Uterine Fibroid / Uterine Leiomyoma / Indore Infertility
•Download as PPTX, PDF•
12 likes•971 views

Definition of fibroid / uterine leiomyoma Diagnosis of Fibroid Treatment of uterine fibroid Surgery for uterine fibroid When is surrogacy required for fibroid By Dr Gajendra Tomar, Indore Infertility Clinic, IVF center

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Uterine Fibroid / Uterine Leiomyoma / Indore Infertility
Similar to Uterine Fibroid / Uterine Leiomyoma / Indore Infertility (20)
Recently uploaded
Recently uploaded (20)
Uterine Fibroid / Uterine Leiomyoma / Indore Infertility
- 2. Uterine Leiomyoma : Introduction Commonest benign solid tumor in females Incidence : Age dependent : Around 25-30 % Smooth muscle + Fibrous connective tissue Fibroid / Uterine Leiomyoma / Fibromyoma Neoplastic single smooth muscle cell of the myometrium (Monoclonal) Leading indication of Hysterectomy
- 3. Causes Etiology still unclear Chromosomal : 40 % cases Polypeptide growth factors Hormones Familial (RR 2.5)
- 4. Hormones Predominantly an Estrogen-dependent tumor Both P & E promote development Serum Levels of E & P are same High Aromatase causes denovo production of estrogen Increased Progesterone receptors – High mitotic counts
- 5. Factors That Affect the Risk of Uterine Fibroids High Risk Low Risk Early Menarche Late Menopause Late menarche Early Menopause Obesity Exercise Nulliparity Increased Parity African descent Smoking High dose Oral contraceptive pills Low Dose Oral contraceptive pills
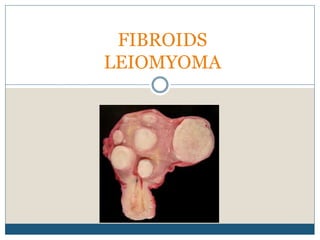
- 8. Fibroids: Composition • Round, firm, and well-circumscribed nodules • Cut section shows whorled appearance • False capsule • There are often multiple tumours in a single uterine specimen. They do not have a true capsule. • They range in size from seedlings to large uterine tumours.
- 9. Histology Whorled (fascicular) pattern of Smooth Muscle (SM) bundles separated by well vascularized connective tissue Pseudocapsule : part of the myometrium which compresses the leiomyoma.
- 10. Histology SM cells elongated with eosinophilic distinct cell membranes May develop areas of degeneration if large including; hyaline/mucoid/Calcified/Cystic Usually < 5 mitotic figures per 10 HPFs Post lupron treatment: initially edema and necrosis, then hyalinization and mild lymphocytic infiltrate
- 11. Origin
- 12. Diagnosis Gynaecology assessment: • History • Abdominal-vaginal exam • Speculum assessment • Assess fibroid size Investigations: • Menstrual diary • Pelvic US • Saline TVUS (SIS) • Hysteroscopy +/- Laparoscopy • MRI (+/- contrast Gadolinium)
- 13. Pelvic Ultrasound Readily Available Cost Effective Symmetric, Well Defined, Hypoechoic Degenerative changes may change appearance 90-95 % Sensitive but may miss submucosal fibroids
- 14. Pelvic Ultrasound SIS Submucosal fibroids Very high sensitivity and specificity
- 15. Saline Infusion Sonography Mainly for submucosal fibroids Very high sensitivity and specificity
- 16. MRI Accurate assessment of size, number and location Not technique dependent Low interobserver variation Impact on surrounding organs Conservative fertility preserving surgeries : Greater role. Adenomyosis vs fibroid : Clear (Junctional zone is more than 15mm, high and low intensity areas in the myometrium)
- 17. MRI Imaging
- 19. The role of Diagnostic Hysteroscopy Classify fibroid(s) and suitability for resection Option of ‘see and treat’ Evaluate size and contour of endometrial cavity and morphology of endometrium. Exclude concomitant pathology (e.g. endometrial thickening, polyps, focal change/cancer).
