BURDEN OF ORAL DISEASES
•Download as PPTX, PDF•
0 likes•58 views

AMRITA SCHOOL OF DENTISTRY

Recommended
Recommended
More Related Content
Similar to BURDEN OF ORAL DISEASES
Similar to BURDEN OF ORAL DISEASES (20)
More from Aneesa K Ayoob
More from Aneesa K Ayoob (20)
Recently uploaded
Recently uploaded (20)
BURDEN OF ORAL DISEASES
- 1. BURDEN OF ORAL DISEASES Seminar no:14
- 2. 2 CONTENTS Introduction Measurements of Burden of Disease Major Oral Diseases and Health Conditions Economic Burden of Oral Diseases Burden of Oral Diseases – India Conclusion References
- 3. INTRODUCTION • The Global Burden of Disease (GBD) provides a tool to quantify health loss from hundreds of diseases, injuries, and risk factors, so that health systems can be improved, and disparities can be eliminated. • The GBD 2019 is the most comprehensive global health study, analyzing 286 causes of death, 369 diseases & injuries, and 87 risk factors. 3
- 4. • The Global Burden of Disease Study 2019 estimated that oral diseases affect close to 3.5 billion people worldwide, with 2 billion people suffering from caries of permanent (most common condition) and 520 million children suffer from caries of primary teeth. • In most low- and middle-income countries, the prevalence of oral diseases continues to increase with growing urbanization and changes in living conditions. 4 Overview of global burden of oral diseases:
- 5. 5 1. Incidence rate: Defined as the number of NEW cases occurring in a defined population during a specified period of time. 2. Prevalence: Defined as the total number of all individuals who have an attribute or disease at a particular time (or during a particular period) divided by the population at risk of having the attribute or disease at this point in time or midway through the period. 3. Life expectancy: Life expectancy is the number of years that the average member of a group can expect to live. MEASUREMENTS OF BURDEN OF DISEASE
- 6. 6 3. Disability-Adjusted Life Years (DALYs): DALY = years of life lost + years lost to disability • It is defined as the number of years of healthy life lost due to all causes whether from premature mortality or disability. • Year of Life Lost: no of death at each age multiplied by the expected remaining years of life according to a global standard life expectancy. • Years Lost to Disability: no of incident cases due to injury and illness is multiplied by the average duration of disease and a weighing factor reflecting the severity of disease on a scale from 0 (perfect health) and 1(dead). One DALY = One year of healthy life lost
- 7. 7 4. Health Adjusted Life Expectancy (HALE): • Based on the framework of WHO’s ICIDH (International Classification of Impairments, Disabilities, and Handicaps ) • It is the equivalent number of years in full health that a newborn can expect to live based on current rates of ill-health and mortality. 5. Assessment of risk factors in the GBD: • A three-level hierarchical organization system was established. • Level 1 risks were clusters of risk factors linked by mechanism, biology or potential policy intervention. • Level 2 risks represented the major proportion of the risk factors themselves. • For some risk factors, such as occupational carcinogens, a third level was added to provide additional detail.
- 8. 8 Level 1 causes are aggregates of non-communicable diseases; injuries; and a category combining infectious diseases, maternal and neonatal disorders, and nutritional deficiencies. Level 2, there are 22 disease and injury aggregate groupings such as respiratory infections and tuberculosis, cardiovascular diseases, and transport injuries. Level 3 includes specific causes such as tuberculosis, stroke, and road injuries. In some cases, these Level 3 causes are the most detailed classification, while for others a more detailed category is specified at Level 4. Examples of Level 4 causes include latent tuberculosis infection, ischemic stroke, and pedestrian road injuries. GBD classifies causes in a hierarchy of four levels.
