Call Girls Jabalpur Just Call 9907093804 Top Class Call Girl Service Available
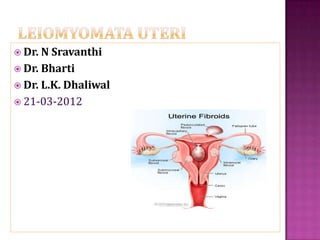
Leiomyomata uteri
1. Dr. N Sravanthi
Dr. Bharti
Dr. L.K. Dhaliwal
21-03-2012
2. A LEIOMYOMA is a benign monoclonal tumour composed of smooth
muscle cells but containing various amounts of fibrous connective
tissue. Its well circumscribed but not encapsulated.
Various terms to refer these tumors :
fibromyoma,
myofibroma,
leiomyofibroma,
fibroleiomyoma,
Myoma
Fibroma
Fibroid
3. Most common benign tumours of uterus and female pelvis.
In 20 – 40 % women in reproductive age group.
About one third of hospital admissions to gynecology services.
Reported to occur in 77% of uteri obtained from TAH specimens
The hysterectomy specimens from
premenopausal women - 7.6 myomas;
postmenopausal women - 4.2 myomas
4. Precise cause is unknown
Genetic factors – 40% have chromosomal abnormalities
(t:12,14), (del 7) (trisomy 12)
Hormones
Estrogen and progesterone appear to promote development
Growth factors
TGF – β, bFGF, EGF, PDGF, IGF, PRL
5. Age (increases with age)
Ethnicity ( African women 2.9 times than White )
Endogenous hormonal factors
Weight ( 21% increased risk with every 10kg rise body weight)
Diet and Exercise and Obesity
Family history/genetic predisposition(first degree relative- 2.5
times increases risk)
Oral contraceptives(no definite relationship)
Menopausal HRT: Therapy will not stimulate growth
Parity( nulliparous > multiparous )
Smoking (reduced)
Tissue injury
6. Benign tumors that originate from smooth muscle cells of the
uterus
Range in size from seedlings to large uterine tumors
solitary or multiple
Depending on the location
Within the myometrium (intramural)
Externally extending to the serosa (sub serous)
internally impinging on the uterine cavity (submucous)
10. In one-third of patient
Usually menorrhagia, but also can present as metrorhhagia or as
menometrorrhagia.
Associated with any type of fibroids, but there is a distinct clinical
pattern with each type.
Bleeding is more common and severe in in submucous fibroids.
11. The submucous leiomyoma bleeds freely at menstruation and may
also bleeds between periods
If the submucous myoma is pedunculated, there is usually a
constant, thin, blood-tinged discharge in addition to the menorrhagia.
Intramural myoma beginning to encroach the uterine cavity can also
present as menorrhagia.
Intramural fibroid near serosa, pedunculated serous tumours can also
present with abnormal bleeding.
12.
13. a) Increased surface area
b) Local hyperestrogenism in areas adjacent to the submucous
tumor, endometrial hyperplasia and endometrial polyps.
c) Thinning and ulceration of the endometrial surface
d) Interference with myometrial and spiral arteriolar(basalis
portion) contractility
e) Congestion and Endometrial venule ectasia
15. Abdominal and pelvic discomfort, Feeling of heaviness in
pelvis, Dyspareunia
Spasmodic dysmenorrhoea
Torsion in pedunculated myoma
Red degeneration
Diffuse adenomyosis
Concomitant pelvic disease: ovarian
pathology, PID, endometriosis, urinary tract or intestinal
pathology
16. In 5-10% of infertile women
Only 2-3% of infertility may attributed to
them(provided other causes have been excluded)
“Removal of fibroids that distort the uterine cavity
may be indicated in infertile women, where no
other factors have been identified, and in women
about to undergo in vitro fertilization treatment.”
