
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Breast cancer handout
Similar to Breast cancer handout (20)
Recently uploaded
Recently uploaded (20)
Breast cancer handout
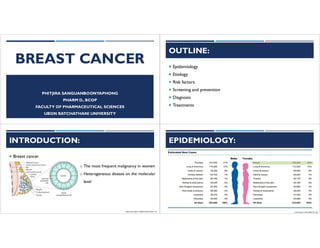
- 1. BREAST CANCER PHITJIRA SANGUANBOONYAPHONG PHARM D., BCOP FACULTY OF PHARMACEUTICAL SCIENCES UBON RATCHATHANI UNIVERSITY OUTLINE: ¡ Epidemiology ¡ Etiology ¡ Risk factors ¡ Screening and prevention ¡ Diagnosis ¡ Treatments INTRODUCTION: ¡ Breast cancer o The most frequent malignancy in women o Heterogeneous disease on the molecular level https://doi.org/10.1038/s41572-019-0111-2 EPIDEMIOLOGY: CA Cancer J Clin 2020;70:7-30.
- 2. EPIDEMIOLOGY: CA Cancer J Clin 2020;70:7-30. EPIDEMIOLOGY: ทะเบียนมะเร็งระดับโรงพยาบาล สถาบันมะเร็งแห่งชาติ พ.ศ.2562 ETIOLOGY: ¡ Unknown etiology ¡ Genetics: represent 5-10% of all breast cancer ¡ Tumor suppressor gene o BRCA 1, BRCA 2 o p53 ¡ Progression gene o HER2 (Human Epidermal Growth Factor Receptor-2, erbB-2) ETIOLOGY: ¡ BRCA1 and BRCA2 o Tumor suppressor gene o Relative rare in general population (1:300 for BRCA1 and 1:800 for BRCA2) o Probability for breast and ovarian CA by 70 yr o BRCA 1 : 57% (breast) and 40% (ovary) o BRCA 2 : 49% (breast) and 18% (ovary) o Non carrier have cancer risk as normal population o Individual likely to get benefit for testing male related
- 3. ETIOLOGY: ¡ Characteristics Associated with an Increased Likelihood of BRCA1 and BRCA2 Mutations Personal History Family History Breast cancer at an early age (≤ 45 years) 2 first degree relatives with diagnosis, at least 1 diagnose at ≤ 50 years Bilateral breast cancer at age ≤ 50 years A first- or second-degree relative with cancer at age 45 y or younger Triple-negative breast cancer at age ≤ 60 years Others cancer associated with BRCA mutation ETIOLOGY: ¡ P53 o Tumor suppressor gene o 20% of breast cancer have mutation, inactivation, loss or down- regulated expression of p53 o Associated with Li-Fraumeni syndrome q < 1% associated of breast cancer associated with this syndrome ETIOLOGY: ¡ HER2 (Human Epidermal Growth Factor Receptor-2, erbB-2) o Proto-oncogene o Amplified/overexpressed in approximately 20-25% of all breast cancers o Impart poorer prognosis o HER2 status should be determined on every primary invasive breast cancer ETIOLOGY: ¡ HER2 (Human Epidermal Growth Factor Receptor-2, erbB-2) Nat. Rev. Clin. Oncol. 2012; 9:16–32. Ionis Tou growthead bindt med anti here a dimerization proteinkinase s iuncancer
- 4. RISK FACTORS: ¡ Gender (Female) o Male breast cancer can occur approx. 1% (associated with BRCA-2) ¡ Age o ≥ 50YO increase risk by 6.7 times ¡ Familial o 1st degree relatives with breast cancer portends a 2-fold higher risk o The risk can increase 3- to 4-fold if a 1st degree relative was diagnosed at an age < 50Y ¡ Benign breast disease ¡ Early thoracic irradiation encompassing the chest/breast area before age 30 RISK FACTORS: ¡ Endogenous estrogen exposure o Early age of menarche (typically defined as ≤ 12 y/o) o Late age of natural menopause (typically defined as ≥ 55 y/o) o Early induced menopause (bilateral salpingo-oophorectomy or BSO) before 50 y/o decreases risk, with further risk reduction as the age of BSO decreases o Age at birth of first child ≥ 30 y/o or nulliparity ¡ Exogenous estrogen exposure o Oral contraceptive is non-significant increase risk when compared to who had never used OC o Longer duration use of hormone replacement therapy increase risk RISK FACTORS: ¡ Obesity o Postmenopausal; higher weight increase risk ¡ Breast density ¡ Physical inactivity ¡ High fat diet ¡ Alcohol consumption SCREENING AND PREVENTION: ¡ Risk estimation o Gail model risk assessment toolà to determine RR to develop breast cancer at 5 years or during lifetime q Risk reduction (prevention) requirement when 5-yr RR ≥ 1.66&% q Factors included • Age • No of 1st degree relatives with invasive breast cancer • Nulliparity or age at first birth • No of previous benign breast biopsies • Atypical hyperplasia in a previous breast biopsy • Race important male A menu Testroyent 1 marri wine esp xsure exgermaelitumor ix award landmine screen iwhen madmen iu HushInext in percent it 1 other uprevent yearn xchiidlssyearhaueitb.by