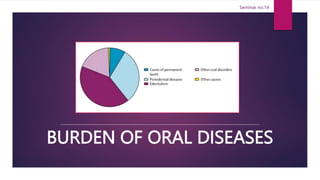
- 9. 9 • Oral disorders was the tenth-ranked Level 3 cause of disability globally in 2019, causing 23·1 million (95% UI 13·6–37·4) YLDs. It was also ranked first and third globally for prevalence (3·48 billion [3·20–3·78] cases) and incidence (4·35 billion [3·89–4·84] cases) in 2019. • Oral disorders comprises caries of deciduous and permanent teeth, chronic periodontal diseases, edentulism (total tooth loss), and other oral disorders (a heterogeneous group including a variety of tooth, tongue, and jaw disorders and malformations not included in the other causes). Source: https://www.healthdata.org/results/gbd_summaries/2019/oral-disorders-level-3-cause
- 10. 10
- 11. Dental caries : Caries of permanent teeth — Level 4 cause • Caries of permanent teeth is defined as permanent dentition showing unmistakable cavity, undermined enamel, a detectably softened floor or wall, a tooth with a temporary filling or a tooth that is filled but also decayed is present. • Caries of permanent teeth caused 2·00 million (95% UI 0·915–3·88) YLDs globally in 2019. It was also ranked first and third globally for prevalence and incidence among all Level 4 causes, with 2·03 billion (1·77–2·33) prevalent and 3·09 billion (2·76–3·39) incident cases in 2019. 11 MAJOR ORAL DISEASES AND HEALTH CONDITIONS
- 12. 12 Periodontal diseases — Level 4 cause • Chronic periodontal disease is defined as Community Index of Periodontal Treatment Needs (CPITN) Class IV, attachment loss (AL) >6 mm, or gingival pocket depth (PD) >5 mm. It is caused by chronic bacterial infection around the teeth. • Chronic periodontal disease causes 7·09 million (95% UI 2·78–15·5) YLDs globally in 2019. It was also ranked seventh and 32nd globally for prevalence and incidence, with 1·09 billion (0·828–1·36) prevalent and 91·5 million (74·2–110) incident cases in 2019.
- 13. 13 Lip and oral cavity cancer — Level 3 cause • This cause includes death and disability resulting from malignant neoplasms of the lips and oral cavity, including ICD-10 codes such as C00–C08 (malignant neoplasm of lip, base of tongue, other and unspecified parts of tongue, gum, floor of mouth, palate, other and unspecified parts of mouth, parotid gland, other and unspecified major salivary glands). • There were 373 000 incident cases (95% UI 341 000–404 000), 199 000 deaths (182 000–218 000), and 5·51 million (5·00–6·03) DALYs due to lip and oral cavity cancer globally in 2019.
- 14. 14 Orofacial clefts — Level 4 cause • Any livebirth with isolated cleft lip, isolated cleft palate, and combined cleft lip and cleft palate resulting from the tissues of the face not joining properly during foetal development. • Orofacial clefts caused 2770 all-ages deaths (1660–5440). The combined global incidence rate was 1·42 per 1000 (0·925–2·18) livebirths, and there were 4·62 million (3·76–5·67) people living with orofacial clefts in 2019.
- 15. 15 Edentulism and severe tooth loss — Level 4 cause • Edentulism is defined as total tooth loss. • Edentulism and severe tooth loss was the 22nd ranked Level 4 cause of disability globally in 2019, causing 9·62 million (95% UI 6·15–14·2) YLDs. It was also ranked 31st and 56th globally for prevalence and incidence, with 352 million (280– 449) prevalent cases and 25·0 million (19·8–30·7) incident cases in 2019.
- 16. Oro-dental trauma • Oro-dental trauma results from injury to the teeth, mouth and oral cavity. • Around 20% of people suffer from trauma to teeth at some point in their life. • Oro-dental trauma can be caused by oral factors such as lack of alignment of teeth and environmental factors . 16 • Treatment is costly and lengthy and sometimes can even lead to tooth loss, resulting in complications for facial and psychological development and quality of life.
- 17. Noma • Noma is a severe gangrenous disease of the mouth and the face. • It mostly affects children aged 2–6 years suffering from malnutrition, affected by infectious disease, living in extreme poverty with poor oral hygiene or with weakened immune systems. • Noma is mostly found in sub-Saharan Africa, although cases have also been reported in Latin America and Asia. 17 • According to estimates (from 1998) there are 140 000 new cases of noma annually. • Without treatment, noma is fatal in 90% of cases. • Where noma is detected at an early stage, its progression can be rapidly halted through basic hygiene, antibiotics and improved nutrition.
