More Related Content Similar to Ebola Active Monitoring Poster, ICEID 2015 (20) 1. RESEARCH POSTER PRESENTATION DESIGN © 2012
www.PosterPresentations.com
BACKGROUND
The Centers for Disease Control and Prevention (CDC) announced in
October 2014 the start of enhanced monitoring for travelers arriving in
the USA from countries undergoing widespread transmission of Ebola
virus disease (EVD). With this enhanced effort, six District of Columbia
(DC) Department of Health (DOH) epidemiologists were tasked with
rapidly establishing contact with all domestic and international travelers
arriving in DC. The following describes our approach in implementing an
infectious disease early warning surveillance system.
OBJECTIVE
Successfully contact and actively monitor all recent travelers (or Persons
Under Monitoring (PUM)) residing in, or visiting, the District of Columbia,
within 24 hours of receiving arrival notifications from the CDC or another
US jurisdiction.
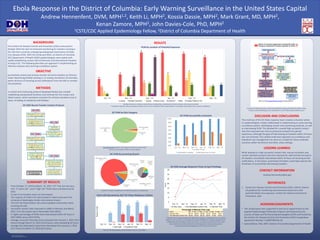
RESULTS
SUMMARY OF RESULTS
• From October 17, 2014 to March 15, 2015, 377 “low, but not zero,
risk”, 9 “some risk” and 0 “high risk” PUMs were monitored by DC
DOH.
• A total of 10 travelers were not interviewed.
• The majority of PUM in DC had traveled to Liberia and were first
screened at Washington Dulles International Airport.
• The 24/7 DC Ebola Hotline call volume peaked in December 2014,
receiving 54 calls.
• Successful contact rates improved to 100% in February and March
2015, from the lowest rate in November 2014 (85%).
• A higher percentage of PUMs were interviewed within 24 hours in
2015 (66%) versus 2014 (53%).
• Average successful interview time increased from January 1, 2015 (24.9
hours) through March 15, 2015 (32.8 hours), never exceeding 33 hours.
• Average first attempted contact time decreased from January 1, 2015
(14.7 hours) to March 15, 2015 (8.9 hours).
ACKNOWLEDGEMENTS
• This study/report was supported in part by an appointment to the
Applied Epidemiology Fellowship Program administered by the
Council of State and Territorial Epidemiologists (CSTE) and funded by
the Centers for Disease Control and Prevention (CDC) Cooperative
Agreement Number 1U38OT000143-03.
• Sasha McGee, PhD, MPH. District of Columbia Department of Health
Ebola Response in the District of Columbia: Early Warning Surveillance in the United States Capital
Andrew Hennenfent, DVM, MPH1,2, Keith Li, MPH2, Kossia Dassie, MPH2, Mark Grant, MD, MPH2,
Kenan Zamore, MPH2, John Davies-Cole, PhD, MPH2
1CSTE/CDC Applied Epidemiology Fellow, 2District of Columbia Department of Health
DISCUSION AND CONCLUSIONS
The small size of the DC Ebola response team created a situation where
six epidemiologists closely collaborated in implementing an early warning
surveillance system, developing contact and monitoring protocols, as well
as interviewing PUM. This allowed for a overall high successful contact
rate that improved over time as protocols evolved from gained
experience, although the goal of interviewing all travelers within 24 hours
was not achieved. This unified small team approach to surveillance and
individual case management can serve as a model for future outbreak
scenarios within the District and other urban settings.
REFERENCES
1. Centers for Disease Control and Prevention (CDC). (2014). Interim
US guidance for monitoring and movement of persons with
potential Ebola virus exposure. Centers for Disease Control and
Prevention, USA.
METHODS
A contact and monitoring protocol (displayed below) was created
establishing standardized timelines and methods for first contact and
failed contact, which remained consistent for all team members once in
place, including on weekends and holidays.
Total Calls Received by 24/7 DC Ebola Telephone Hotline
The 24/7 DC Ebola Hotline received the first call on 11/12/2014.
CONTACT INFORMATION
Andrew.Hennenfent@dc.gov
DC PUM Successfully Contacted
PUM by Location of Potential Exposure
*Multiple Countries includes a travel history including any combination of Liberia, Guinea, Sierra Leone and Mali
**Unknown indicates unknown exposures history due to a non-compliant PUM, contact failure or incomplete information from a airport notification.
DC PUM by Risk Category
DC DOH Average Response Times to Epi-X Postings
PUM that were contacted before the official Epi-X posting, or assisted in the care of EVD
patients in the US, were not included in the final calculations for average response times.
Additionally, first attempted contact times were not actively recorded until 2015, with
documentation of contact attempts and average times varying among persons
conducting monitoring, ranging from 10.5 hours to 26.0 hours.
Not interviewed indicates risk category could not be determined
due to a non-compliant PUM or contact failure
DC PUM by Screening Airport
*Indicates travelers transferred to DC DOH by another U.S. jurisdiction.
Example of a facility-specific protocol developed for various potential EVD patient intake
locations within Washington, DC, and posted to the DC DOH website (ebola.dc.gov)
15
19
38
38
37
34
8
2
12
4
14
2
3
5
1
19
21
8
2
8
11
9
10
9
1
2
17
34
3
10
Oct. '14 Nov. '14 Dec. '14 Jan. '15 Feb. '15 Mar. '15
Liberia Multiple Countries* Guinea Sierra Leone Unknown** Mali Treated Patient in US
Low, But Not Zero,
Risk
95%
Not interviewed
3%
Some Risk
2%
0
5
10
15
20
25
30
35
Oct. '14 Nov. '14 Dec. '14 Jan. '15 Feb. '15 Mar. '15
Hours
24 Hour Goal First Attempted Contact Time Interview Time
Percentage of Missing Time Logs
Month Oct. '14 Nov. '14 Dec. '14 Jan. '15 Feb. '15 Mar. '15
Interview Time 82.1% 25.0% 24.5% 13.7% 15.9% 0.0%
First Attempted Contact Time 92.9% 46.2% 60.2% 26.0% 19.5% 19.0%
Hartsfield–Jackson
1.0%
John F. Kennedy
8.8%
Newark Liberty
1.6%
O'Hare
0.3%
Transfers*
6.7%
Toronto
Pearson
0.3%
Washington Dulles
81.1%
Unknown
0.3%
Other
3.4%
30%
40%
50%
60%
70%
80%
90%
100%
Oct. '14 Nov. '14 Dec. '14 Jan. '15 Feb. '15 Mar. '15
% of Recent Travelers
Successfully Contacted Interviewed within 24 hours
23
54
42
50
41
1
20
15
22
5
Oct. '14 Nov. '14 Dec. '14 Jan. '15 Feb. '15 Mar. '15
NumberofCalls
Total Calls Transferred Calls
DC DOH Recent Traveler Contact Protocol
LESSONS LEARNED
While leading to a high successful contact rate, manual reminders and
contact attempts proved to be time intensive for staff and did not lead to
all travelers successfully interviewed within 24 hours of receiving arrival
notifications. In the future, automated reminders could help improve the
timeliness of successfully interviewing travelers.