SOGC CLINICAL PRACTICE GUIDELINES
No. 128,May 2003
17. Mechanisms:
Interference with sperm transport, ovum capture
Displacement of cervix
Deformity of uterine cavity
Distorted adnexal anatomy
Obstruction of proximal fallopian tubes
Interference with implantation
Increased or disordered uterine contractility
Local inflammation
Impaired blood flow
18. Common during pregnancy
OCPs containing high dose of estrogens
HOWEVER – “Rapid growth in post-menopausal women is
highly suggestive of malignancy”
Sarcomatous change in leiomyoma
Sarcoma
Carcinoma endometrium
Estrogen secreting ovarian neoplasm
19. Incidence of leiomyosarcoma in hysterectomy specimens
of women receiving surgical treatment for fibroid
0.1% in reproductive age group
1.7% after age of 60 years
Leiomyosarcoma in a series of hysterectomies performed for presumed uterine
leiomyomas.
Am J Obstet Gynecol 1990;162:968–76
20. Careful history regarding symptoms.
Bimanual pelvic examination : (enlarged, irregularly
shaped, firm, and non-tender uterus )
21. Ultrasound (TAS and TVS)
best initial test based on its noninvasive nature and cost-
efficiency.
lowest sensitivity and specificity
concentric, solid, hypo echoic masses
anechoic components - from necrosis.
Calcifications are hyper-echoic, with sharp acoustic
shadowing
22.
23. Provides contrast
Better defines submucous myomas, polyps, endometrial
hyperplasia, or carcinoma
Precisely defines the location, attachment of the submucous
fibroids and also determines whether it is amenable to
hysteroscopic resection
Limitation of detection of leiomyomata is o.5 cm diameter.
24. More sensitive(64%) and specific(88%) than US
Evaluation of number , size, and position of sub-
mucosal, intramural fibroids and sub serous fibroids.
Allows precise myoma mapping - Helpful in planning surgery
May differentiate adenomyosis from myomas.
(adenomyosis is associated with junctional zone thickness of
more than 15mm (or 12 mm in a non-uniform junctional
zone).
Focal, not well-demarcated, high-intensity or low-intensity
areas in the myometrium also correlate with adenomyosis)
Expensive modality
25. FIGO classification system (PALM-COEIN) for causes of abnormal uterine
bleeding in nongravid women of reproductive age
28. Women who are mildly or moderately symptomatic with
fibroids – observation may allow the treatment to be
deferred, perhaps indefinitely.
“As women approach menopause, there is limited time for new
symptoms and after menopause the bleeding stops and the
fibroids decrease in size.”
Except for women with
Severe anemia from fibroid related menorrhagia
Or hydronephrosis from ureteric obstruction from a massively
enlarged fibroid uterus
29. Risk of malignancy is less than 0.1%.
“There is currently no evidence to substantiate
performing a hysterectomy for an asymptomatic
leiomyoma for the sole purpose of alleviating the
concern that it may be malignant.”
SOGC CLINICAL PRACTICE GUIDELINES
No. 128,May 2003
30. GnRH AGONISTS :
Treatment reduces the uterine volume, fibroid
volume(30%), and bleeding with resultant increase in
hemoglobin.
Menses return in 4-8weeks after discontinuation, and uterine
size returns to pre-treatment levels within 4-6 months
SIDE EFFECTS : hot flushes, vaginal dryness, transient
frontal
headaches, arthralgia, myalgia, insomnia, edema, emotiona
l lability, depression, and decreased libido.
SURGICAL DRAWBACK S:
potential difficulties with enucleation of the myoma and longer intra-
operative times,
an inability to distinguish and remove smaller myomas at risk to regrow
31. “The hypo-estrogenic state induced by GnRH agonists causes significant bone
loss after six months of therapy”
Low doses of estrogen and progestins may be added in an effort to reduce
the side effects and inhibit bone loss and allow long term use.
GnRH Agonists as temporary treatment for Peri-menopausal women may
be considered.
