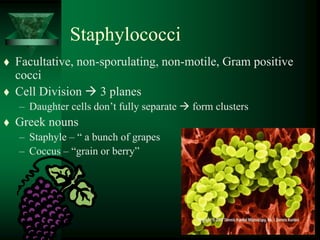
4. Staphylococci
27 species Three Important Species
Staphylococcus aureus
– Important human pathogen
Staphylococcus epidermidis
– Normal skin flora, disease under special circumstances
Staphylococcus saprophyticus
– UTI’s in young females
6. S. aureus - Epidemiology
Reservoir – Humans
Asymptomatic Carriage Sites:
– Nares
– Rectum
– Perineum
– Pharynx
Skin Colonization - Brief, Repeated
Transmission - Person to Person
7. S. aureus Carriage Rates
Population Carriage Rate (%)
General Population 25
Hemodialysis 75
Diabetic on insulin 50
Patients receiving 50
allergy shots
Intravenous Drug Users 40
17. A 22-month-old boy with a
staphylococcal folliculitis on the buttocks.
The lesions have been excoriated. Diaper
occlusion may have been related to onset
of the rash.
18. Furuncle
Often starts as infection of
hair follicle Folliculitis
Firm, tender red nodule
Painful
Fluctuant with time Drain
spontaneously
33. Impetigo
• The most common skin infection in
children.
• Causative agent is carried in the nasal area.
• Bacteria invade the superficial skin.
34. Impetigo
Superficial infection of skin
Usually
– S. aureus
– Streptococcus pyogenes
Children
Hot Weather
Minor Trauma
Initially vesicles
39. Interventions
•Good general hygiene
•Wash gently with soap and water
•Topical antibiotic therapy
•Wash hands
•Systemic antibiotics only if severe
and does not respond to topical.
(keflex po)
44. Cellulitis
A full-thickness skin infection
involving dermis and underlying
connective tissue.
Any part of the body can be
affected.
Cellulitis around the eyes is usually
an extension of a sinus infection or
otitis media.
46. Assessment
History and physical exam
WBC count
Blood culture
Culturing organism from lesion
aspiration.
CT scan with peri-orbital cellulitis
47. Clinical Manifestations
Characteristic reddened or lilac-
colored, swollen skin that pits when
pressed with finger.
Borders are indistinct.
Warm to touch.
Superficial blistering.
70. Interventions
Hospitalization if large area involved
or facial cellulitis.
IV antibiotics.
Pain management.
Warm moist packs to area if ordered.
Assess for spread
If peri-orbital test for ocular
movement and vision acuity
76. Expansion of abscess
Periosteal elevation
Shearing of arteries
Subperiosteal
abscess
Reactive bone
Ischemia = osteonecrosis (sequestrum)
Pyogenic osteomyelitis -pathogenesis
77. Pus in joint
Extension into soft tissue
Draining sinus
Skin
Cortical necrosis =
sequestrum
Reactive bone surround
sequestrum: involucrum
Continuous resorption
Continuous new bone
and fibrosis of marrow
sequestrum
Pyogenic osteomyelitis -pathogenesis
93. Patterns of Disease - S. aureus
1) Invasion with Tissue Destruction
2) Toxin Mediated
– Toxic Shock Syndrome
– Scalded Skin Syndrome
– Staphylococcal Food Poisoning
94. TOXIC SHOCK SYNDROME
Acute Febrile Illness
Subsequent Development of Hypotension
and Shock.
Noted association with S. aureus phage
group I
Named the illness "Toxic Shock Syndrome“
95. TOXIC SHOCK SYNDROME
1990 - More than 3,300 cases have been
reported
95% in women
90% occurred during menstruation in
women who were using tampons
1989 - 61 cases of TSS reported
96. Toxic Shock Syndrome -
Epidemiology
1. Menstrual
Colonization of the Vagina and Cervix
with TSST-1 producing strains of S.
aureus
– Tampon Associated
• Risk proportional to the absorbancy of Tampon
– Not tampon associated
98. Pyrogenic Toxin
Family of Proteins secreted by
– S. aureus
– Strep pyogenes
Include
– TSST-1
– Staphylococcal Enterotoxins A, B,C
– Pyrogenic Exotoxin A & B
– Streptococcal Scarlet Fever Toxins A, B,C
99. Toxic Shock Syndrome
- Clinical Manifestations
1. High Fever (>39.9oC)
2. Scarlatiniform Eruption
3. Hypotension and Shock
4. Desquamation during
convalescence
100. Staphylococcal toxic shock
syndrome
Toxic shock syndrome (TSS)
Toxic shock syndrome toxin
(TSST-1)
Super antigen
Tampon or infected wound, TSST-
1 enters blood stream and cause
fever, rash, exfoliation of skin and
shock (death rate 3%)
101. Manifestations of Specific Organ
Involvement
Mucous Membranes: hyperemia
Gastrointestinal Tract: vomiting and diarrhea
Muscle: severe myalgias
Central Nervous System: disorientation
Kidney: azotemia, pyuria urinary tract infection
Liver: elevation of serum bilirubin and SGOT
Blood: Thrombocytopenia
102. Toxic Shock Syndrome -
Diagnosis
• Isolation of toxin producing S. aureus
from a patient with a compatible
clinical illness.