- 18. 18
- 19. 19
- 20. • Oral diseases disproportionally affect the poor and socially disadvantaged members of society. • There is a very strong and consistent association between socioeconomic status (income, occupation and educational level) and the prevalence and severity of oral diseases. 20 • This association exists from early childhood to older age and across populations in high-, middle- and low-income countries. ORAL HEALTH INEQUALITIES
- 21. • Unequal distribution of oral health professionals and a lack of appropriate health facilities to meet population needs in most countries means that access to primary oral health services is often low. 21 • Out-of-pocket costs for oral health care can be major barriers to accessing care. • Paying for necessary oral health care is among the leading reasons for catastrophic health expenditures, resulting in an increased risk of impoverishment and economic hardship. ACCESS TO ORAL HEALTH SERVICES
- 22. WHO response • The World Health Assembly approved a Resolution on oral health in 2021 at the 74th World Health Assembly. • The Resolution recommends a shift from the traditional curative approach towards a preventive approach that includes promotion of oral health within the family, schools and workplaces, and includes timely, comprehensive and inclusive care within the primary health-care system. 22 • The Resolution affirms that oral health should be firmly embedded within the noncommunicable disease agenda and that oral health-care interventions should be included in universal health coverage programs.
- 23. 23 • The World Health Assembly delegates asked WHO: to develop a draft global strategy on tackling oral diseases for consideration by WHO governing bodies in 2022; and by 2023: to translate the global strategy into an action plan for oral health; to develop “best buy” interventions on oral health; and to explore the inclusion of noma within the roadmap for neglected tropical diseases 2021-2030. • WHO was asked to report back on progress and results until 2031 as part of the consolidated report on noncommunicable diseases.
- 24. 24 • The sizable burden of oral disorders (measured as DALYs) and their socioeconomic impact make them an important global public health issue. • The Lancet made a commitment starting with GBD 2015 to publish 4 signature papers annually covering mortality, YLDs, DALYs, and risk factors (GBD 2015: from . . . 2016).
- 25. 25 • The age-standardized rate (ASR) of the prevalence, incidence, and DALYs increased worldwide from 1990 to 2019. • In 2019, Western Sub-Saharan Africa carried the heaviest burden of periodontitis, whereas the nation with the highest periodontitis burden was Gambia. • The burden of periodontitis was negatively associated with the level of socioeconomic development. • Although, the majority of periodontitis burden was observed among those aged 55–59 years, the incidence of periodontitis has shown an increasing trend among younger individuals.
- 26. 26 • Age-standardized prevalence of caries in permanent and deciduous teeth decreased 3.6% (95% uncertainty interval, 2.6% to 4.5%) and 3.0% (1.3% to 4.9%), respectively. • Population growth was the key driver of the changes in the number of caries cases, especially in sub-Saharan Africa (percentage contribution: 126.6%, permanent teeth; 103.0%, deciduous teeth). • Globally, 64.6 million (95% CI, 64.4 to 64.9 million) and 62.9 million (62.8 to 63.1 million) prevalent cases of caries in permanent and deciduous teeth were attributable to sociodemographic inequality in 2019. • This amounted to 3.2% (3.2% to 3.2%) and 12.1% (12.1% to 12.1%) of the global number of prevalent cases of caries in permanent and deciduous teeth.
- 27. 27 ECONOMIC BURDEN OF DENTAL DISEASES • Dental diseases impose a significant financial burden on society. • The financial burden is caused by three types of expenses: direct costs (treatment costs), indirect costs (productivity losses from absences from work and school), and intangible costs (pain, difficulties with speaking, tasting, biting, chewing, or eating, difficulties expressing emotions like smiling, and involvement in social activities) (S. Listl et al., 2015). • Prediction results show an increase in per capita oral health spending across the majority of nations, assuming no significant policy changes. • Germany is predicted to spend the most expenditure in 2040 ($889 USD), while Mexico would spend the least ($52 USD). (Milica Jevdjevic et al., 2021). Source: Talal M. Alzahrani, Ahmad A. Jumah, Fayez A. Alshehri, Sattam A. Alshiha (2022). Assessment of the Economic Burden of Dental Diseases. Saudi J Oral Dent Res, 7(9): 220-224.
- 28. 28 Challenges for Oral Health Related Economic Evaluations Source: Talal M. Alzahrani, Ahmad A. Jumah, Fayez A. Alshehri, Sattam A. Alshiha (2022). Assessment of the Economic Burden of Dental Diseases. Saudi J Oral Dent Res, 7(9): 220-224. • The GBD's use of disability weights for oral diseases has not been properly reported. The most commonly cited data on the burden of caries worldwide (The Global Burden of Disease Study), based their statistics on a contentious assumption where all DMFT reported in epidemiological studies were counted as the DT component, representing solely untreated caries lesions (Bernabe et al., 2020). • Despite several attempts to construct a meaningful alternative measure to translate oral health benefits (Birch & Ismail, 2002), the lack of utilities employed in economic evaluations has been listed as one of the main shortcomings of dental research (Qu et al., 2019; Rogers et al., 2019).
