1. Background
• Heart failure (HF) occurs in more than 5.8 million people in the
United States and is among the most frequent causes of
hospitalizations1
• It is a progressive disorder characterized by the inability of the
heart to fill (diastolic HF) or eject (systolic HF) with sufficient blood
to the rest of the body. Clinically diagnosed systolic HF patients
have a reduced EF (HFrEF) of ≤ 40%1
• Aldosterone levels are elevated in HF patients due to decreased
renal perfusion. Binding of aldosterone to its receptor leads to
sodium and fluid retention, endothelial dysfunction, left ventricular
hypertrophy and myocardial fibrosis2
• Standard therapy currently includes an angiotensin converting
enzyme (ACE) inhibitor or angiotensin II receptor blocker (ARB)
and an evidence-based beta blocker1
• ACC/AHA guidelines suggest the use of an aldosterone receptor
antagonist (ARA’s) in addition to standard therapy in NYHA class II
to IV HF patients and post myocardial infarction patients with a
HFrEF of ≤ 40%1
• There is overwhelming evidence of benefit of ARAs in reducing
mortality and hospitalizations as shown in multiple trials: RALES,
EPHESUS & EMPHASIS-HF3-5
• However in practice, aldosterone antagonists are prescribed only
to 35% of eligible patients6
• In 2011, HF was responsible for costs of more than $39 billion
annually in the USA alone6
Purpose
• To analyze the benefits of using ARAs in eligible HF
patients and reveal the underutilization in practice
Methods
• Literature Search performed using Pubmed, Ovid &
Clinicaltrials.gov to find randomized clinical trials and other
primary literature
• Various key terms were used such as “systolic heart failure,”
“eplerenone,” “spironolactone,” and “aldosterone antagonists”
• The search included the following filters: English language,
humans and full text accessible
• Supplemental information was obtained from AHA/ACC
guidelines, Pharmacotherapy: A Pathophysiologic Approach and
UpToDate
Discussion
• There is currently no evidence of using an ARA in patients with
diastolic HF or in patients who are already stable on just an
ACEI/ARB and beta blocker
• ARAs should only be used in patients with a creatinine clearance
>30mL/min and potassium levels <5.0 mEq/dL
• Underuse of ARAs may be attributed to the need for regular follow-up
visits due to the increased risk of hyperkalemia and increased
incidence of gynecomastia
• Although spironolactone and eplerenone are equally effective,
eplerenone is more selective to the mineralocorticoid receptor and is
shown to have less side effects
• Eplerenone has lower incidences of hyperkalemia and
gynecomastia
• However, spironolactone is more often used in practice because it is
relatively inexpensive
• In RALES, only 11% of patients were on a beta blocker because
benefit for them had not yet been established
• Relative risk reduction for spironolactone may have been
overestimated due to suboptimal therapy
Conclusion
• From current studies, ARAs should be initiated alongside
standard therapy to reduce morbidity, mortality, and
hospitalization in patients who are experiencing NYHA class II-
IV symptoms and have experienced CV complications in the
past 6 months
• Despite the concerns, cases of severe hyperkalemia were
shown to be low throughout clinical trials with no cases of death
from hyperkalemia. This should ease the apprehension that a
physician may have when prescribing these medications
Future Treatment Options
• Look toward the development of novel selective aldosterone
antagonists
• Currently BAY94-8862 (finerenone) is a non-steroidal aldosterone
antagonist in phase III clinical trials for the treatment of HF
• Current trials show decrease in non-selective adverse effects such as
gynecomastia, impotence, and low libido
• Trials also show a low incidence of hyperkalemia in all dose groups
averaging 2.4% allowing for reduced treatment cost due to reduction
in monitoring of hyperkalemia
References
1. Yancy, CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, et al. 2013 Guideline for the management of heart
failure a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice
guidelines. Circulation 2013;128:e240-e327
2. Nagarajan V, Chamsi-Pasha M, Tang WH. The role of aldosterone receptor antagonist in the management of heart
failure: An update. Cleve Clin J Med. Sept 2012; 79 (9)
3. Pitt B, Zannad F, Remme W, Cody R, Castaigne A, Perez A, et al. The effect of spironolactone on morbidity and mortality
in patients with severe heart failure. N Engl J Med 1999;341(10):709-717
4. Pitt B, Remme W, Zannad F, Neaton J, Martinez F, Roniker B, et al. Eplerenone, a Selective Aldosterone Blocker, in
Patients with Left Ventricular Dysfunction after Myocardial Infarction. N Engl J Med 2003;348(14):1309-21
5. Zannad F, McMurray JJ, Krum H, Veldhuisen DJ, Swedberg K, Shi H, et al. Eplerenone in Patients with Systolic Heart
Failure and Mild Symptoms. N Engl J Med. 2011;364:11-21
6. Fonarow GC, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, et al. Heart failure in the outpatient
cardiology practice setting: findings from IMPROVE-HF. Circ Heart Fail 2008;1(1):98-106
7. Pitt B, Zannad F. Eplerenone: Is it time to add this drug to current heart failure therapy? Ther Adv Chronic Dis
2012;3(1):5-9.
