Downloaded 37 times
![Letters to patients: a survey
If the doctor I see in clinic writes to me rather than to my GP:
[strongly agree, agree, neither agree nor disagree, disagree, strongly disagree]
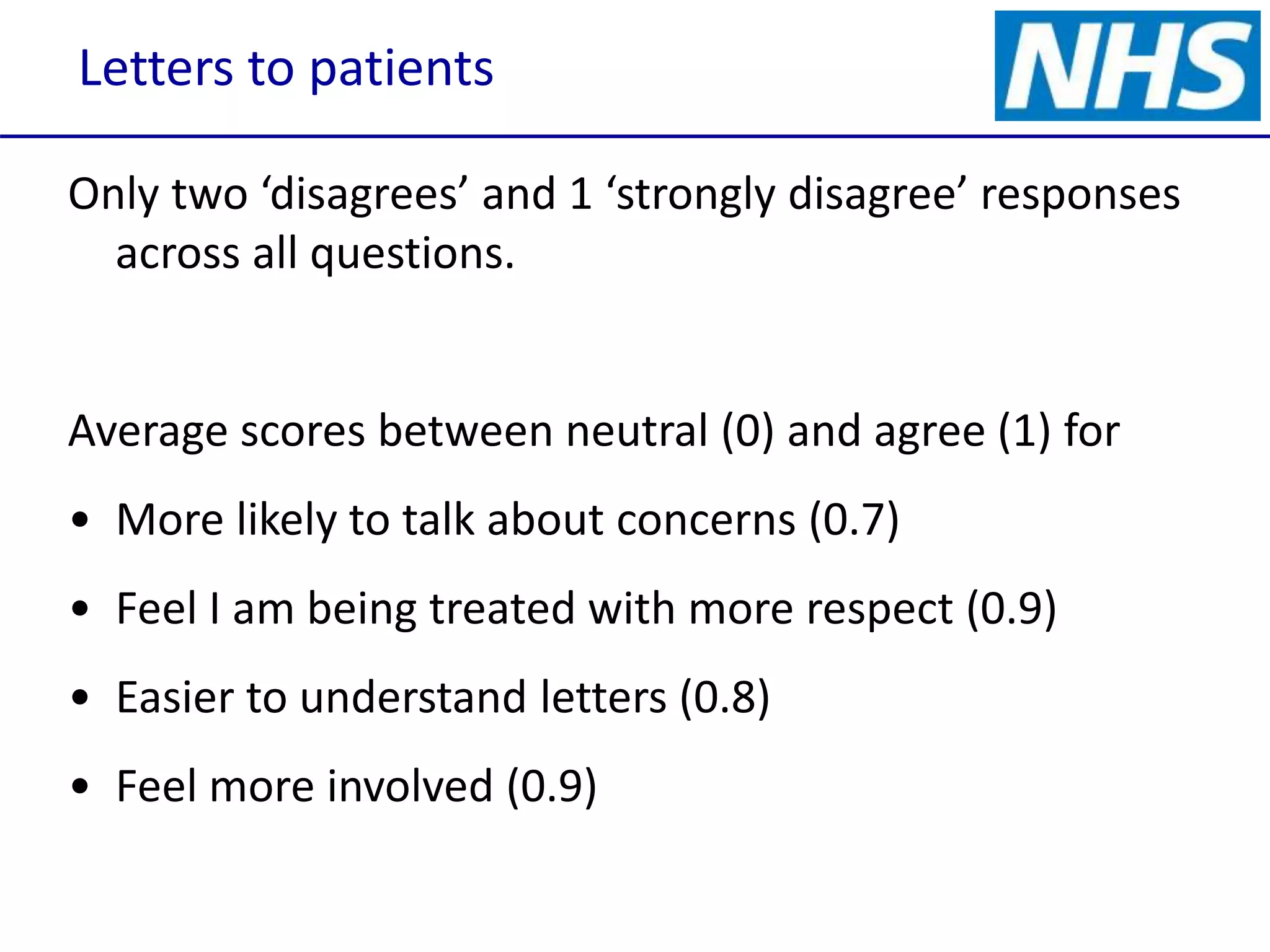
• I am more likely to talk about concerns I have when I next come
to clinic.
• I am more likely to make an appointment with the GP if my
medication needs changing.
• I feel that I am being treated with more respect.
• The letter to me is easier to understand than letters sent to my
GP.