- 5. SCREENING AND PREVENTION: ¡ Screening methods for early detection 1. Breast self examination (BSE) o Perform monthly; week after menses 2. Clinical breast examination (CBE) 3. Mammography o Report result as BI-RADS (0-6) 4. Breast MRI o Adjunct to mammography Health Care Women Int. 2003; 24: 773-793. SCREENING AND PREVENTION:: ¡ Screening recommendation SCREENING AND PREVENTION: ¡ Screening recommendation ¡ High risk group defined as o Prior thoracic RT between the ages of 10 – 30 y o Women ≥ 35 y with 5-year Gail model risk of invasive breast cancer ≥ 1.7% o Known genetic predisposition o Women with a history of LCIS and a >20% lifetime risk o Prior history of breast cancer SCREENING AND PREVENTION: ¡ Prevention recommended for o High risk group (in the previous slide) o Patient preference for risk reduction therapy ¡ Prevention method o Bilateral total mastectomy ± reconstruction o Bilateral salpingo-oophorectomy (BSO) o Agents for risk reduction: q Premenopausal – tamoxifen or clinical trial q Postmenopausal – tamoxifen, raloxifene,AI, or clinical trial NCCN. Breast cancer risk reduction. V1.2020 odium nom group highriskampi now nonmainw in specalista cut.ae adiuctexroutine am i f oumna.aetamib v e naman s tamibhx maruti 4 ornaimonium s any
- 6. PATHOLOGY: ¡ Histology subtypes Nature Reviews Disease Primers. 2019; 5(66): 1-31. DIAGNOSIS: ¡ Determination of the ER, PR and HER2 status is mandatory for all patients with invasive breast cancer ¡ Hormonal status (ER/PR) o Testing by immunohistochemistry o Considered ER/PR positive when nuclear staining > 1% of invasive tumor cells ¡ Ki-67 o Used to determine proliferation and predicts chemosensitivity o Relevant for luminal type breast cancer (HR positive, Her-2 negative) o Cut off value ≥ 20% classified as high level Nature Reviews Disease Primers. 2019; 5(66): 1-31. DIAGNOSIS: ¡ HER2 (Human Epidermal Growth Factor Receptor-2, erbB-2) o Simplified HER2Testing Algorithm for Breast Cancer Arch Pathol Lab Med. 2018;142:1364–1382 ASCO/CAP suggested o Positive result : IHC 3+ or 2+ with positive FISH INTRINSIC SUBTYPES OF BREAST CANCER: Subtypes ER PR HER-2 Ki-67 Luminal A + ≥20% - Low (< 20%) Luminal B qHER-2 negative qHER-2 positive + + - - - - High (≥20%) Any HER-2 Overexpression - - + Any Triple negative breast (Basal type) - - - Any Annals of Oncology. 2013; 24: 2206–2223. no pinpreventionr armor 2 endocrine tx mo io.in 3 howtast nonaggressive poor prognosis disease anion 4 erimpositive fuendocrinet prognosis inigh erpositive 3erepositive positives chemotherapy base sina.am sure ion immunohistochemistry
- 7. BREAST CANCER AND HISTOLOGIC MOLECULAR SUBTYPE: STAGING: STAGING: STAGING: Inoperable disease e ve o a a want en n w wi ma o n b oink v ne o a di want first systemic tx
- 8. MANAGEMENT OF BREAST CANCER: ¡ Treatment modalities divided into 3 modalities qSurgery qRadiation qPharmacologic treatments o Chemotherapy o Endocrine therapy à HR positive o Anti-HER2 à HER-2 positive o CDK4/6 inhibitors o mTOR inhibitor MANAGEMENT OF BREAST CANCER: ¡ Surgery o 2 main types of surgery to remove breast cancer qBreast conservative surgery (BCS) aka Lumpectomy qMastectomy o 2 types of surgery to remove nearby lymph node qSentinel LN biopsy qAxillary LN biopsy American cancer society latest update 2019 MANAGEMENT OF BREAST CANCER: ¡ Surgery o Mastectomy with axillary LN dissection (ALND) o BCS + ALND + whole breast RT qMeta-analysis of XRT vs. no XRT after BCS showed • Reduction in the 10-year risk of first recurrence by 15.7% (95%CI 13.7-17.7, p<0.00001) • Reduction 5-year risk of breast cancer death by 3.8% (95%CI 1.6-6.0, 2p<0.00005) o Benefit in q All Ductal carcinoma in situ (DCIS) q Invasive breast cancer (all stage I, II, IIIA and resectable IIIB or IIIC) American cancer society latest update 2019 Lancet 2011; 378: 1707–16 MANAGEMENT OF BREAST CANCER: ¡ Radiation required in o All BCS (recommended) o ALN positive ≥ 4 (recommended), 1-3 LV (Considered) o ALN negative • T > 5 cm • Positive margin • T ≤ 5 cm with closely margin (< 1 mm) Emma qithtriple negative breast mono so should cuz betterX margin positive 2 i amastectomy with node positive zanode for no local control rimonoina vbenitit a size it a a margin Hormonal status what ismargin 5 I Imodonoton n c ww mastectomy andbetter