- 29. 29 BURDEN OF ORAL DISEASES - INDIA • The prevalence of dental caries among the 12-year- old’s ranged between 23.0 % to 71.5 % and adults aged 35-45 years was between 48.1% to 86.4%. • The elderly in 65-74 years had dental caries in the range of 51.6 % to 95.1 %. • Periodontal diseases among adults & elderly were in the range of 15.32 % to 77.9 % & 19.9% to 96.1%. • The prevalence of untreated dental caries in children below six years was found to be 49.6 % in India as per the systematic review published in year 2018.
- 30. 30
- 31. 31
- 32. 32 Economic Impact of Oral Health Services in India: • From the Current Health Expenditures, Union Government share is Rs. 46896 crores (8.7%) and the State Government’s share Rs. 84953 crores (15.8%). • Local bodies’ share is Rs. 4339 crores (0.8%), Households share (including insurance contributions) about Rs. 367373 crores (68.1%, OOPE being 63.2%), enterprises (including insurance contributions) is Rs. 24512 crores (4.5%) and NGOs is Rs. 7837 crores (1.5%). • External/donor funding contributes to about Rs. 3462 crores (0.6%). • Contribution by Current Dental outpatient curative care Expenditures is Rs. 392.44 crores (0.07% of total health expenditures) according to National Health Accounts Estimates for India 2016-17.
- 33. 33 Targets: 1. Oral Health Status • Establish baseline data for oral disease burden of the country by 2025. • Reduce the morbidity and mortality from dental and oro-facial diseases by 15% by 2030 2. Health System Performance • Increase utilization of public oral health facilities by at least 50% per district by 2030. • Increase the coverage of community-based awareness programs and procedures for oral health through health care facilities by 50% by 2025; and 70% by 2030 3. Oral Health System strengthening Make available assured and appropriate preventive and promotive oral health services at each health & wellness center and primary health center by 2025 and in addition, make available assured curative oral health services at each Primary Health Center by 2030. 4. Oral Health Management Information • Ensure district-level electronic database of information on health system components by 2025. • Establish integrated oral health information architecture & exchanges between district & primary health centers by 2030.
- 34. 34 Oral health inclusion in components of National Health Mission: • Flexible Pool for Non-Communicable Diseases, Injury & Trauma which includes National Programme for Control of Blindness, National Mental Health Programme, Health Care for the Elderly, National Programme for Prevention &Control of Deafness, National Tobacco Control Programme, National Oral Health Programme, Assistance to States for Capacity Building, National Programme for Prevention and Control of Cancer, Diabetes, CVD and Stroke, Other New Initiatives under Non-Communicable Diseases. (Approved Outlay for 2019-20 – Rs 717.00 (in crores)) • Miscellaneous Programmes which includes (1) Forward Linkages to NRHM and (2) Pilot Projects which includes Sports Medicine, Deafness, Leptospirosis Control, Control of Human Rabies, Medical Rehabilitation, Oral Health, Fluorosis (Approved Outlay for 2019-20 – Rs 25.00 (in crores))
- 35. 35 National Commission on Microeconomics and Health (NCMH) Background Papers- Burden of Disease in India • Dental Caries • Dentofacial Anomalies Or Malocclusion • Periodontal Diseases • Oral Cancer • Epidemiology Of Oral And Dental Diseases
- 36. 36 • Feasible and scalable multilevel interventions, guided by multidisciplinary research collaborations. • Natural experiments on oral health care reform and policies to monitor their impacts should be reported. • The demonstration of large-scale community projects using effective evidence-based approaches should be documented. • Research on payment and delivery reform alongside related legislative and regulatory changes is limited. CHALLENGING TASKS: CLOSING THE GAPS
- 37. 37 CONCLUSION • Oral disease represents one of the most common public health issues and remains a major global health burden, yet it has frequently been neglected in public health strategy and policy. • Various oral diseases and conditions have a significant socio-economic impact. • Oral diseases and NCDs share risk factors, such as excess sugar/alcohol consumption and tobacco use. • There should be an integration of oral health into the general health agenda for optimal health and well-being. • The long-term sustainable strategy for global oral health must focus on health promotion and disease prevention, through controlling the modifiable common risk factors.