32. GnRH antagonists : (Ganirelix) immediate suppression of endogenous
GnRH.
Progesterone mediated treatment :
Mifepristone (RU 486 )
RISK OF ENDOMETRIAL HYPERPLASIA
Progesterone releasing IUD : LNG-IUS may reasonable for selected
women with fibroid associated menorrhagia( <12 weeks, regular
cavity)
Decrease in mean estimated blood loss and increase in hemoglobin but no
decrease in uterine volume
Progesterone receptor modulators:
ASNOPRISNIL
33. Serious medical conditions, such as severe anemia or ureteral
obstruction, often need to be addressed surgically.
Surgical intervention may also be indicated in women who have
myomas that are associated with menorrhagia, pelvic pain or
pressure, or urinary frequency or incontinence that compromises
quality of life.
Women with large symptomatic myomas who have completed
childbearing are most often recommended to have a hysterectomy.
34. Abnormal uterine bleeding not responding to conservative
treatments
Infertility when there is distortion of the endometrial cavity or
tubal obstruction
Recurrent pregnancy loss (with distortion of the endometrial
cavity)
Pain or pressure symptoms (that interfere with quality of life)
Urinary tract symptoms (frequency and/or obstruction)
Anemia secondary to chronic blood loss
High level of suspicion of pelvic malignancy
Growth after menopause
ACOG, VOL. 104, NO. 2, AUGUST 2004
35. Myomectomy should be considered as alternative to hysterectomy .
May be considered in women with large fibroids and wish to retain
uterus and desire child bearing.
36. Pre operative correction of anemia:
Iron supplementation
Blood transfusion
Erythropoietin alfa/ epoetin
GnRH Agonist Treatment:
mitigate the bleeding
Result in increase in hemoglobin.
37. MANAGING BLOOD LOSS :
Pre operative GnRH agonists treatment
Hypotensive anaesthesia
Vasopressin(20U in 20 ml NS) - as effective as vascular
occlusion for controlling blood loss
Tourniquets :
Bonney’s myomectomy clamp
Ring forceps
Elastic rubber catheter(around cervix)
Rumel’s Type tourniquet
38. Adequate exposure of the operative field.
Avoid traumatic instrumentation and injury to the serosa.
Sutures on serosal surface should be of fine absorbable non reactive
material.
Evaluate the size, number and location of myomas, and their proximity
to the endocervical canal, uterine vessels, and fallopian tubes.
Careful planning of uterine incisions. Aim should be removal of all
myomas through a single incision made in anterior uterine corpus and in
the midline to avoid vascular areas and broad ligament laterally
39.
40.
41. Traditionally used for submucous myomas.
When submucous myoma becomes pedunculated myoma can be
delivered gradually through the dilated cervix.
After satisfactory pre-op. preparation, and broad spectrum
antibiotics, vaginal myomectomy should be performed in the
operating room.
One should avoid too much of downward traction(may cause
uterine fundal inversion).
Pedicle is identified and clamped as high as possible within the
uterine cavity and ligature is applied.
In case of brisk bleeding tamponade with inflated Foley’s balloon
can be done.
42. Mainly for submucous myomas.
Successful in treating the menstrual symptoms.
Menorrhagia is controlled in 90% patients.
Usually performed under laparoscopic guidance to prevent
inadvertent perforation.
In selected women who are not desirous of future
fertility, endometrial ablation may be efficacious in treating
abnormal bleeding.
43.
44. LESS POST OPERATIVE PAIN, SHORTER HOSPITAL STAY AND
SHORTER RECOVERY THAN ABDOMINAL MYOMECTOMY
Limitations :
Difficult to remove in certain locations.
Large or multiple fibroids.
When myomas are embedded deep in the myometrium.
Retrieval of myomas could be a problem, morcellation may be required
Larger myoma can be removed vaginally through a posterior colpotomy
incision.
Conversion to laparotomy rate 7.5%
Complication rate 3.8%
45.
46.
47.