- 9. MANAGEMENT OF BREAST CANCER: ¡ Chemotherapy Recommended in ¡ Stage I-IIIA (as adjuvant tx) o All lymph node positive o LN (-) q ER (+) • Tumor size 0.6-1 cm à Consider in high risk group • Tumor size > 1 cm à all patients q ER (-) • Tumor size 0.6-1 cm à Consider in high risk group • Tumor size ≥ 1 cm à all patients o All HER-2 (+) High risk group o Histology grade 3 o Triple negative o LVI positive o Oncotype DX Recurrence score ≥ 31 points o HER2-positive MANAGEMENT OF BREAST CANCER: ¡ Chemotherapy Recommended in o Stage IIIB-IIIC (Neoadjuvant therapy) o Stage IV o All triple negative breast cancer EARLYTO LOCALLY ADVANCED BREAST CANCER MANAGEMENT (STAGE I-III) NCCNV1.2021 Early breast cancer ER negative HER-2 positive Node (+) or Node (-) with T>1cm Adj.CMT+ Trastuzumab HER-2 negative Node (+) or Node (-) with T>1cm Adj. CMT ER positive HER-2 negative Node (+) Adj. CMT followed by adj. ET Node (-) T ≤ 0.5 cm Adj. ET T >0.5 cm Oncotype Dx RS ≥ 31 Adj. CMT followed by adj. ET RS < 31 Adj. ET HER-2 Positive Node (+) or Node (-) with T>1cm Adj.CMT+ Trastuzumab followed by adj. ET CMT = Chemotherapy ET = Endocrine therapy Adj.=Adjuvant treatment mi 7 eaten makens.metas info'iascularinvasive m m f umnumb iertirst ruminatype ai Heroverexpression tripieneg ruminal neg Kiaoi rumina Her neg n'I with win chemotaxrole e g't ABC antiereumono endocrine no endocrine the act aimonem a only 1oz aweekaweer static better recurrener I t.cnoieswa
- 10. AFTER PREOPERATIVETREATMENT: CONVENTIONAL CMT ¡ Regimen for adjuvant can use for neoadjuvant ¡ Preferred regimen for HER-2 negative CONVENTIONAL CMT ¡ Regimen for adjuvant can use for neoadjuvant ¡ Preferred regimen for HER-2 positive Paclitaxel + trastuzumab may be considered for patients with low-risk T1,N0,M0, HER2-positive disease, particularly those not eligible for other standard adjuvant regimens due to comorbidities PHASE III ECOG 1199:ADJUVANT PACLITAXEL VS DOCETAXEL, BOTH Q3W AND QW, IN EBC ns.wim nistagesbisc ana Doxorubicin no.to.no m but a o base anti nerdy g aweek antacy learn.no waitin acbase www.dbyictaxa me n.n.ema.y.ne.a.aymq.ae a capecitabine nterceptina n.nswe.ieiwee ner.ptin i ras u.umab pantinter acbased week better e negativeacbase Doxorubicin nonabase cyclophosphamide acardiotoxict cyclophosphamide tonowbst to premen tamoxifen pacitexact oocetexeiiwr.azX.imini taxa ERpositive r positive pacitexel to acetexel to acetexel a postmen AIs if cats carboplatin carboplatin endocrine tx trastuzumab trastuzumab trastummabtpertummab www.iskoniyitono
- 11. PHASE III ECOG 1199:ADJUVANT PACLITAXEL VS DOCETAXEL, BOTH Q3W AND QW, IN EBC Sparano J, et al. N Engl J Med. 2008;358:1663-1671. PHASE IIITRIAL COMPARING ACWITHTC AS ADJUVANTTHERAPY FOR OPERABLE BREAST CANCER J Clin Oncol.2006; 24:5381-5387. J Clin Oncol. 2009; 27:1177-1183 The primary end point of this trial was the overall DFS. The secondary endpoint was the overall survival. TCVSTAXAC IN HER2- BREAST CANCER (ABC JOINT ANALYSIS): J Clin Oncol. 2017; 35:2647-2655. ADJUVANT ANTI-HER 2: ¡ N9831/NSABP B-31 Joint Analysis:AC-TH vs ACT J Clin Oncol.2011; 29:3366-3373 y basedmore.ardiotoxic cardio toxicity weekly better betterardiotoxict kneneptinw.in bettersbasedn.on it actouwedby xoii.nu
- 12. BCIRG 006:AC-TVSTCH OR AC-TH: Slamon D, et al. N Engl J Med. 2011;365:1273-1283. Slamon D, et al. SABCS 2015. Abstract S5-04. BCIRG 006: DFS AND SAFETY Slamon D, et al. N Engl J Med. 2011;365:1273-1283. PHASE III APHINITY: DUAL HER2TARGETING IN ADJUVANTTHERAPY OF EBC: N Engl J Med 2017;377:122-31. PHASE III APHINITY: DUAL HER2TARGETING IN ADJUVANTTHERAPY OF EBC: N Engl J Med 2017;377:122-31. Anthracycline rubicin eiection traction act not more xiouan inerotore Tat oinkwnecardiotoxict trastuzumabi.nu dimerize Her.nu Her pertuzumabir dimerize Henarwaer better