- 21. USG / Hysteroscopy / Laparoscopy
- 24. Fibroids and Pregnancy Fibroid on Pregnancy Mostly uneventful 2/3rd Increased rate of spontaneous miscarriage preterm labor , placenta abruption Malpresentation, labor dystocia cesarean delivery postpartum hemorrhage Pregnancy on Fibroid Variable and Unpredictable 2/3rd : No change 1/3rd : Increase Growth usually limited almost exclusively to the first trimester Reduction in size towards pre pregnant – 4 weeks https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2876319/
- 25. Red Degeneration Carneous Degeneration Large fibroid Mainly during second half of pregnancy and puerperium. The cause is not known but is probably vascular in origin. Infection does not play any part. Naked eye appearance of the tumor shows dark areas Cut section revealing raw-beef appearance often containing cystic spaces. Color is due to the presence of hemolysed red cells and hemoglobin. Microscopically, evidences of necrosis are present. Vessels are thrombosed but extravasation of blood is unlikely
- 26. Red Degeneration : Diagnosis and Management during pregnancy Pain, Vomiting, and Fever Raised leucocytes, Raised CRP Acute appendicitis, sub acute salpingo-oophoritis, Torsion of pedunculated subserosal leiomyoma, threatened abortion Management: Conservative and symptomatic
- 27. Sarcomatous changes less than 0.1 percent cases. The usual type is leiomyosarcoma High Suspicion • Recurrence of fibroid polyp • sudden enlargement of fibroid • Pain, Bleeding, Closer to menopause Diagnosis • Serum LDH • GD Enhanced MRI : Increased vascularity & perfusion
- 28. Differential diagnosis (1) Pregnancy (2) Full bladder (3) Adenomyosis (4) Myohyperplasia (5) Ovarian tumor
- 30. Do nothing Asymptomatic fibroids Mild to moderate symptoms that aren't significantly affecting everyday activities. Fibroids usually shrink after the menopause, and symptoms ease or resolve.
- 31. Symptomatic Medical Management Nonsteroidal anti-inflammatory drugs (NSAIDs) have been a regular solution for pain Tranexamic acid : procoagulant drug : reduces blood loss in cases of mild bleeding
- 32. Combination Oral Contraceptive Pills In the past considered a risk factor Suppressive effects on endometrial proliferation No effect on decreasing uterine fibroid volume or uterine size Easy accessibility, oral administration, and low cost
- 33. Progestins Lack of high-quality evidence May even promote uterine fibroid cell growth Associated with histopathological changes that may be mistaken for leiomyosarcoma or smooth-muscle tumors of unknown malignant potential
- 34. LNG-IUS Causes Endometrial atrophy Improvement in menstrual bleeding and hemoglobin levels No appreciable change in fibroid volume Effective for up to 5 years, Minimal side effects are reported No additional patient's compliance after insertion Symptomatic women with no endometrial distortion If cavity is distorted, expulsion rates are high
- 35. GnRH Agonists GnRH agonists are synthetic peptides with longer half-life than native GnRH Increase (FSH) and (LH) secretion : flare effect After that, receptor down-regulation, followed 1–3 weeks later by a hypogonadotropic hypogonadal state, often termed — “pseudomenopause” Induced Hypoestrogenic state
- 36. GnRH Agonists Significant improvement in both pre- and postoperative hemoglobin levels Significant reductions in uterine volume, fibroid volume More beneficial in cases of large uterine fibroids (>10 cm) if myomectomy is to be performed, thus reducing operative time, intraoperative bleeding, and the risk of blood transfusion
- 37. GnRH Agonists Drawbacks Menopausal symptoms, such as hot flashes and atrophic vaginitis, and a decrease in bone mineral density (BMD) after long-term use limit GnRH agonists. Myoma degeneration and obliteration of the interface between the myoma and myometrium, making removal difficult Small uterine fibroids that become too soft and difficult to visualize : may be missed
- 38. SPRMs Progesterone stimulates proliferative activity in uterine fibroid cells, but not in normal myometrial cells Compared with myometrium, fibroids overexpress ERs and progesterone receptors (PRs) GnRH with addback P Mifepristone is thought to have almost pure antagonistic properties Other SPRMs such as ulipristal acetate exhibit mixed agonist and antagonist properties Novel PRM-associated endometrial changes
