hemodynamic patho physiology ttt Right ventricle is supplied by RCA through marginal branches Patients with acute RVMI high grade AV block OR Bradycardia hypotension without AV block proximal occlusion dec. RV Free wall perfusion Dyskinesis fall in blood delivery to LV ( even with intact LV systolic function ) Majority of RVMI occlusion of the RCA proximal to the Right marginal branches Notes: * Hypotension bradycardia due to vagal afferent on LV , RV or infero-posterior * Tachycardia may be present due to sympathetic discharge to raise CO ) Other factors : 1-Right Atrial ischaemia ( occlusion to proximal right atrial branches ) 2- depression of LV function ( prior MI) 3- Ticuspid valve regargitation 4- mechanical complications of MI In 15 % of population , or pts with left predominant system 50 % of RV supplied with left circulation ( chronic occlusion , significant collateral flow from the left anterior descending or circumflex arteryUp to date 2019
- 4. ECHOcardiogramECGClinical presentation ECHO Shows RV cavity dilatation , impaired RV free wall motion ** Urgent Echo should be in pts with an inferior MI + Evidence of Hemodynamic compromise RVMI Signs 1- Hypotension 2- JVP increased 3-Clear lung Fields 4- ECG : ST elevation of an acute inferior MI Major limitation : suboptimal visualization of the cardiac structures in some pts Inferior wall infarction by ST Elevation in leads II ,III ,aVF Right Sided pericordial leads V4R ,V5 , V6 particularly V4R Small RVMI : may not lead to hypotension ,No JV distension Most ECHO signs : 1-RV cavity dilatation ( RA dilataion incase of iscahemia ) 2-impaired RV free wall motion 3-Diastolic reversed septal curvature 3- Dec. TAPSE & or reduced EF 4-plethora of inferior Vena Cava ** Note : PE & Pulmonary HTN ECHO abnormalities ≥ 1 mm doming ST elevation of Right sided pericordial leads V4R, v5R Note : * pericarditis with pericardial temponade may present with similar pic - Echo shows RV dilatation in RVMI Note : LVMI : contrast of RVMI * pulmonary congestion , S3, S4 heart sounds , mitral valve murmur
- 5. Differential DiagnosisHemodynamic monitoring Percarditis TemponadesPERVMIIn minority of pts, placement of Pulmonary artery catheter ( ** ischaemic RV is prone to catheter induced Ventricular arrithmyia ) ST elevation in inferior leads : lead III ,II , aVR ECG : ST Elevation in Right percordial leads V1 , V2 No Inferior ECG : ST elevation in right Percordial leads V4R ,V5R ,V3R inferior leads : lead III ,II , aVRHemodynamically significant RV infarcts inc . in RA pressure to pulmonary wedge pressure > 0.8 ( normal<0.6) Diastolic filling pressures of RA ,RV , PCW ,LV may be elevated or equalized Kussamaul’s sign in JVP if LV dysfunction may prevent manifestation Plerutic chest pain , clear lung fields , hypotension ( shock Troponin +ve Ischemic Chest pain , clear lung fields , hypotension ( shock ) troponin +ve ECHO No DilatationECHO , right ventricular systolic dysfunction McConenell’s sign n large PE - Additional testing : VQ perfusion helical CT scanning ECHO , right ventricular systolic dysfunction RV Cavity dilatation , RV free wall motion Other Studies : Cardiac MRI is more sensitive in inferior MI but not recommended to be used
- 6. Outline of Treatment of RVMI General treatment : Dual Antiplatet therapy ( Aspirin + P2Y12 inhibitor ) Anticoagulant Statin Therapy Use with Caution ø Drugs that Decrease Preload ( nitrates , diuretics ) ø decrease contactility ( CCB ) ø slow HR (ββ) Incase of Low cardiac output , clear lung field , low or normal JVP optimization of preload Small boluses of normal Saline to increase preload Presistant Hypotension even after salin Dopamine ( grade 2C)usual starting dose 5 mcg kg min RVMI don’t benefit from afterload reducing therapy “Some “ pts may benefit from afterload reducing therapy ( either : Vasodilating agents ,intraaortic ballon ) Bradycardia , AV abnormalities Atropine (parasympatholytic) & Transvenous pacing AVOID drugs that decrease preload : Nitrates, opioids , Diuretics
- 7. Optimization of HR &AV synchronny Optimization of RV after loadOptimization of RV preloadGeneral Management In pts with RVMI Atropine ( parasympatholytic) Temporary Pacemaker ** Ischemic right ventricle has fixed StrokeVolume then RV Output depends on the HR & AV transport RV output may be comprimised Incases of LV dysfunction with elevation of pulmonary venous pressure , Hypoxemia with pulmonary artery VC ,α agonists pulmonary VC, mechanical Ventillation Incase of evidence of low CO : ( Hypotension , hypoperfusion , normal low JVP ) who don’t have Rv failure or pulmonary congestion intravenous fluids :Saline Coronary Reperfusion fibrinolytics PCI Show better prognosis RV Recovery Like the management of STEMI Dual Antiplatelet therapy ( Aspirin + P2Y12 inhibitor ) Anticoagulant Statin Therapy Use with Caution ø Drugs that Decrease Preload ( nitrates , diuretics ø Antiischaemic used with caution insatble pts ( decrease contactility ( CCB ) ø slow HR (ββ Some give atropine before PCI in the case of vagotonia HR < 55 beatsmin even if BP normal RV Afterload reducing agent is not indicated But RV MI with LV dysfunction use intraaortic balloon pump Occasionally afterload reducing agents • 200 -300 ml of saline + assessing JVP & BP •Once increases in JVP > 15 mmHg without increases in aortic pressure further expansion won’t improve hemodynamics - Severe Hypotension stabilized by inotropic agents , vasopressors Inotropic agents hypotension not responding to fluid resusitation Dopamine 5 mcgkgmin up to 15 mcg kgmin depending on response ( monitor for ventricular ectopy &tachycardia Dubtamine 5 mcgkgmin-> upto 20 mcgkgmin ( same as Dopamine) - Dec. PR higher doses dec BP Mechanical Assist devices intraaortic balloon pump in cardiogenic shock due to LV dysfunction Impella PR improves hemodynamics in RV failure øAvoid use of Nitrates ,diuretics as they reduced RV Preload Øinsertion of a bladder catheter can cause inc. vagal tone dec preload , cardiogenic shock Reperfusion with primary PCI or fibrinolytics ( check pharmacotherapy practice guide)
- 8. Pharmacotherapy principles & practice :ACS