- 13. KATHERINE:TRASTUZUMAB EMTANSINEVS TRASTUZUMAB AS ADJUVANTTHERAPY FOR HER2+ EBC NEJM. 2019;380:617. KATHERINE: DFS NEJM. 2019;380:617. ANTI-HER-2: ANTI-HER-2: Name FDA approved indication Mechanism of action Dose range Toxicities Trastuzumab Humanized monoclonal antibody HER2 (+) breast cancer (adjuvant, metastatic) o extracellular domain IV of HER2 o 4 mg/kg LD, then 2 mg/kg weekly o 8 mg/kg LD, then 6 mg/kg every 3 weeks o Black box warning: cardiotoxicity: avoid concurrent with anthracyclines o infusion reactions o embryo-fetal toxicity o pulmonary toxicity (pneumonitis) Pertuzumab o extracellular domain II of HER2 o Block heterodimerization with HER 1, 3, 4 o 840 mg LD then 420 mg q3 weeks o Cardiotoxicity (1.2%) o Hand-foot syndrome o Infusion reactions Trastuzumab emtansine (TDM-1) Antibody drug conjugate HER2 (+) breast cancer o HER2 block o Inhibit microtubule polymerization o 3.6 mg/kg q 3 weeks o Not interchangeable with trastuzumab o Cardiotoxicity o Hepatotoxicity o Pulmonary toxicities o Peripheral neuropathy Cancer Pharmacology and Pharmacotherapy Review. 2016 i 31313C 2Herat 3 Malvo 3 aimag change to T Dn Fo SB sa a positive change too betteranninia a same immune
- 14. ANTI-HER-2: Future oncol. 2017; 14(7): 1-14. CHEMOTHERAPY RELATED CARDIAC DYSFUNCTION: Shakir DK, et al. J Clin Med Res. 2009;1:8. Type I Type II Characteristic Cellular death Damage starts with 1st dose Cellular dysfunction Pathology Biopsy changes No typical biopsy changes Cumulative dose Related Not related Reversible Permanent Reversible Anticancer agents involved Anthracyclines Trastuzumab, lapatinib CHEMOTHERAPY RELATED CARDIAC DYSFUNCTION: Treatment factors o Type of drug o Dose of each cycle o Cumulative dose o Schedule of administration o Route of administration o Combination with other cardiotoxic- drug or radiation Patient factors o Age o Presence of cardiovascular risk factor o Previous cardiovascular disease o Prior mediastinal radiotherapy Ann Oncol. 2010;21 Suppl 5:v277. J Clin Oncol.2016; 35:893-911. ASCO RECOMMENDATION: ¡ For patients who undergo with anthracycline o Evaluation cardiac function at baseline by ECHO or MUGA scanning o For patients with a LVEF >50% at baseline: q Consider repeating after reaching 250-300 mg/m2 q Repeat after reaching 400 mg/m2 in patients with known risk factors of cardiac failure or after 450 mg/m2 in the absence of risk factors q Discontinue doxorubicin if: ØFunctional signs of cardiotoxicity and/or ØAbsolute decrease in LVEF ≥ 10% associated with a decline to a level of < 50%. typeotardiotoxicity Ac trastuzumab irrevesible unemotx anti microtubules myocyte dead n.com www.w. risktaotmadeveiopcardiotoxic starter then recheck my cumulative dose or w mgacoot
- 15. ASCO RECOMMENDATION: ¡ For patients who undergo with trastuzumab o Assess LVEF prior to initiation, every 3 months and every 6 months for at least 2 years following completion of adjuvant Trastuzumab o Withhold trastuzumab for at least 4 weeks for any of the following q ≥ 16 absolute decrease in LVEF from baseline q LVEF below institutional limit of normal and ≥ 10 absolute decrease from baseline o Resume if LVEF returns to normal limits and absolute decrease from baseline is ≤ 15 (within 4 –8 weeks) o Permanently discontinue if persistent (> 8 weeks) LVEF decline or if suspended ≥ 3 occasions for cardiomyopathy ADJUVANT ENDOCRINETHERAPY: N Engl J Med.2001; 344(4):276-285. ENDOCRINETHERAPY: ¡ Selective Estrogen Receptor Modulators (SERMs) ¡ Aromatase Inhibitors (AI) ¡ Selective Estrogen Receptor Downregulators (SERDs) ¡ Ovarian ablation for premenopausal status o LHRH agonist/antagonist o Surgery Nat Rev Cancer. 2003;3:821–831. SELECTIVE ESTROGEN RECEPTOR MODULATORS (SERMS) ¡ Tamoxifen ¡ MOA: o Selectively stimulate or inhibit the estrogen receptors of different target tissues o Inhibit the estrogen receptor found in breast cells o Activate the estrogen receptor present in uterine endometrial cells ¡ Usual dose 20 mg/day Clinical Interventions in Aging 2014:9 1437–1452 estrogen trisk a woman then every then.mg at iia iiion baselinehold Hua a week back to baselinerestrat but ii persist a minnow weeks A stroke metastatis stage w.io induce on ma post mention chance endometrial cancer