- 39. Mifepristone Mifepristone (RU-486) is a progesterone receptor modulator that has almost pure antagonistic properties and may directly decrease the PR in the myometrium and leiomyoma Significantly reduced uterine and leiomyoma volume and related symptoms 2.5 mg daily for 3 to 6 months as the optimum treatment. Insufficient Evidence : Atypical endometrial hyperplasia
- 40. Ulipristal Acetate Exhibits anti proliferative effects on leiomyoma cells and the endometrium Repeated intermittent 3-month open-label UPA courses Decreased uterine bleeding symptoms with treatment As effective as leuprolide acetate in controlling heavy menstrual bleeding
- 41. Ulipristal Acetate Rapid control of the symptoms decreasing volume by 50% after 12 months of treatment, Similar manner as GnRH analogs, excellent safety and tolerability profile Amenorrhea in 80% of the patients Considered as a first-line treatment once symptomatic treatment is not effective Surgery, when necessary, is not compromised Combination with another treatment method, like LNG- IUS, is recommended after finishing UPA
- 42. Others SERM’s AI https://www.ncbi.nlm.nih.gov/pmc/articles/PM C5592915/ https://www.jogc.com/article/S1701- 2163(15)30338-8/pdf https://www.aafp.org/afp/2017/0115/p100.html https://www.ncbi.nlm.nih.gov/pmc/articles/PM C5854898/
- 43. Surgical & Other non Medical Modes Hysterectomy Myomectomy Conservative Radiological Interventions
- 44. Hysterectomy In women who have completed childbearing, hysterectomy Permanent solution for symptomatic leiomyomas The only indications for hysterectomy in a woman with completely asymptomatic fibroids are enlarging fibroids after menopause without HRT
- 45. Type of hysterectomy Abdominal, Laparoscopic, or Vaginal route : Surgeon’s training, experience, and comfort Abdominal supracervical or total hysterectomy : randomized trials have demonstrated no differences in sexual and urinary function Less blood loss and complications associated with supracervical hysterectomy
- 46. Vaginal hysterectomy Preferred technique provides several statistically significant advantages, decreased blood loss, shorter hospitalization, and shorter paralytic ileus time limited by the size of the myomatous uterus. Abdominal hysterectomy is an alternative approach
- 47. Laparoscopic Hsyterectomy The laparoscopic extraction of the uterus may be performed with morcellation Rotating blade cuts the tissue into small pieces. This technique has come under scrutiny because of concerns about iatrogenic dissemination of benign and malignant tissue
- 48. Myomectomy Women who wish to retain their uterus, regardless of their fertility desire. Well planned, site, size, number. Women should be counselled about the risks of requiring a hysterectomy at the time of a planned myomectomy. Five years following laparoscopic myomectomy, the cumulative probability of recurrence in women who subsequently gave birth was 42%. In those who did not give birth, it was 55%
- 49. Myomectomy Hysteroscopic Myomectomy Laparosocopic Myomectomy Open Myomectomy
- 50. Hysteroscopic Myomectomy Submucous myomas (types 0, I, and II) up to 4 to 5 cm in diameter can be removed hysteroscopically. Type II myomas are more likely to require a 2-staged procedure Risk of excessive fluid absorption and uterine perforation, particularly with those with less than 5 mm thickness between the fibroid and the uterine serosa
- 51. Laparoscopic myomectomy is a procedure associated with less subjectively reported postoperative pain, lower postoperative fever and shorter hospital stay No evidence suggested a difference in recurrence risk After the completion of myomectomy, application of antiadhesion barriers has been proposed. None of these adjuncts has demonstrated an improvement in fertility and pregnancy outcomes
- 56. Uterine Artery Embolization Carried out by interventional radiologists and consists of injecting an occluding agent into one or both uterine arteries Most common alternative offered to women with sympotomatic uterine fibroids Very large uteri (over 20 weeks) may not have a clinically significant response Single submucosal fibroids or subserosal fibroids may respond better to surgery than UAE Post Embolization syndrome : Pain, Fever, Expulsion Pregnancy rates were lower and miscarriage rates higher following UAE Best reserved for women who do not desire future pregnancy
- 57. UAE v/s Myomectomy RCT for UAE versus myomectomy : comparable symptom improvement and improved QoL. The re-intervention rate is > for UAE.
