SHOULD I SEWOR
SHOULD THEY
GO?
EVALUATION TO
TREAT OR REFER
Lacerations for specialist evaluation:
• Extensive or deep lacerations / puncture wounds on limbs or torso
• Neurovascular compromise
• Fracture, amputation or joint involvement
• Severe contamination
• Significant tissue loss
• Lip lacerations that cross the vermillion border / Lid lacerations
26.
Which
wounds
should
NOT be
sutured?
• DON’TSUTURE:
• Animal bites – unless on face
• Human bites
• Lacerations older than 24 hrs (unless on face)
• Lacerations overlying infected tissue
• Deep puncture wounds
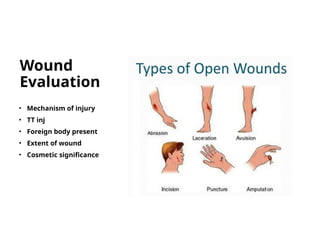
#24 Things to ask yourself:
- Was the Injury blunt, abrading, crush, lacerating, tearing?
Tetanus: My rule of thumb – if greater than 2 years, give it. CDC recommendations are 5 yrs. But I have not encountered once patient who presents for a laceration that can tell me when they last received a Tdap.
Foreign body: If concerned – GET AN XRAY … example of retained dog tooth
Extent of wound –depth, length; is there a neurovascular or tendon injury
#25 One thing I do want to point out with regarding to wounds you should be able to care for is YOUR EXPERIENCE AND ABILITY TO MONITOR WOUND – EITHER IN YOUR COMMUNITY OR CLINIC SETTING.
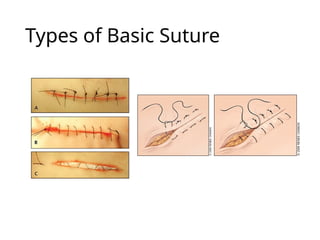
#28 Most wounds can be closed effectively with nonabsorbable, single interrupted sutures.
A running (“baseball”) suture is used for long, low-tension wounds, whereas a subcuticular running suture is ideal for closing small lacerations in low skin-tension areas where cosmesis is important, such as on the face.
The horizontal mattress technique may be the best option for closing gaping or high-tension wounds or wounds on fragile skin because it spreads the tension along the wound edge. The vertical mattress technique is best for everting wound edges in areas that tend to invert, such as the posterior neck or concave skin surfaces