- 16. META-ANALYSIS OFTAMOXIFEN ALONE IN PREMENOPAUSAL WOMEN EBCTCG, et al. Lancet. 2011;378:771-784. 13.2% 9.2% META-ANALYSIS OFTAMOXIFEN ALONE IN PREMENOPAUSAL WOMEN EBCTCG, et al. Lancet. 2011;378:771-784. § Tamoxifen side effect o Hot flashes o Vaginal discharge, sexual dysfunction o Menstrual irregularity o Significantly increased risk ofVTE o Non significant increased risk of strokes o Increased the risk of uterine cancer o Limited to women over 55 years SELECTIVE ESTROGEN RECEPTOR MODULATORS (SERMS) s t e r o i d s 7 2 ( 2 0 0 7 ) 829–842 J Clin Oncol 2010;28:3784 J Clin Oncol. 2019; 37:636-646. ¡ Tamoxifen o Prodrug o Metabolized through multiple enzymes to be more active compound (Endoxifen and 4- hydroxytamoxifen) q CYP2D6 is considered the rate-limiting enzyme o ASCO recommendation o Drug-drug interaction between tamoxifen and CYP2D6 inhibitors should be avoid SELECTIVE ESTROGEN RECEPTOR MODULATORS (SERMS) s t e r o i d s 7 2 ( 2 0 0 7 ) 829–842 J Clin Oncol 2010;28:3784 J Clin Oncol. 2019; 37:636-646. ¡ CYP 2D6 and tamoxifen ¡ Strong to moderate inhibitors should be avoided during tamoxifen ¡ Agents can be use o citalopram, escitalopram, and venlafaxine trecurrence.lu mortality sigwhen thromboembolisms age so year 2 sigin
- 17. AROMATASE INHIBITORS: § Letrozole (Femara®) 2.5 mg/day § Anastrozole (Arimidex®) 1 mg/day § Exemestane (Aromasin®) 25 mg/day § Blocks estrogen production from other tissue § Recommended in postmenopausal patients AROMATASE INHIBITORS: ¡ Menopause definition o Prior bilateral oophorectomy o Age ≥60 y o Age <60 y and amenorrheic for 12 or more months in the absence of chemotherapy, tamoxifen, toremifene, or ovarian suppression and follicle-stimulating hormone (FSH) and estradiol in the postmenopausal range o If taking tamoxifen or toremifene, and age <60 y, then FSH and plasma estradiol level in postmenopausal ranges NCCN V1.2021. ADJUVANT HORMONALTRIAL DESIGN: ¡ Direct comparison; o Supporting trial;ATAC, BIG1-98,TEAM ¡ Switching o Supporting trial; IES,ARNO/ABCSG combined analysis ¡ Sequencing o Supporting trial;ABCSG 8 alone (arms A & C), BIG 1-98 sequencing arms (C&D) ¡ Extended adjuvant o Supporting trial; MA-17R, NSABPB-33,ABCSG-6a ADJUVANT HORMONALTRIAL DESIGN: J Clin Oncol. 2010; 28:3784-3796 Pre men tamoxifen FRpositive postmen aIs estrogen mazin a Is only coz generate anadipose tissue
- 18. ADJUVANT HORMONALTRIAL DESIGN: J Clin Oncol. 2010; 28:3784-3796 ENDOCRINETHERAPY SIDE EFFECTS : ¡ Cardiovascular toxicity o AI increase risk of hypercholesterolemia o Tamoxifen increase risk of venous thromboembolism (VTE) ¡ Gynecologic toxicity o More common in tamoxifen (á risk of uterine cancer, benign endometrial, hysterectomy, and vaginal discharge) ¡ Menopausal symptoms o Hot flashes (Tamoxifen > AI) o Vaginal dryness (AI >Tamoxifen) J Clin Oncol. 2010; 28:3784-3796 ENDOCRINETHERAPY SIDE EFFECTS : ¡ Musculoskeletal toxicity o AIs are associated with greater loss of bone mineral density and fractures o Bisphosphonate therapy can mitigate AI-associated loss of bone density § AIs cause a musculoskeletal/arthralgia syndrome o pain, stiffness, or achiness o a 2-4 week break will dramatically reduce symptoms J Clin Oncol. 2010; 28:3784-3796 JCO Oncol Pract. 2020; 16:733-739 ENDOCRINETHERAPY SIDE EFFECTS : ¡ Endocrine toxicities management ASCO EDUCATIONAL BOOK pin risk cardiovascular toxic w.nai.eugradesa discon in a week then re challenges more tamoxifen a Is
- 19. METASTATIC BREAST CANCER MANAGEMENT(STAGE IV) NCCNV1.2021 GENERAL CONSIDERATION: ¡ Goals of therapy: palliation, prolongation of life (if possible) and to maximize quality of life ¡ Bone and soft tissue metastases tend to have a better prognosis and are more likely to respond to endocrine therapy. ¡ Symptomatic visceral metastases generally require chemotherapy due to need for rapid response. Metastasis breast cancer Visceral involvement Systemic therapy HER-2 positive CMT+antiHER- 2 HER-2 negative CMT ± Atezolizumab No visceral involvement HR positive HER-2 positive ET ±AntiHER-2 HER-2 negative ET HR negative HER-2 positive CMT + antiHER-2 HER-2 negative CMT ± Atezolizumab ENDOCRINETHERAPY IN ADVANCED BREAST CANCER: ¡ Evolving standard of care endocrine therapy landscape regimens for HR+/HER2- MBC Anastrozole PI. Exemestane PI. Letrozole PI. Fulvestrant PI. Everolimus PI. Palbociclib PI. Ribociclib PI.Abemaciclib PI. Alpelisib PI. Brufsky. Cancer Treat Rev. 2017;59:22.Lim E. Oncology (Williston Park). 2012;26:688.Croxtall. Drugs. 2011;71:363.Cohen. Oncologist. 2001;6:4. involve lung liver brain Yuniboness crisis non visceral Hr Her viscera p.er triple neg with f ne with mono immunotherapy papositive it trastummab boxetaxeltirastummabtpertuarmab AIs series boxetaxeltirastnzumabtpertnzuma a uue.int with.br uoinhi cidib mom Doxorubicin pm expression i iatezolizumab itinesingle agent withimmunotx paclitaxel pompositive expression scorepembrolizumab