103. Toxic Shock Syndrome -
Treatment
1) Treatment of Hypotension and Shock
– Vigorous Fluid Replacement
2) Attention to the Site of S. aureus Colonization
– Removal of Tampons
– Drainage of Staphylococcal Abscess
3) Anti-Staphylococcal Antibiotic Therapy
104. STAPHYLOCOCCAL SCALDED SKIN SYNDROME
A Disease of Infants
– Localized Infection with Diffuse Skin Rash
S. aureus (Phage group II) recovered from:
– Nose
– Pustules
– Eye
– Umbilicus
Exfoliative Toxin
– Two Serologically and Biologically Distinct Proteins
• Exfoliatin A
• Exfoliatin B
– Inter-Epithelial Splitting of Stratum Granulosum Layer
105. Staphylococcal Scalded Skin Syndrome -
Clinical Features
Starts Abruptly
– Perioral erythema
– Sunburn like, tender rash
spreads over entire body
Bullae Appear Rapidly
– Nikolsky sign
– Flaccid bullae slough off
Denuded areas
106. Staphylococcal Scalded Skin Syndrome -
Clinical Features
Exfoliated Areas Eventually Dry
– Flaky desquamation lasting 3-5
days
Within 10 days After Onset
Complete Recovery
– New epidermis has replaced the
denuded areas
110. Staphylococcal Food Poisoning
20% of Outbreaks of Acute Food
Poisoning
Toxigenic Strain of S. aureus growing in
contaminated food
– Produces Enterotoxin B (Heat Stable)
Person to Person Transmission
– Responsible organism usually isolated from person
involved meal preparation
111. Staphylococcal Food Poisoning
Commonly implicated foods
– Custard filled bakery good
– Canned food
– Potato salad
– Ice cream
Food appears normal in
appearance, odor and taste
112. Staphylococcal Food Poisoning -
Clinical Features
Incubation period 2-6 hours
Enterotoxin stimulates intestinal
peristalsis and CNS
– Abrupt onset:
• Salivation
• Nausea and vomiting
• Abdominal cramps
• Watery diarrhea
Afebrile
Self limited, symptoms disappear in 8 hours
113.
114. S. aureus
Evolution of Drug Resistance in S. aureus
Methicillin
[1970s]
Methicillin-
resistant
S. aureus (MRSA)
S. aureus
Penicillin
[1950s]
Penicillin-resistant
Vancomycin-resistant
enterococci (VRE)
Vancomycin
[1990s]
[1997]
Vancomycin
intermediate-
resistant
S. aureus
(VISA)
[ 2002 ]
Vancomycin-
resistant
S. aureus
115. Bone5:
7%–13%
Vancomycin Penetration
Sternal Bone1:
57%
Heart Valve4:
12%
CNS:
<10%
Fat4:
14%
Muscle4:
9%
Epithelial
lining fluid3:
18%
Lung tissue2:
17%–24%
1. Massias L et al. Antimicrob Agents Chemother. 1992;36:2539-2541; 2. Cruciani M et al. J Antimicrob
Chemother. 1996;38:865-869. 3. Lamer C et al. Antimicrob Agents Chemother. 1993;37:281-286;
116. MRSA in Europe.
In England and Wales, from
January to December 1999
methicillin resistance was
37% of the S.aureus reports.
Except Scandinavia and
Netherlands most countries
have high rates of MRSA.
119. Reservoir for the Spread of
Antibiotic Resistant Pathogens
clinical
infections
colonized
(asymptomatic)
120. Standard Precautions for Health
Care workers include:
Hand hygiene / handwashing- before and after
patient contact and after touching contaminated
items
Gloving - when touching blood, body fluids,
secretions, excretions,and contaminated items
Masking – if aerosol of infectious material
expected
Gowning
Appropriate handling of laundry
121. Most common mode of
transmission of pathogens is via
hands!
So Why All the Fuss About
Hand Hygiene?
122. The Inanimate Environment Can
Facilitate Transmission
~ Contaminated surfaces increase cross-transmission ~
Abstract: The Risk of Hand and Glove Contamination after Contact with a
VRE (+) Patient Environment. Hayden M, ICAAC, 2001, Chicago, IL.
X represents VRE culture positive sites
123. Staphylococcus epidermidis
Normal Flora
– Virtually all humans carry S. epidermidis on the skin
and in and around body orifices
Hospital Acquired Infection
– Contamination by S. epidermidis carried by the patient
• most important event in infections associated
with foreign bodies
125. S. epidermidis - Patterns of Infection
Nosocomial Bacteremia -most common cause
Endocarditis
A. Native Valve
– Uncommon- 5% of cases
B. Prosthetic Valve
– Single most common cause (40% of cases)
– Probably caused by inoculation at the time
of surgery
– Indolent course
126. S. epidermidis - Patterns of Infection
Intravenous Catheters
-Single most common cause (50-75% of cases)
Cerebrospinal Fluid Shunts
Peritoneal Dialysis Catheter
Vascular Grafts
Prosthetic Joints
127. S. epidermidis Infection -
Treatment
1. Antimicrobial Therapy
Usually resistant to multiple antibiotics
– Beta lactams
– Erythromycin, Clindamycin, Tetracycline
Require therapy with Vancomycin
2. Removal of Foreign Body
128. Staphylococcus saprophyticus
Colonizes the genitourinary mucosa of some young
women
Causes both upper and lower urinary tract disease
– 95% of cases are in females 16-35 years old
– Responsible for 20% of the UTI's in this age group
• Second only to E. coli
Pathogen of young, sexually active females
– 70% sexual intercourse within 24 hours preceding onset of
symptoms