• I feel more involved in my care.](https://image.slidesharecdn.com/eliaswritingletterstopatients151008forsharing-151009100401-lva1-app6892/75/Writing-letters-to-patients-and-copying-GP-in-4-2048.jpg)
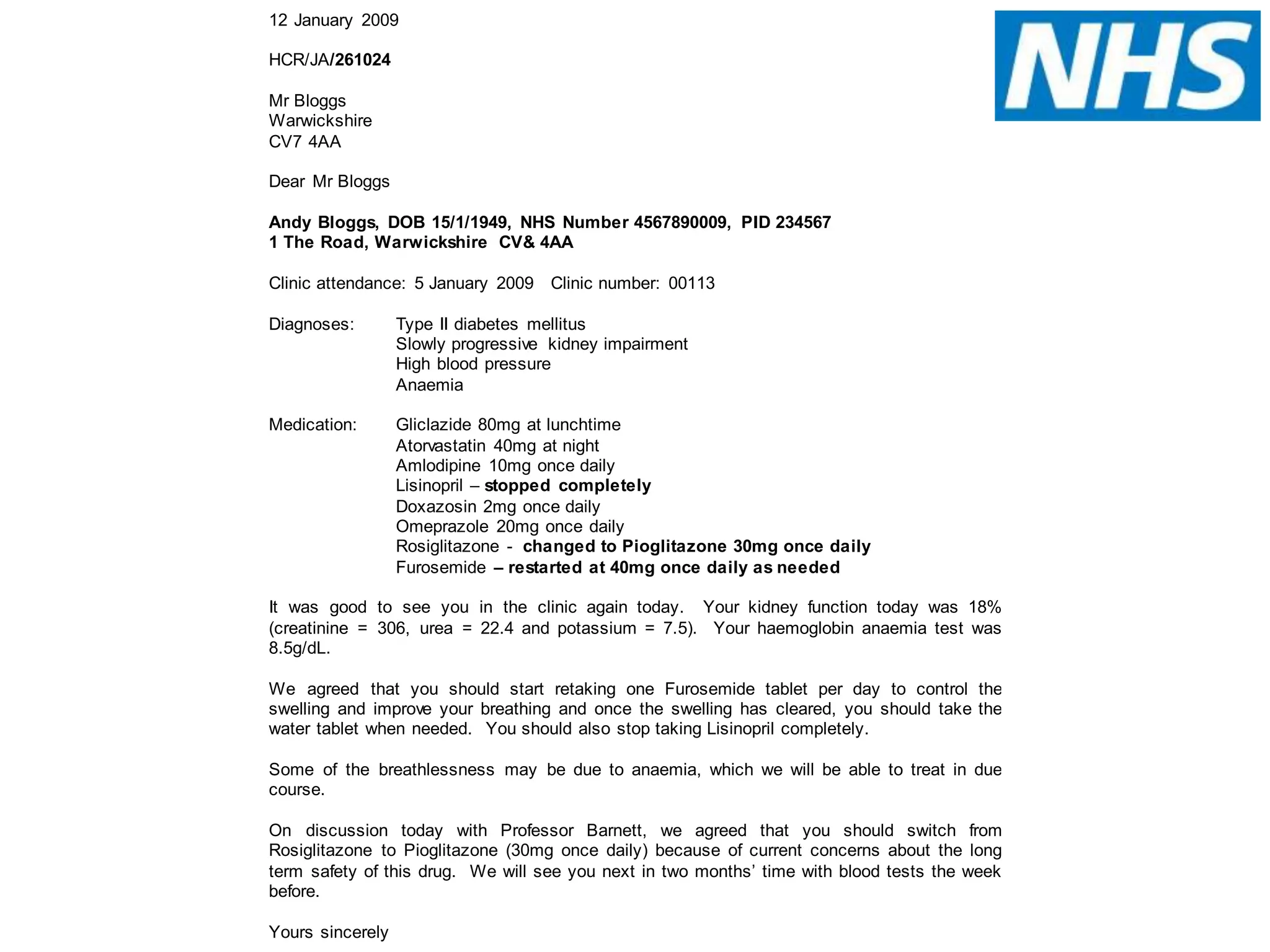
![Problem List
Acute kidney injury and hypertension 2013
Crescentic IgA nephropathy on kidney biopsy 2013
Current Medications
Frusemide Tablets 40mg PO once a day
Ramipril Tablets 5mg PO once a day* [02/10/15]
Ranitidine Tabs/Inj 150mg PO twice a day
* added or dose changed within last 14 days
ALLERGIES/INTOLERANCE: none known
BP: 104/72 Weight: 72.2 kg Urine Blood: trace Urine Protein: neg
It was a pleasure to see you in clinic today. I'm pleased to hear that you have no problems to report since we last saw
you.