- 20. COMBININGTARGETED AND ANTIESTROGEN THERAPIES TO OVERCOME RESISTANCE IN HR+ ADVANCED BC ¡ ~ 50% of HR+ MBCs do not benefit from ET due to resistance ¡ Mechanisms of resistance may include loss/alteration of ER expression; overexpression/activation of GF receptors; or activation of downstream signal transduction pathways Brufsky. Oncologist. 2018;23:528. AlFakeeh. Curr Oncol. 2018;25:S18. ENDOCRINETHERAPY IN ADVANCED BREAST CANCER: SELECTIVE ESTROGEN RECEPTOR DOWNREGULATORS (SERDS) ¡ Fulvestrant ¡ Binds to Estrogen receptor and antagonizes receptor ¡ Down-regulates receptor expression ¡ Dose: 500 mg IM on D1, 15, 29 and once monthly thereafter Oncol Ther (2017) 5:17–29 SELECTIVE ESTROGEN RECEPTOR DOWNREGULATORS (SERDS) and.line Erbulin metastatis are tamoxifen proliferation aso becomeitiness spine t i min abetter
- 21. CDK 4/6 INHIBITORS: ¡ The Role of CDK4/6 in Breast Cancer o Growth of HR+ MBC is dependent on cyclin D1, a direct transcriptional target of ER o Cyclin D1 activates CDK4/6, resulting in G1-S phase transition and cell cycle entry[1] o Some cell-line models of endocrine resistance show dependence on cyclin D1 and CDK4/6[2,3] 1. Asghar. Nat Rev Drug Discov. 2015;14:130. 2. Miller. Cancer Discov. 2011;1:338. 3. Thangavel. Endoc Relat Cancer. 2011;18:333. CYCLIN D1 AND CDK4/6 REGULATE G1-S CHECKPOINT, DRIVE CELLULAR PROLIFERATION DOWNSTREAM OF SIGNALING PATHWAYS: Lange. Endocr Relat Cancer. 2011;18:C19. Kundsen. Trends Cancer. 2017;3:39.Otto. Nat Rev Cancer. 2017;17:93.Corona. Drug Des Devel Ther. 2018.12:321. Tripathy. Clin Cancer Res. 2017;23:3251-3262. IMPACT OF CDK4/6 INHIBITION ON PFS FIRST-LINE SETTING: Phase III Study PALOMA-2[1,2] MONALEESA-2[3,4] MONARCH-3[5,6] MONALEESA-3[7,8] MONALEESA-7[9] Setting 1st line 1st line 1st line 1st and 2nd line 1st line* Endocrine partner Letrozole Letrozole Letrozole or anastrozole Fulvestrant Tamoxifen, letrozole, or anastrozole CDK4/6 inhibitor Palbociclib Ribociclib Abemaciclib Ribociclib Ribociclib No. patients 666 668 493 365 672 HR 0.563 0.56 0.54 0.55 0.55 PFS, mos 27.6 vs 14.5 25.3 vs 16 28.18 vs 14.76 33.6 vs 19.2 23.8 vs 13.0 ORR, % 55.3 vs 44.4 52.7 vs 37.1 59 vs 44 40.9 vs 28.7† 41 vs 30 1. Finn. NEJM. 2016;375:1925.2. Rugo. Breast Cancer Res Treat. 2019;174:719.3. Hortobagyi. NEJM. 2016;375:1738. 4. Hortobagyi. Ann Oncol. 2018;29:1541. 5. Goetz. JCO. 2017;35:3638.6. Johnston. NPJ Breast Cancer. 2019;5:5. 7. Slamon. JCO. 2018;36:2465. 8. Slamon. NEJM. 2020;382:514. 9. Tripathy. Lancet Oncol. 2018;19:904. *1st line ET; up to 1 prior line of CT permitted in advanced setting (14% of patients had received CT in advanced setting). †Includes 1st and 2nd line. IMPACT OF CDK4/6 INHIBITION ON PFS: SECOND-LINE SETTING Phase III Study PALOMA-3[1,2] MONARCH-2[3] MONALEESA-3[4,5] Setting 2nd line 2nd line 1st and 2nd line Endocrine partner Fulvestrant Fulvestrant Fulvestrant CDK4/6 inhibitor Palbociclib Abemaciclib Ribociclib No. patients 521 669 346 HR 0.50 0.536 0.57 PFS, mos 11.2 vs 4.6 16.9 vs 9.3 14.6 vs 9.1 ORR, % 25 vs 11 48.1 vs 21.3 32.4 vs 21.5* Different Patient Populations Any # prior ET 1 prior CT allowed Only 1 prior ET No prior CT allowed *ORR includes 1st- and 2nd-line patients. 0-1 prior ET No prior CT allowed 1. Cristofanilli. Lancet Oncol 2016;17:425. 2. Turner. NEJM. 2018;379:1926. 3. Sledge. JAMA Oncol. 2020;6:116. 4. Slamon. JCO. 2018;36:2465. 5. Slamon. NEJM. 2020;382:514. me combination p survival.iprogressionfree arrolea trozole aIs corallo inhibitors c cidib then this way line serbstmtor inh lwpt.no Advanced stageat first liner craweslantteverolimus I arpositivey t.uwestanttcbr.am inhibitors ribocidib roleotendocrinet Serbs