8. Bakris GL, Agarwal R, Chan JC, Cooper Me, Gansevoort RT, Haller H, et al. Effect of eplerenone on albuminuria in
patients with diabetic nephropathy: A randomized clinical trial. JAMA 2015 1;214(9):884-894
9. Eschalier R, McMurray J, Swedberg K, Veldhuisen D, Krum H, Pocock SJ, et al. Safety and efficacy of eplerenone in
patients at high risk for hyperkalemia and/or worsening renal function: analyses of the EMPHASIS-HF study subgroups
(Eplerenone in Mild Patients Hospitalization And SurvIval Study in Heart Failure). J Am Coll Cardiol 2013;62(17):1585-93
10. Bui AL, Horwich TB, Fonarow GC. Epidemiology and risk profile of heart failure. Nat Rev Cariol 2011;8(1):30-41
11. Maron BA, Leopold JA. Aldosterone Receptor Antagonists; effective but often forgotten. Circulation. 2010; 121(934-939)
12. Albert NM, Yancy CW, Liang L, et al. Use of Aldosterone Antagonists in Heart Failure. JAMA. Oct 2009:32(15)
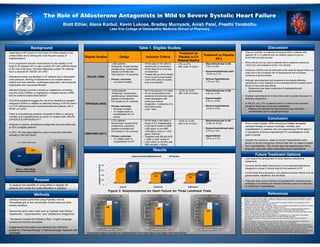
Table 1. Eligible Studies
Eligible Studies Design Inclusion Criteria
Treatment vs
Placebo in CV
Related Deaths
Treatment vs Placebo
AE’s
RALES (1999)
• 1,663 patients
• Multicenter, double-blinded,
parallel-group, randomized,
placebo-controlled trial
• 195 centers in 15 countries
• Primary outcomes:
• All cause mortality
• NYHA class IV HF within 6
months prior to enrollment
• NYHA class III or IV at time
of enrollment
• Treated with an ACE inhibitor
(if no CI) and a loop diuretic
• LVEF<35% within 6 months
prior to enrollment
• 27% vs 37%
• (RR, 0.69; P<0.001)
• Discontinued due to AE:
7.5% vs 4.8%
• Gynecomastia/breast pain:
10.2% vs 3.1%
• Serious Hyperkalemia:
1.7% vs 1.2%
EPHESUS (2003)
• 6,642 patients
• Multicenter, double-blind,
parallel-group, randomized,
placebo-controlled trial
• 674 centers in 37 countries
• Primary outcomes:
• All-cause mortality
• CV related death or
hospitalization for CV
events
• MI in the previous 3-14 days
• HF as documented by the
presence of pulmonary rales,
chest radiography with
pulmonary venous
congestion, or presence of a
third heart sound
• LVEF <40%
• 12.3% vs 14.6%
• (RR, 0.83; P=0.005)
• Discontinued due to AE:
4.4% vs. 4.5%
• Gynecomastia:
0.5% vs. 0.6%
• Serious hyperkalemia:
5.5% vs 3.9%
EMPHASIS (2011)
• 2,737 patients
• Randomized, double-blind,
prospective, superiority,
placebo-controlled trial
• 278 centers in 29 countries
• Primary outcomes:
• CV related death or
hospitalization for HF
• NYHA class II with either a
history of CV hospitalization
in the last 6 months or BNP
>250 pg/mL or pro-BNP
>500 pg/mL (men) or >750
pg/mL (women)
• Treatment with BB and ACE-
I, ARB, or both unless CI
• LVEF ≤30% (or 30-35% with
QRS duration >130ms)
• 10.8% vs 13.5%
• (HR, 0.76; P=0.01)
• Discontinued due to AE:
13.8% vs 16.2%
• Gynecomastia/breast pain:
0.7% vs 1.0%
• Hyperkalemia:
8.0% vs 3.7%
Results
* Composite Endpoint consists of hospitalizations from heart failure and death from heart failure
The Role of Aldosterone Antagonists in Mild to Severe Systolic Heart Failure
Brett Ethier, Alena Korbut, Kevin Lukose, Bradley Murnyack, Anish Patel, Preethi Yarabothu
Lake Erie College of Osteopathic Medicine School of Pharmacy
0
200
400
600
800
RALES EPHESUS EMPHASIS
515
345
304
753
391 399
NUMBEROFPATIENTS
Figure 3. Hospitalizations for Heart Failure for Three Landmark Trials
Spironolactone/Eplerenone Placebo
536
650
0
100
200
300
400
500
600
700
NUMBEROFPATIENTS
Figure 4. Composite Endpoint*
for RALES Trial
Relative Risk Reduction Sprionolactone Placebo
32% RRR
885
993
400
500
600
700
800
900
1000
1100
NUMBEROFPATIENTS
Figure 5. Composite Endpoint*
for EHPESUS Trial
Relative Risk Reduction Eplerenone Placebo
13% RRR
249
356
0
50
100
150
200
250
300
350
400
NUMBEROFPATIENTS
Figure 6. Composite Endpoint*
for EMPHASIS Trial
Reduction in Risk Eplerenone Placebo
37% RR
25%
75%
Figure 1. Heart Failure
Prevalence Worldwide
US Rest of the world
0
10
20
30
40
50
60
70
80
90
80
86
36
Figure 2. Underuse of
Aldosterone Antagonists
ACE/ARB B-Blocker Aldosterone Antagonists
Lightspring. Human Heart Anatomy from a Healthy Body on a Blue and
Black Graph Background as a Medical Health Care Symbol of an Inner
Cardiovascular Organ. Digital image. Lightspring's Portfolio. Shutterstock,
n.d. Web. 1 Apr. 2016.