You have no ankle swelling. Your weight is up a little. Kidney function on the blood tests is stable.
Although today’s urine dip is negative for protein, the measured protein level in the urine is still high (PCR 90). This has
steadily improved over the last year. The introduction of the ramipril tablet last time will have helped with that.
We talked about how best to control blood pressure and protein leak. You have had some dizzy spells which has meant
that you have not increased the ramipril beyond 5mg. I suggest you stick with things as they are at the moment, and
when I next see you we can consider stopping the frusemide with a view to increasing the ramipril.
We will see you again in 3 months.
Best wishes,](https://image.slidesharecdn.com/eliaswritingletterstopatients151008forsharing-151009100401-lva1-app6892/75/Writing-letters-to-patients-and-copying-GP-in-12-2048.jpg)

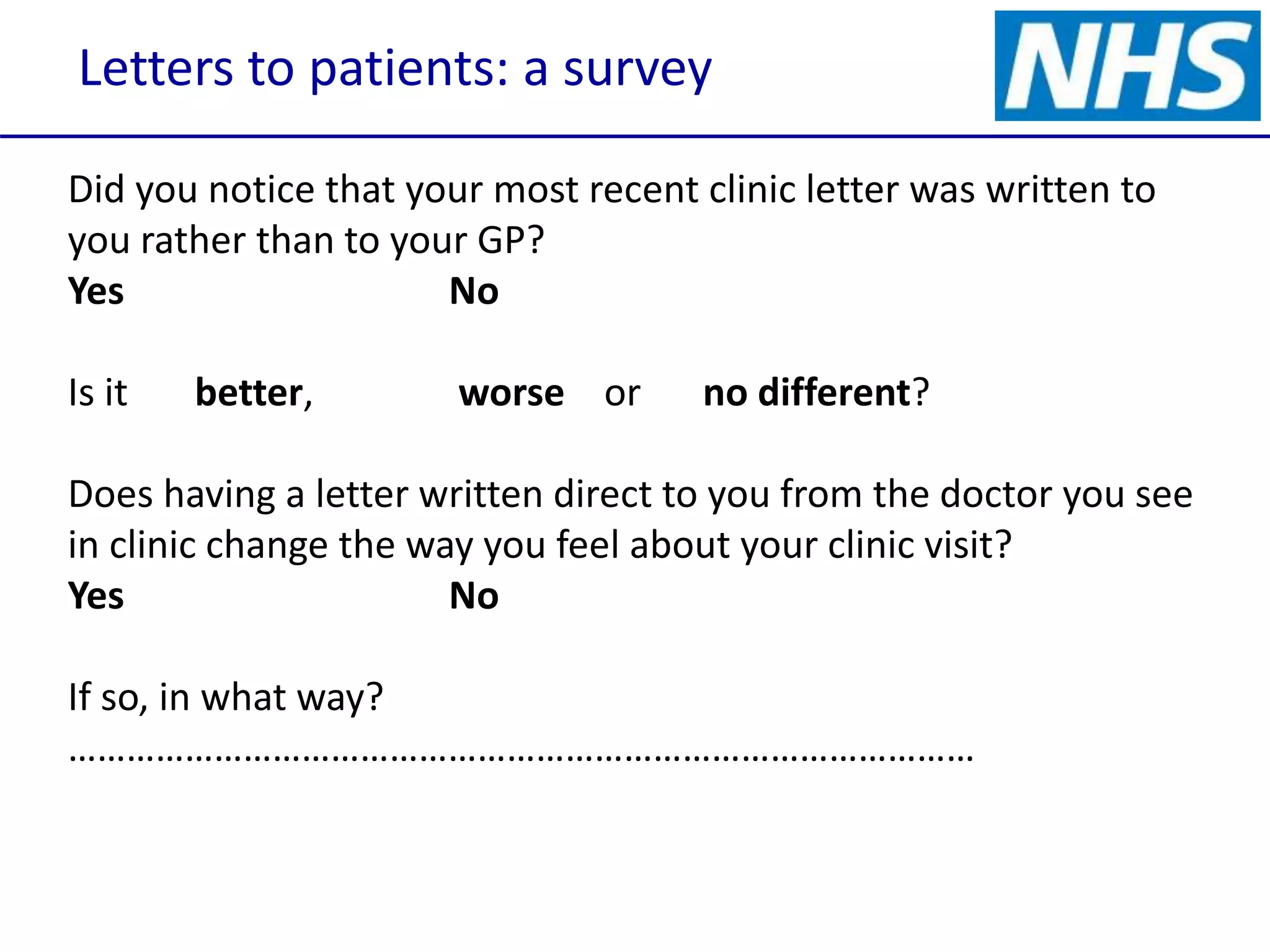
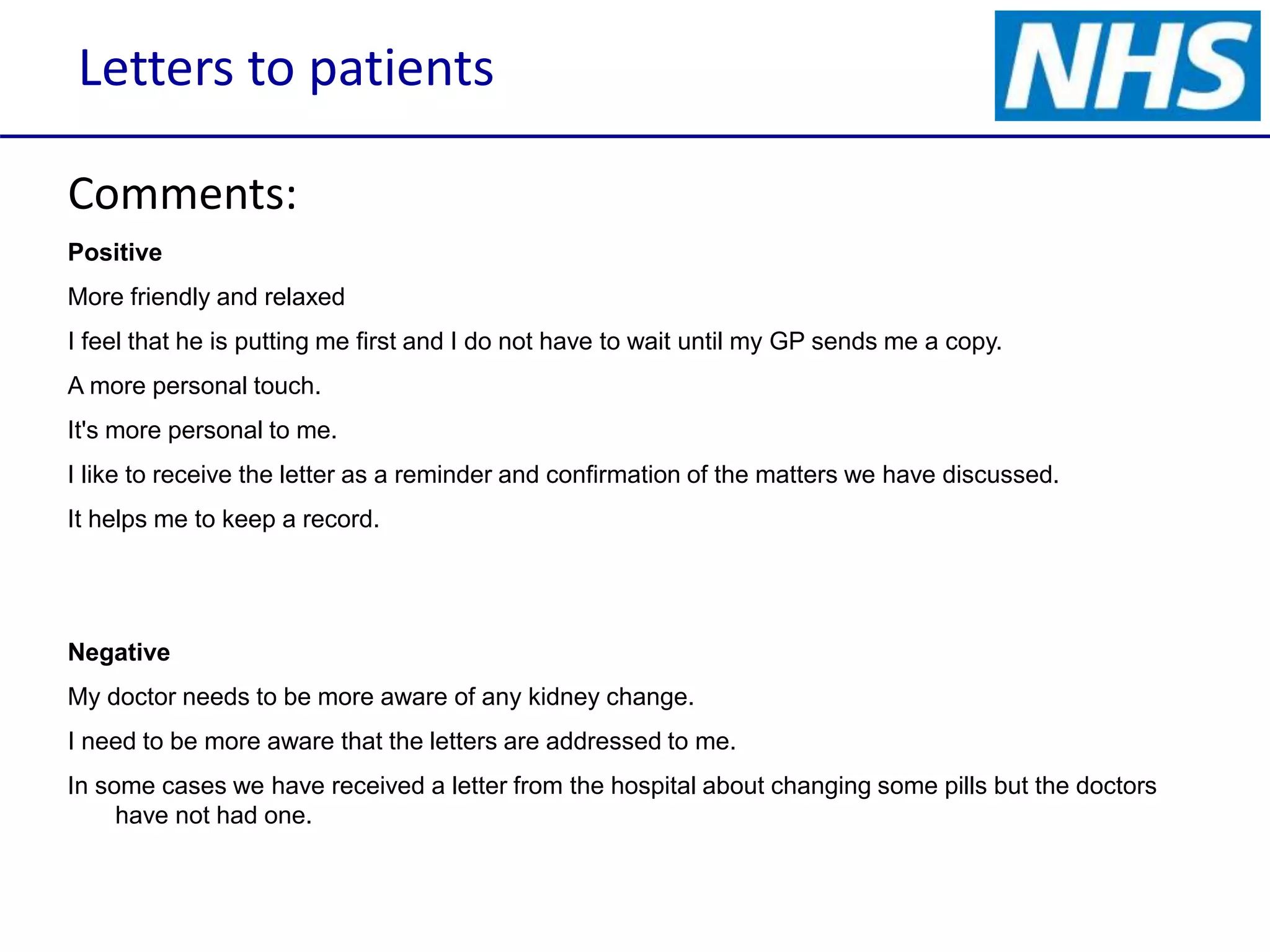
A survey conducted among kidney clinic patients revealed that letters addressed directly to them improved their understanding and involvement in their care. Most patients felt respected and were more likely to discuss concerns or make GP appointments when receiving letters directly from their doctor, with a high level of agreement on the effectiveness of this communication method. Overall, the practice of writing to patients is viewed positively, with suggestions for simplifying language and formatting in future correspondence.















































