
Recommended
Recommended
More Related Content
Similar to refreshed laparoscopic burch colposuspension.pptx
Similar to refreshed laparoscopic burch colposuspension.pptx (20)
Recently uploaded
Recently uploaded (19)
refreshed laparoscopic burch colposuspension.pptx
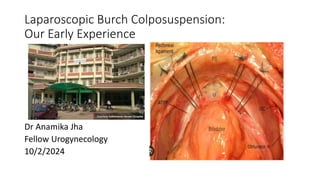
- 1. Laparoscopic Burch Colposuspension: Our Early Experience Dr Anamika Jha Fellow Urogynecology 10/2/2024
- 2. Contents • Introduction • Classification • Surgical management and complications • Our experience • References
- 3. • Burch colposuspension is an operation used to treat Stress Urinary Incontinence(SUI). • SUI- Involuntary leakage of urine on effort or exertion or sneezing or coughing(ICS). Incidence: • Urinary incontinence - 30% to 40%. • SUI - the most common form of urinary incontinence in women (50%) .
- 4. Pathophysiology • In a continent individual, increased abdominal pressure is evenly distributed over the bladder, bladder neck, and urethra, allowing the urethra to withstand the pressure and maintain continence. • In a person with pure stress urinary incontinence, either the urethra is hypermobile or the sphincter is intrinsically deficient.
- 5. • In urethral hypermobility, the urethral vesicular junction (UVJ) is displaced extra-abdominally, and the increased intra-abdominal pressure is unevenly distributed such that the sphincter can no longer withstand the pressure and urine leaks. • With intrinsic sphincter deficiency (ISD), the UVJ is not hypermobile; however, the maximal urethral closing pressure, the Valsalva leak-point pressure, or both are too low to withstand the increase in intra-abdominal pressure and, thus, urine leaks past the sphincter.
- 6. Blaivas Classification of stress incontinence: • Type 1: anatomical, due to hypermobility of the urethrovesical angle • Type 2: rotational descent of the bladder base • Type 3: intrinsic sphincter deficiency (ISD)
- 7. Operations for SUI When non-surgical management for stress urinary incontinence has failed, and the woman wishes a surgical procedure, : • Colposuspension (open/laparoscopic/robotic) • Autologous rectus fascial sling • Retropubic mid-urethral mesh sling (TOT/TVT) NICE GUIDELINE 2019
- 8. Principles of surgery • Restoration of normal anatomy to maintain bladder neck and proximal urethra as intra-abdominal structures. • Strengthening support of bladder neck and proximal urethra preventing funneling of vesicourethral junction in response to intravesical pressure. • To increase functional urethral length
- 9. Retropubic Colposuspension Surgeries • The modern era of retropubic surgery for stress incontinence began in 1949, when Marshall et al. described their technique for urethral suspension in a man with post prostatectomy incontinence. • several modifications of this operation has been done. • This procedure is performed suprapubically (through low abdominal incision) to reach the space of Retzius.
- 10. Retropubic Colposuspension Surgeries • Based on “Delancey’s Hammock Theory” • Marshall–Marchetti–Krantz (MMK):(1949) endopelvic fascia fixed to periostuem of symphysis pubis: obsolete • Burch procedures: (1961) periurethral tissue fixed to Cooper’s ligament • Can be done via Open or laparoscopic method
- 11. Technique of Burch colposuspension
- 14. Vaginal cuff and bilateral adnexa are identified. Retrograde filling of bladder to identify its margins. Parietal peritoneum is retracted posteriorly away from the anterior abdominal wall. Peritoneum is entered to access the space of Retzius. Space of Retzius is a potential space and opens with the help of pneumodissection from the insufflated abdomen. Procedure
- 15. • Dissection down to the level of Cooper ligaments is performed, with the urethra, ureterovesical junction and the lower margin of the bladder all being exposed. • Placement of a finger or vaginal manipulator into the vagina can help with identification of the borders of the vaginal walls. • Suspension sutures are placed; suture should pass through the endopelvic fascia and vagina without entering the vaginal epithelium; to help with suture placement, an assistant has a finger on vagina, placing upward pressure on the anterior vaginal wall. • Sutures are brought up to Cooper ligament on the ipsilateral side and tied.
- 17. • Successful outcome following colposuspension: 85-90% at 1 year and 70% at 20 years. • A recent 2017 Cochrane review showed that Burch and other retropubic colposuspension procedures has a long-term (5 years or more) success rates of around 70% . • Compared to pubovaginal slings, open colposuspension is associated with a lower risk of voiding dysfunction, but with a higher risk of subsequent pelvic organ prolapse.
- 18. Complications • Short term complications Intra operative vascular injury, bladder and urethral injury Infections Voiding difficulties • Long term complications De novo detrusor overactivity(14 - 17%) Posterior vaginal wall prolapse(14 - 49%) Vault or cervical prolapse(42%) Dyspareunia (2-5%) Recurrent UTI (4.5%) Erosion of non-absorbable sutures
- 19. Cases done in KMH in 2023 • TOT-15 • Laparoscopic Burch Colposuspension-18
- 20. Complications • Failed surgery- 2 (Neurogenic Bladder -1d/t DM-2:Hematoma and infection in Burch sutures) • Bladder injury -2 • Port site infection-3 • Urinary retention -1
- 21. References • Walters MD.Karram MM.Urogynecology and Reconstructive Pelvic Surgery.4th edition.USA:Elsevier;2007 • Berek JS. Berek and Novak’s gynecology. 15th ed. USA: Lippincott Williams and wilkins; 2012 • Hoffman BL,Schorge JO,Bradshaw KD,Halvorson LM,Schaffer JI,Corton MM.Wiliams Gynaecology.new york,USA:McGraw-Hill Education;2016.Chapter 23,Urinary incontinence;p.514-37. • Abrams P, ArtibaniW, Cardozo L, Khoury S,Wein A.Clinical Manual of Incontinence in women-based on reports of 3rd international consultation on continence.21sted.Paris, France: Health publications Ltd ;2005 • Cardazo L.Staskin D.Textbook of Female Urology and Urogynecology.5th edition.
Editor's Notes
- ISD=maximal urethral closure pressure <20 cm H2O and/or a Valsalva leak-point pressure <60 cm H2O
- According to cause
- Network meta-analysis of over 21,000 women from 175 trials, obtained from earlier meta-analyses and subsequent trials, reported SUI cure rates of 89.4 percent for traditional bladder neck sling, 89.1 percent for retropubic MUS, 76.6 percent for open colposuspension, and 64.1 percent for transobturator MUS
- Procedure is lifting and fixation of the urethra and bladder neck to the pubic bone or ligaments
- After 2 sutures are placed on each side, they are passed through pectineal ligament, so that all four suture ends exit above the ligament to facilitate knot tying. Inset: when placing the sutures. One should take the full thickness of vaginal wall, excluding the epithelium, with the needle parallel to urethra. This is best achieved by suturing over the finger placed vaginally
- Culposuspension: a. Burch b.MMK c. culposuspension using white line of pelvic fascia