1. BACKGROUND
Disclosures and Contributions
Authors of this project have the following to disclose concerning
possible financial or personal relationships with commercial entities
that may have a direct or indirect interest in the subject matter of this
project.
• The preliminary results of this sub-analysis have not been yet
reviewed by the sponsor and the authors are solely responsible for the
contents of this report.
• Dr. Lapointe was funded by research grant from
• Dr. Lapointed has previously received speaking honoraria from
• Redcap project was funded by SCTR-Office of Biomedical Informatics
Services grant support.
Ann Winston Thornhill, PharmD Candidate; Austin Avrett, PharmD Candidate; Danielle Ball, PharmD Candidate;
Mike Corvino, PharmD Candidate; Marc Lapointe, PharmD, BCPS; Pierre Giglio, MD
THE CLINICAL IMPACT OF HYPONATREMIA IN NEURO-ONCOLOGY:
A GLOBAL 7-YEAR RETROSPECTIVE EVALUATION
METHODS
RESULTS
OBJECTIVES
CONCLUSION
• Poor documentation of fluid status in patient
charts
• Lack of documentation of signs and symptoms of
hyponatremia when treatment was initiated
• Laboratory values only available through MUSC
health system electronic medical records
• Approximately 300 patients in the database were
excluded due to lack of laboratory data
• No cases of hyponatremia <115 were observed
RESULTS LIMITATIONS
Demographics
Normonatremic
Patients
N=441
Hyponatremic
Patients
N=178
Mean age, n, yr 49 55
Male, n (%) 214 (49) 100 (56)
Female, n (%) 227 (51) 78 (44)
Ethnicity, n (%)
African American 97 (22) 46 (26)
Caucasian 329 (75) 122 (69)
Hispanic 10 (2) 4 (2)
Other 5 (1) 6 (3)
Tumor treatment
duration
Tumor Type
Normonatremic
Patients
N=441
Hyponatremic
Patients
N=178
N % N %
Adenoma 10 2 1 <1
Astrocytoma 44 10 13 7
Ependymoma 26 6 8 4
Ganglioma 10 2 1 <1
Glioblastoma 106 24 62 35
Glioma 18 4 10 6
Lymphoma 6 1 11 6
Meningioma 102 23 26 15
Oligoastrocytoma 12 3 5 3
Oligodendroglioma 24 5 9 5
Other 53 12 28 16
Unknown 30 7 4 2
Diagnostic and Treatment Modalities
• Observed hyponatremia treatment modalities
and sequence of therapies utilized were not
standardized.
• Treatments included fluid restriction, salt
tablets, hypertonic saline, normal saline, and
loop diuretic
• 11% of patients treated were overcorrected,
74% of these were patients with moderate –
severe hyponatremia
• Although we observed a relatively high
incidence of hyponatremia that required
medical management, we only observed
isolated cases of ER and outpatient visits due
to hyponatremia.
• We did see however prolonged hospital stay
due to hyponatremia.
• Diagnostic testing of urine osmolality was not
routinely conducted in the majority of cases
and treatment was administered without
definitive knowledge of volume status.
• Future studies to standardize diagnostics and
treatment modalities in this patient population
are needed
• Hyponatremia is a common electrolyte disorder,
defined as a serum sodium concentration < 135
mEq/L.
• It is categorized as hypovolemic, euvolemic, and
hypervolemic hyponatremia based on the patient’s
extracellular fluid volume.
• Clinically significant neurologic symptoms of
hyponatremia generally occur at serum sodium
concentrations < 130 mEq/L. Common complaints
include encephalopathy, lethargy, confusion,
ataxia, difficulty concentrating, and psychosis.
• Approach to treatment of non-acute cases is
generally based on clinical severity and underlying
cause of the disorder.
• Patients with brain tumors are particularly
sensitive to the CNS side effects of hyponatremia.
This can have a significant impact on morbidity
and mortality, as the associated symptoms often
overlap with those of their primary disease and
the adverse effects of medications used during
treatment.
• Electronic medical records of patients diagnosed
with a brain tumor between 2006 to 2014 were
retrospectively examined.
• Records were used to evaluate:
• Demographic characteristics
• Incidence and recurrence of hyponatremia
• Treatment modalities and rate of correction
• Determine the incidence of hyponatremia during
the entire course of brain tumor management.
• Determine the incidence of clinically significant
hyponatremia requiring medical management.
• Characterize the diagnostic and treatment
modalities used to manage hyponatremia.
• Evaluate the treatment modalities used and their
associated outcomes.
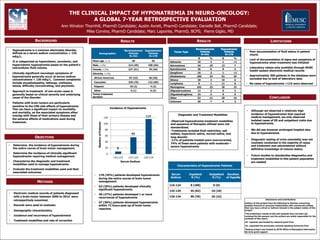
Incidence of Hyponatremia
• 178 (29%) patients developed hyponatremia
during the entire course of brain tumor
management.
• 63 (35%) patients developed clinically
significant hyponatremia.
• 48 (27%) patients developed 1 or more
recurrences of hyponatremia
• 67 (38%) patients developed hyponatremia
within 72 hours post-op of brain tumor
resection
Characteristics of Hyponatremic Patients
Serum
Sodium
Inpatient
N (%)
Outpatient
N (%)
Duration
of HypoNa
116-124 8 (100) 0 (0)
125-129 45 (82) 10 (18)
130-134 90 (78) 25 (22)