JOURNAL READING
PSYCHIATRY
RSKD MALUKUPROVINCE
FACULTY OF MEDICINE
PAPUA UNIVERSITY
Supervisor : dr. Sherly Yacobus, Sp. KJ
Compiled by : Ester Novella Duwit
Background
Preventing relapseand hospitalization in schizophrenia is a major public
health challenge.
Antipsychotic medications reduce relapse risk (NNT = 3) and lower overall
mortality rates.
Long-acting injectable antipsychotics (LAIs) are more effective than oral
medications.
Adherence Issues
Relapses have serious consequences, especially in early stages of illness.
Second psychotic episodes tend to respond less well to treatment than the
first.
Studies show that 35.7% of patients discontinue medication within 30 days,
and 54.3% within 60 days after first hospitalization.
LAIs can improve adherence, but physicians often consider LAIs only after
repeated relapses.
INTRODUCTION
FACULTY OF MEDICINE
PAPUA UNIVERSITY
5.
Limitations of PreviousResearch
Some RCTs and observational studies show LAIs are
superior; others do not.
RCT participants tend to be more adherent than general
patient populations.
Large simple trials are needed to provide more
representative and real-world data.
INTRODUCTION
FACULTY OF MEDICINE
PAPUA UNIVERSITY
6.
Study Objective
Toassess time to first psychiatric hospitalization between
LAI aripiprazole monohydrate and antipsychotic
treatment as usual over a 2-year period.
Focus on early-phase schizophrenia patients before a
pattern of repeated hospitalizations develops.
OBJECTIVE
FACULTY OF MEDICINE
PAPUA UNIVERSITY
7.
Study Design
PRELAPSEStudy : Investigator-initiated, multicenter,
cluster-randomized clinical trial.
Clinics were divided into two groups: LAI treatment
(AOM) vs. usual antipsychotic treatment (CC).
Participants only consented to the treatment assigned to
their clinic—not to individual randomization.
Enrollment: Dec 2014 – Final Assessment: Mar 2019.
Participants gave written informed consent before any
procedures.
METHODS
FACULTY OF MEDICINE
PAPUA UNIVERSITY
8.
Location :
Clinicseligible if they had:
Early-phase schizophrenia patients,
LAI treatment capacity,
Willingness to be randomized.
Clinics paired by characteristics (academic/community).
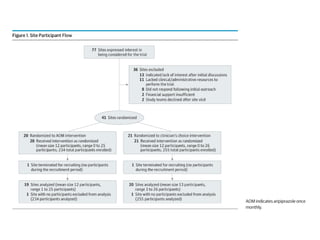
41 clinics randomized; 39 remained active across U.S.
state:
19 clinics (AOM group)
20 clinics (CC group)
METHODS
FACULTY OF MEDICINE
PAPUA UNIVERSITY
9.
Statistical Analysis, consistof :
Primary: Cox regression with robust sandwich estimator
(accounts for clustering).
Sensitivity: Discrete-time mixed-effects survival model.
Secondary:
Poisson regression: Hospitalization rates,
Linear mixed models: Changes in QLS, BPRS.
Software: SAS v9.4
Visualization: Kaplan-Meier survival curve.
STATISTICAL ANALYSES
FACULTY OF MEDICINE
PAPUA UNIVERSITY
10.
Inclusion Criteria:
DSM-5schizophrenia diagnosis via SCID-5,
<5 years antipsychotic use,
Aged 18–35,
Capable of informed consent.
Exclusion Criteria:
Other primary psychiatric diagnosis,
Pregnant/lactating,
Unstable medical condition,
Prior clozapine use,
Aripiprazole intolerance (AOM sites only)
Participant Eligibility
FACULTY OF MEDICINE
PAPUA UNIVERSITY
11.
Intervention Protocol
AOMGroup: Free AOM + standard services.
AOM prescribed per FDA guidelines (oral lead-in, proper
injection intervals).
Switch to alternate treatment allowed if needed.
CC Group: Standard treatment as determined by clinic
(LAI optional).
INTERVENTION
FACULTY OF MEDICINE
PAPUA UNIVERSITY
12.
Determination of PrimaryOutcome
Data source: Hospitalization, ER, and Crisis (HEC) forms,
completed every 2 months.
Recorded 8 inpatient event types, including:
Psychiatric hospitalization, psychiatric ER visits, detox stays, and crisis
stabilization.
Events cross-checked with Serious Adverse Event (SAE)
reports.
Primary outcome defined as:
Psychiatric hospitalizations,
Overnight stays in crisis units or psychiatric ERs,
Select detox or transitional housing stays with inpatient-like context.
INTERVENTION
FACULTY OF MEDICINE
PAPUA UNIVERSITY
13.
Event Review &Classification
384 total events:
184 classified as psychiatric hospitalization by chair + 1
reviewer.
200 events reviewed by an independent review committee.
Committee: 3 senior psychiatrists + 1 biostatistician
( Joanne Severe, MS).
Events were anonymized and randomly ordered.
INTERVENTION
FACULTY OF MEDICINE
PAPUA UNIVERSITY
14.
Primary Classification Categories
P = Psychotic symptoms present (main cause of
admission),
O = Non-psychotic psychiatric cause (e.g., depression,
anxiety, SI/SA),
U = Undetermined (not enough info or unclear),
D = Detox/Rehab (excluded from primary outcome),
NIV = Not an inpatient visit.
FACULTY OF MEDICINE
PAPUA UNIVERSITY
15.