- 22. CDK4/6 INHIBITORS: COMPARISON OF KEY DOSING AND ADMINISTRATION CHARACTERISTICS Characteristic Palbociclib[1-3] Ribociclib[4,5] Abemaciclib[5,6] Target (IC50,nM) CDK4 (11); CDK6 (15) CDK4 (10); CDK6 (39) CDK4 (2); CDK6 (10) Route PO PO PO Dose, mg 125 QD 600 QD Monotx: 200 BID Combo with ET: 150 BID Schedule 3 wks on/1 wk off 3 wks on/1 wk off Continuous Half-life, hr 27 32.6 17-38 1. DeMichele. Clin Cancer Res. 2015;21:995. 2. Hamilton. Cancer Treatment Rev. 2016;45:129. 3. Costa. Ann Oncol. 2017;28:44. 4. Infante. Clin Cancer Res. 2016;22:5696. 5. Barroso-Sousa. Breast Care. 2016;11:167. 6. Dickler. Clin Cancer Res. 2017;23:5218. ¡ Abemaciclib,palbociclib, and ribociclib can be taken with or without food ¡ Medication should be taken at approximately the same time each day ¡ Avoid concomitant use of strong CYP3A4 inhibitors and inducers TOXICITY MONITORING AND MANAGEMENT: ¡ Key AEs With CDK4/6 Inhibitors: Monitoring and Prevention TOXICITY MONITORING AND MANAGEMENT: ¡ Dose Modifications Dose Level Abemaciclib + Fulvestrant or AI Abemaciclib Monotherapy Palbociclib Ribociclib Recommended starting dose 150 mg BID 200 mg BID 125 mg/day 600 mg/day First dose reduction 100 mg BID 150 mg BID 100 mg/day 400 mg/day Second dose reduction 50 mg BID 100 mg BID 75 mg/day 200 mg/day Further dose reductions Discontinue if further dose reductions needed beyond 50 mg BID 50 mg BID Discontinue if further dose reductions needed beyond 75 mg/day Discontinue if further dose reductions needed beyond 200 mg/day TOXICITY MONITORING AND MANAGEMENT: ¡ Management of Interstitial Lung Disease/Pneumonitis ¡ Rate of ILD/pneumonitis with CDK4/6 inhibitors ranges from 1.0% to 3.3% ¡ Grade 3/4 AEs occurred in 0.1% to 0.6% of patients ¡ Patients should be counseled on importance of contacting healthcare provider in case of dry cough with/without fever[1-3] ¡ Monitor regularly for pulmonary symptoms or radiologic changes indicative of ILD or pneumonitis (eg, hypoxia, cough, dyspnea, interstitial infiltrates)[1-3] ¡ If pneumonitis suspected, interrupt therapy immediately ¡ Seek pulmonary consultation and consider early institution of corticosteroids[4] ¡ Permanently discontinue if recurrent symptomatic or severe ILD/pneumonitis 1. Abemaciclib PI. 2. Palbociclib PI. 3. Ribociclib PI. 4. Jazieh. Expert Rev Anticancer Ther. 2019;19:917. www.wm oordneutropeniapneumonitis disc on every day 2 minion g ra ds w wnor then diam Hold
- 23. ENDOCRINE RESISTANCE IN ER- POSITIVE BREAST CANCER: qPI3K/mTOR pathway is frequently altered in HR+ BC and has been implicated in resistance to endocrine therapies q~ 40% of HR+ BC harbor a PIK3CA mutation, leading to hyperactivation of the PI3K pathway qPI3K signaling promotes estrogen-independent growth of ER+ BC cells, and this growth is inhibited by the addition of PI3K inhibitors to antiestrogens[6-8] Future Med. Chem. (2015) 7(12) 1511-19. BOLERO-2: EXEMESTANE ± EVEROLIMUS IN NONSTEROIDAL AI–REFRACTORY ABC: Baselga J, et al. N Engl J Med. 2012;366:520-529. BOLERO-2: IMPROVED PFSWITH MTOR INHIBITION: Yardley. Adv Ther. 2013;30:870. Baselga. NEJM. 2012;366:520. BOLERO-2:TOXICITY ¡ Understanding and Modifying Toxicity Associated With Everolimus q Phase II SWISH trial: steroid mouthwash‡ essentially eliminated stomatitis in postmenopausal patients with HR+/HER2- MBC receiving everolimus + exemestane Grade ≥ 2 stomatitis was 2.4 (n = 2) by 8 wks in SWISH vs 27.4% by 8 wks in BOLERO-2 (primary endpoint) and 33% over total study duration Rugo. Lancet Oncol. 2017;18:654. mtor Inhibitors combination n wn.es into resistance combination bettersurvival but.mn stomatitis a Is alone a oexamethasone stomatitis imgnomia.mg ml
- 24. APPROACHTOTHERAPY FOR HR+/HER2- MBC: MOVE TO PERSONALIZATION 1. Cardoso. Ann Oncol. 2018;29:1634. 2. Abemaciclib PI. 3. Palbociclib PI. 4. Ribociclib PI. 5. Alpelisib PI. 6. Fribbens. JCO. 2016;34:2961. 7. Bardia. SABCS 2017. Abstr PD5-08. 8. Everolimus PI. 9. Olaparib PI. 10. Talazoparib PI. 11. Modi. JCO. 2020;38:1887. 12. Smyth. Cancer Discov. 2020;10:198. 13. Bardia. ASCO 2018. Abstr 1004. ANTI-HER-2 IN ADVANCED BREAST CANCER: PHASE III CLEOPATRA STUDY:TRASTUZUMAB AND DOCETAXEL ± PERTUZUMAB IN HER2+ MBC Baselga J, et al. N Engl J Med. 2012;366:109-119. PHASE III CLEOPATRA STUDY: PFS AND OS Baselga J, et al. N Engl J Med. 2012;366:109-119. HR positive HER 2 positive Herceptin 1 then f mid line rat itine addthis.be er combination pertuzumab in survival
