Sphincter tone/cranial nerve function is typically intact, respiratory muscle weakness is rare
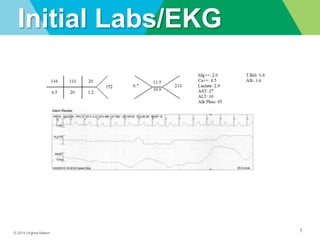
Tall peaked T waves w/ shortened QT interval, lengthening of PR interval and QRS, P waves disappears and ultimately QRS becomes sine wave
Porgression of EKG changes do not correlate well with serum potassium concentration. Review of 90 pt with hyperK found that EKG abnormalities increased with increasing serum potassium, but EKG was insensitive for diagnosis of hyperK. 46% had changes with hyperK
Peaked T waves not specific, but also seen in early phase of acute MI, early repolarization, LVH
Sphincter tone/cranial nerve function is typically intact, respiratory muscle weakness is rare
Tall peaked T waves w/ shortened QT interval, lengthening of PR interval and QRS, P waves disappears and ultimately QRS becomes sine wave
Porgression of EKG changes do not correlate well with serum potassium concentration. Review of 90 pt with hyperK found that EKG abnormalities increased with increasing serum potassium, but EKG was insensitive for diagnosis of hyperK. 46% had changes with hyperK
Peaked T waves not specific, but also seen in early phase of acute MI, early repolarization, LVH
Sphincter tone/cranial nerve function is typically intact, respiratory muscle weakness is rare
Tall peaked T waves w/ shortened QT interval, lengthening of PR interval and QRS, P waves disappears and ultimately QRS becomes sine wave
Porgression of EKG changes do not correlate well with serum potassium concentration. Review of 90 pt with hyperK found that EKG abnormalities increased with increasing serum potassium, but EKG was insensitive for diagnosis of hyperK. 46% had changes with hyperK
Peaked T waves not specific, but also seen in early phase of acute MI, early repolarization, LVH
CaGluconate for stabilizing myocardial conduction system
Due to its potential for adverse effects and minimal effect on potassium levels (decreases potassium by about 1 mEq/L over 24 hours), some authors have questioned the use of sodium polystyrene sulfonate.
Common wasters include diuretics, but also mineralcorticoids, glucocorticoids (31% of hospitalized pt with severe hypokalemia caused by corticosteroids), high dose penicillins. Then also mag wasters include foscarnet, cisplatin, aminoglycosides.
Colonoscopy prep causes hypok in 56-58% of pts.
Trousseau's sign depends upon the effect of ischemia to increase excitability of the nerve trunk under the cuff, rather than at the motor endplate; excitability is maximal at three minutes and returns to normal even if ischemia is maintained for a longer period.
Jesus, J.E and Landry, A. Chvostek’s and Trousseau’s Signs. N Engl J Med 2012, 367:e15 DOI 10.1056/NEJMicm1110569