Healthcare Market Overview, May 2024: Funding, Financing and M&A, from Oppenh...
Sample Pain Clinic Referral Form
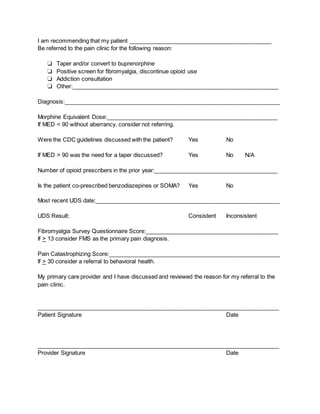
1. I am recommending that my patient _____________________________________________
Be referred to the pain clinic for the following reason:
❏ Taper and/or convert to buprenorphine
❏ Positive screen for fibromyalgia, discontinue opioid use
❏ Addiction consultation
❏ Other:_________________________________________________________________
Diagnosis:____________________________________________________________________
Morphine Equivalent Dose:______________________________________________________
If MED < 90 without aberrancy, consider not referring.
Were the CDC guidelines discussed with the patient? Yes No
If MED > 90 was the need for a taper discussed? Yes No N/A
Number of opioid prescribers in the prior year:_______________________________________
Is the patient co-prescribed benzodiazepines or SOMA? Yes No
Most recent UDS date:__________________________________________________________
UDS Result: Consistent Inconsistent
Fibromyalgia Survey Questionnaire Score:__________________________________________
If > 13 consider FMS as the primary pain diagnosis.
Pain Catastrophizing Score:______________________________________________________
If > 30 consider a referral to behavioral health.
My primary care provider and I have discussed and reviewed the reason for my referral to the
pain clinic.
____________________________________________________________________________
Patient Signature Date
____________________________________________________________________________
Provider Signature Date