Additional Subcategories
Commitment-related:Suicidal/homicidal ideation or
attempt,
Internal mood: Depression, anxiety, anger,
Overt/social behavior: Aggression, social issues,
None: No clear secondary reason noted.
FACULTY OF MEDICINE
PAPUA UNIVERSITY
16.
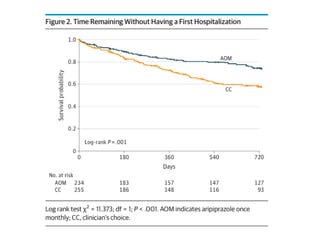
Primary Outcome
Timeto First Psychiatric Hospitalization
Tracked via phone interviews (every 2 months) and resource use
forms (every 4 months).
Verified via records; adjudicated by blinded committee.
Included: Overnight stays in crisis or psychiatric EDs.
Excluded: Substance detox-only admissions.
FACULTY OF MEDICINE
PAPUA UNIVERSITY
17.
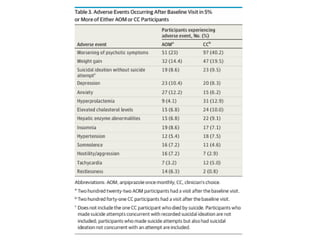
Secondary Outcomes
Assessedat baseline, 12 months, 24 months:
BPRS, CGI, C-SSRS, QLS, SCID-5, RBANS.
Adverse events tracked via clinical visits (every 6
months).
Aim: Limit extra contact beyond normal care.
FACULTY OF MEDICINE
PAPUA UNIVERSITY
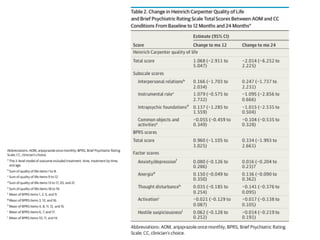
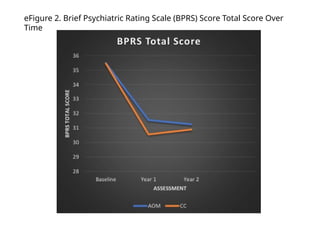
eFigure 2. BriefPsychiatric Rating Scale (BPRS) Score Total Score Over
Time
25.
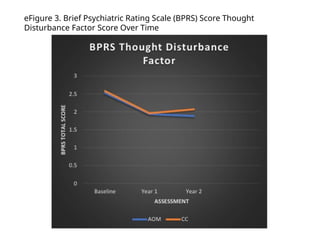
eFigure 3. BriefPsychiatric Rating Scale (BPRS) Score Thought
Disturbance Factor Score Over Time
26.
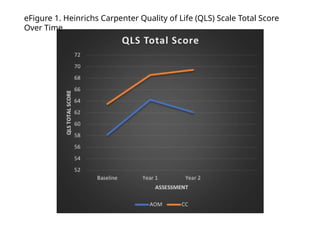
eFigure Summary
eFigure1 – QLS Total Score:
Quality of life stable; no significant group difference.
eFigure 2 – BPRS Total Score:
General symptom improvement over time; no group difference.
eFigure 3 – BPRS Thought Disturbance:
Stable over time; no significant difference between AOM and CC.
RESULT
FACULTY OF MEDICINE
PAPUA UNIVERSITY
27.
The use ofLAIs like aripiprazole monohydrate significantly
delays first hospitalization in early-phase schizophrenia.
These findings suggest clinicians should more broadly
consider LAI treatment for early-phase patients.
Conclusion
LAI use in early-phase schizophrenia led to a clinically
meaningful 44% reduction in first hospitalization risk.
NNT = 7 confirms strong preventive potential of LAIs in
this population.
CONCLUSION
FACULTY OF MEDICINE
PAPUA UNIVERSITY
Limitations
Baseline characteristicsbetween groups were similar,
but:
Cluster randomization could allow for selection effects.
High LAI usage in CC group may underestimate AOM’s
benefits.
Study only tested one LAI formulation (AOM).
Results likely generalizable due to mix of academic and
community sites.
Site training was key—should be implemented more
broadly.
LIMITATIONS
FACULTY OF MEDICINE
PAPUA UNIVERSITY
#9 The statistical analysis methods used in the study included:
Cox Regression (Cox Proportional Hazards Model)
Used to analyze time to first hospitalization (time-to-event analysis), adjusting for intracluster dependence (e.g., participants from the same study site may share similar characteristics).
Discrete-Time Mixed-Effects Survival Analysis
Used as a sensitivity analysis for the Cox model, treating time as a discrete variable and accounting for random effects of study sites, making the results more robust to inter-site variation.
Mixed-Effects Poisson Regression
Employed to analyze the total number of hospitalizations between treatment groups. This model is suitable for count data and accounts for hierarchical data structures, such as patients nested within different study sites.
Three-Level Linear Mixed-Effects Regression
Used to evaluate changes in QLS (Quality of Life Scale) and BPRS (Brief Psychiatric Rating Scale) scores over time. This model considers:
Repeated measures within individuals (longitudinal data),
Clustering at the study site level, and
Individual-level variation within a multilevel data structure.
Kaplan-Meier Survival Plot
A visual tool used to compare the probability of remaining hospitalization-free over time between the two treatment groups, providing an intuitive view of event-time differences.
All analyses were conducted using SAS version 9.4, a statistical software commonly used in clinical and epidemiological research.