- 38. 38 REFFERNCES • Park, Park’s Textbook of Preventive &Social Medicine, 25th Edition, Jabalpur: Banarsidas Bhanot,2019. • Lajoie, Julie. "Understanding the Measurement of Global Burden of Disease." Prepared for the National Collaborating Centre for Infectious Diseases August (2013). • https://www.healthdata.org/gbd/2019 • https://www.thelancet.com/gbd • https://www.who.int/news-room/fact-sheets/detail/oral- health#:~:text=The%20Global%20Burden%20of%20Disease%20Study%202019%20estimated%20that%20o ral,the%20most%20common%20condition1.
- 39. 39 • https://pubmed.ncbi.nlm.nih.gov/33069326/ • https://www.healthdata.org/results/gbd_summaries/2019/oral-disorders-level-3-cause • https://journals.sagepub.com/doi/abs/10.1177/0022034517693567?journalCode=jdrb • https://journals.sagepub.com/doi/abs/10.1177/00220345211056247 • https://aap.onlinelibrary.wiley.com/doi/abs/10.1002/JPER.21-0469 • https://www.scielo.br/j/rsbmt/a/rvpDy9npBdFcgM89TtgLrCr/abstract/?lang=en • https://www.proquest.com/openview/0684d2394caa2c84503421d91b5fdc68/1?pq- origsite=gscholar&cbl=2045580 • https://main.mohfw.gov.in/sites/default/files/N_56820_1613385504626.pdf • https://screening.iarc.fr/doc/Commision_on_Macroeconomic_and_Health_Bg_P2_Oral_and_dental_diseases. pdf
- 40. THANK YOU 40
Editor's Notes
- Composition of DALYs by constituent Level 4 causes for both sexes combined, 2019
- Disease burden is the impact of a health problem as measured by financial cost, mortality, morbidity, or other indicators global health? Health problems, issues, and concerns that transcend national boundaries, which may be influenced by circumstances or experiences in other countries, and which are best addressed by cooperative actions and solutions (Institute Of Medicine, USA- 1997) Examples include infectious diseases (SARS, TB, avian influenza, malaria,) non infectious diseases (diabetes mellitus, tobacco related diseases) and other health risks (global warming, conflict, nuclear power) etc.
- Uses of DALYs It is the simplest and the most commonly used measure to find the burden of illness and the effectiveness of the interventions. • To assist in selecting health service priorities • To identify the disadvantaged groups • Targeting health interventions • Measuring the results of health interventions • Providing comparable measures for planning & evaluating programs • To compare the health status of different countries
- C00 This is primarily due to inadequate exposure to fluoride (in the water supply and oral hygiene products such as toothpaste), availability and affordability of food with high sugar content and poor access to oral health care services in the community. Marketing of food and beverages high in sugar, as well as tobacco and alcohol, have led to a growing consumption of products that contribute to oral health conditions and other noncommunicable diseases.
- Non fatal health outcome estimations Oral Deciduous Caries Oral Edentulism Oral Periodontal Diseases Oral Permanent Caries
- The sizable burden of oral disorders (measured as DALYs) and their socioeconomic impact make them an important global public health issue. The other notable topic relevant to oral health is the introduction of the sociodemographic index (SDI) by the GBD 2015 collaborative group (Institute for Health Metrics and Evaluation 2016b). Figure 1 shows the prevalence rate of oral disorders by SDI, and untreated dental caries accounts for a substantial amount of the overall prevalent cases regardless of SDI status. Figure 2 shows burden when DALYs are considered instead of prevalence. In this approach, edentulism is now responsible for a significant proportion of the burden, and this burden is clearly more substantial in high versus low SDI countries.
- Previous studies on the global burden of caries primarily focused on simple descriptive statistics. We aimed to characterize the burden, trends, and inequalities of untreated caries of permanent and deciduous teeth from 1990 to 2019 at the global, regional, and national levels through an array of analytic approaches. Estimates of caries burden were extracted from the Global Burden of Disease Stud Burden of dental caries remains a global public health challenge. A systemwide reform of the global oral health care system is needed to tackle the causes of the burden and inequality of dental caries. y 2019.
- Vision: All the people of India enjoy the highest possible level of dental and oro-facial health, through promotive, preventive, curative and rehabilitative services with the highest professional standards, integrity, safety, equity and ethics.