- 25. CURRENT APPROACH FOR SEQUENCINGTHERAPY 1. Giordano. JCO. 2018;36:2736. PHASE III EMILIA STUDY:T-DM1VS LAPATINIB/CAPECITABINE IN HER2+ MBC Verma S, et al. N Engl J Med. 2012;367:1783-1791. PHASE III EMILIA STUDY:T-DM1VS LAPATINIB/CAPECITABINE IN HER2+ MBC Verma S, et al. N Engl J Med. 2012;367:1783-1791. TUCATINIB: HER2-SELECTIVETKI Borges. ASCO 2016. Abstr 513. Borges. JAMA Oncol. 2018;4:1214. emtan.me better better become andine docetaxel intelineirrorias it
- 26. HER2CLIMB: PHASE II STUDY DESIGN Murthy. SABCS 2019. Abstr GS1-01. Murthy. NEJM. 2019;382:597. HER2CLIMB: PFS AND OS: Murthy. SABCS 2019. Abstr GS1-01. Murthy. NEJM. 2019;382:597. TUCATINIB: ¡ Indication: o Combination with trastuzumab/ capecitabine for treatment of advanced, unresectable or metastatic HER2+ BC, including patients with brain metastases, who have received ≥ 1 previous HER2-targeted therapy ¡ Dose: 300 mg taken orally twice daily with or without food ¡ Tucatinib can cause severe diarrhea; administer antidiarrheal treatment as clinically indicated ¡ Tucatinib can cause severe hepatotoxicity o Monitor ALT,AST, and bilirubin prior to starting tucatinib, q 3 wks during treatment, and as clinically indicated ¡ Management of AEs may require temporary interruption, dose reduction, or discontinuation TUCATINIB: ¡ Dose modification Dose Level Tucatinib Recommended starting dose 300 mg BID First dose reduction 250 mg BID Second dose reduction 200 mg BID Third dose reduction 150 mg BID Further dose reductions Permanently discontinue in patients unable to tolerate 150 mg BID norbecome ind line means as it bid HER 2 positive
- 27. MANAGEMENT OF METASTASIS TNB: ¡ Chemotherapy o Single agent and combination regimen can be used o Combination chemotherapy provides little higher rate of response q E1193 trial ØSingle agents (Doxorubicin, Paclitaxel) showed equivalent efficacy ØCombination (Doxorubicin+Paclitaxel) showed superior overall response rates and time to TTF Ø Combination did not improve either survival or quality of life compared to sequential single-agent therapy o Continue 1st line chemotherapy until progression J Clin Oncol. 2003; 21(4): 588-92. MANAGEMENT OF METASTASIS TNB: ¡ Chemotherapy PHASE III EMBRACETRIAL OF ERIBULIN VSTPC FOR HEAVILY PRETREATED MBC Cortes J, et al. Lancet. 2011;377:914-923. PHASE III EMBRACETRIAL Cortes J, et al. Lancet. 2011;377:914-923. Triple neg i nothing Doxorubicin pm expression i iatezolizumab itinesingle agent withimmunotx c Paclitaxel pmpositive pin expression no scorepembrolizumab Chemotherapy and line Erbulin r e just improve L single agent ok mid line a new drug anti microtubule I am for
- 28. ADDITIONALTARGETEDTHERAPIES AND ASSOCIATED BIOMARKER TESTING FOR RECURRENT OR STAGE IV DISEASE IMMUNOTHERAPY: ROLE OF COMBINATION BETWEEN CMT AND ICIS: Annals of Oncology 30: 219–235, 2019 ATEZOLIZUMAB + NAB-PACLITAXEL IN PATIENTSWITH UNTREATED ADVANCEDTNBC (IMPASSION130): NEJM. 2018;379:2108. air oiligand program death imith tripienegas chemotx recombinationoverall survival nanoalbuminbound paclitaxel
- 29. IMPASSION130 UPDATE: OS IN ITT POPULATION AND OS BY PD-L1 STATUS: KEYNOTE-355: STUDY DESIGN Lancet 2020; 396: 1817–28 KEYNOTE-355: PFS Lancet 2020; 396: 1817–28 Early breast cancer ER negative HER-2 positive Node (+) or Node (-) with T>1cm Adj.CMT+ Trastuzumab HER-2 negative Node (+) or Node (-) with T>1cm Adj. CMT ER positive HER-2 negative Node (+) Adj. CMT followed by adj. ET Node (-) T ≤ 0.5 cm Adj. ET T >0.5 cm Oncotype Dx RS ≥ 31 Adj. CMT followed by adj. ET RS < 31 Adj. ET HER-2 Positive Node (+) or Node (-) with T>1cm Adj.CMT+ Trastuzumab followed by adj. ET CMT = Chemotherapy ET = Endocrine therapy Adj.=Adjuvant treatment Gbenititlunddpm ipositive alone survival orbenitithrawcombinedpositivesarezio
- 30. Metastasis breast cancer Visceral involvement Systemic therapy HER-2 positive CMT+antiHER- 2 HER-2 negative CMT ± Atezolizumab No visceral involvement HR positive HER-2 positive ET ±AntiHER-2 HER-2 negative ET HR negative HER-2 positive CMT + antiHER-2 HER-2 negative CMT ± Atezolizumab THANKYOU FORYOUR ATTENTION