48.
49. Significant disadvantage is post- operative pelvic adhesions
Overall rate 35 -40%
Rate of adhesion per myomectomy site 15 – 20%
Rate of adhesion on adnexa 25%
Risk factors for adhesion:
Use of uterine sutures
Posterior uterine wall myomas
Prior existence of pelvic adhesions
50. A. INTERCEED : Oxidized regenerated cellulose can
be placed over uterine corpus to protect the tubes
and ovaries from the denuded peritoneal surfaces
and uterine incision.
51. B. GORE-TEX (Polytetrafluoroethylene surgical
membrane) :
Non absorbable barrier
Can be sutured over the uterine incisions
C. SEPRAFILM :
Bioresorbable membrane
Sodium hyaluronate and carboxymethyl cellulose
Reduce the incidence, severity, extent and areas of uterine
adhesions after myomectomy.
D. GnRH ANALOGUES
52. Percutaneous cannulation of femoral artery
Embolization of uterine artery and its branches accomplished by
injecting gelatin sponges, Poly Vinyl alcohol particles, tris-acryl gelatin
microspheres via catheter until occlusion/ or slow flow.
Total radiation exposure (approx 5cGy).
Effects on early ovarian failure, fertility and pregnancy are unclear.
Appropriate candidates for UAE include women who have symptoms
severe enough to warrant hysterectomy or myomectomy.
53.
54.
55. CONTRAINDICATIONS :
Active pelvic infection
Severe contraction medium allergy
Arteriovenous malformations
Desire for future pregnancy
Pedunculated myoma
Undiagnosed pelvic mass.
56. COMPLICATIONS :
Post-procedural pain
Post embolisation syndrome
Early Ovarian Failure(controversial)
Effects on Fertility and Pregnancy (possibility of
decreased ovarian reserve and potential for increased
pregnancy complication, women who wish to conceive
should not be treated with UAE)
57. Uses high-intensity ultrasound waves that are focused into a small area
of between 4 – 16mm, to produce heat and energy, which kills the
tumor cells.
Concurrent MRI allows
precise targeting of the tissue as well as to
monitor the temperature of treated tissues
Not recommended for women wishing future fertility
ADVANTAGES:
Very low morbidity
Rapid recovery with return to normal life
58.
59.
60. Observed in 2.7% - 12.6% of pregnant women
EFFECTS OF PREGNANCY:
Most do not increase in size during pregnancy.
Pregnancy has a variable and unpredictable effect on myoma
growth, likely dependent on individual differences in
genetics, circulating growth factors, and myoma-localized
receptors.
A reduction in myoma size was observed 4 weeks after delivery.
61. EFFECTS ON PREGNANCY:
Very rarely lead to an unfavorable pregnancy outcomes.
Cesarean section more common among women with fibroids.(23% Vs 12%)
However , there is increases risks of
preterm delivery(19.2% Vs 12.7%)
Placenta previa(3.5% Vs 1.8%)
Post partum hemorrhage(49.1% Vs 21.4%)
Malpresentation
“Uterine rupture during pregnancy or delivery as a consequence of
abdominal myomectomy appears to be rare.”
62. Although new myomas may grow after
myomectomy, most women will not require
additional treatment.
Myomas detected after myomectomy, often
referred to as recurrence, either are the result of
persistence of myomas left at the time of
surgery or are newly developed myomas.
63. Clinical exam alone may not be effective in
assessing the incidence of new appearance of
myomas, because women who return to the
gynecologist are more likely to have gynecologic
problems associated with new myomas than are
women who remain asymptomatic
64. Routine ultrasound follow-up is sensitive but
detects many clinically insignificant myomas.
Meaningful information for a woman with myomas
considering treatment is her approximate risk of
developing symptoms that would require yet
additional treatment.
65. Age
Subsequent childbearing
Number of myomas initially removed
Gonadotropin-releasing hormone agonists
Laparoscopic myomectomy