- 58. Focused Energy Delivery Systems A number of focused energy delivery systems have been tested in the past decade including those based upon radiofrequency electricity, supercooled cryoprobes, and most recently, MRg-FUS or high frequency ultrasound guided transcutaneous focused ultrasound ablation A major disadvantage of all systems and techniques used to desiccate or ablate fibroids may be that they treat one fibroid at a time and they target the centre of fibroids, while fibroids have been shown to grow mostly from their periphery These technologies are relatively new and although many are promising, they often lack long-term data, which interferes with our ability to present all risks and benefits with assurance. Ongoing research and data collection are required to assess the relative merit of newer options as the technology continues to expand
- 59. MR-guided focused ultrasound Shortterm efficacy is adequate Skin burns have occurred in up to 7% of patients and at least one bowel perforation was reported Disadvantages of the MRg-FUS system include high exclusion rate, requirement of an MR machine, prolonged time (minutes to several hours), treatment of 1 fibroid at a time, and ablation of fibroids centrally, while fibroids seem to grow peripherally
- 60. Radiofrequency myolysis Delivering of RF energy to myomas under ultrasonic guidance in an attempt to dessicate them directly well tolerated and results in rapid recovery, high patient satisfaction, improved quality of life, and effective symptom relief Total mean fibroid volume was reduced by 45.1% and mean blood loss by 38.3% at 12 months post-procedure. Disadvantages include the requirement of laparoscopy and concomitant use of ultrasound, additional percutaneous skin incision(s), its treatment of 1 fibroid at a time (< 8 cm diameter), and its ablation of fibroids centrally while fibroids grow peripherally
- 63. No Hysteroscopic Acess, No Gestational Desire
- 64. No hysteroscopic access, Desire future fertility
- 65. Cervical Fibroid Lantern on St Paul’s Cathedral
- 66. Cervical Fibroid The paucity of smooth muscles in the cervical stroma makes leiomyomas in the cervix uncommon The incidence of cervical fibroids is around 0.5% – 2% Depending on the position, cervical fibroids can be anterior, posterior, lateral or central Symptoms are mainly due to pressure effects on the bladder leading to acute urinary retention and increased frequency of micturition, the pressure effect on the rectum can cause constipation
- 67. Surgery for cervical fibroid In case of hysterectomy, the principal to be followed is enucleation followed by hysterectomy to minimize injury to ureter and also uretric stenting can be done prior to surgery. Enucleation in case of central cervical fibroid, The problems anticipated during hysterectomy for large cervical fibroid are due to distortion of normal anatomy of ureter and uterine vessels and sometimes due to pulled up bladder anteriorly. Therefore, there are more chances of injury to ureter, bladder and uterine vessels.5,6 Intracapsular enucleation of fibroid is the best approach to prevent injury to bladder and ureters
- 68. In my early years as a gynaecological surgeon, a case occurred which profoundly affected my outlook. A lady, recently married, wishing above all things to have a child underwent a subtotal hysterectomy on account of a single submucous fibroid. Being a woman of strong character and reticent fortitude, she accepted the blow without complaint and by assuming a proud indifference to children, held her insistent mother instinct at bay and none but those who knew her well perceived the tragedy. I was among this number and the grief of it is still keen in me today
Editor's Notes
- Translocations between 12 &14, deletions and rearrangements of chromosome 6 / 7 : Cellular, large and large Epidermal growth factor (EGF), insulin-like growth factor-1 (IGF-1), transforming growth factor (TGF),
- limited to reproductive life.. Increased growth during pregnancy.. They do not occur before menarche.. Following menopause, there is cessation of growth.. GnRH : Reduction in size. When P is given with GnRH, No reduction OCP’s HRT : More to do with progesterone than estrogen Increases during pregnancy but lower in multipara’s
- Obesity : SHBG Falls, increased conversion of adrenal androgens to estrone