DEFINITION
•Osteogenesis imperfecta a.k.a
FragilitasOssium
•A relatively rare non-sex-linked
hereditary disorder
characterized by an unusual
fragility of bone and
osteoporosis leading to multiple
fractures often from a trivial
cause
4.
EPIDEMIOLOGY
•Estimated incidence is
approximately1 in every 12,000-
15,000 births
•Equal frequency among males and
females and across races and
ethnic groups
•Inheritance can be autosomal
dominant (commonest), autosomal
recessive or sporadic depending on
the type
5.
ETIOPATHOGENESIS
• The fundamentalpathology in osteogenesis
imperfecta is a disturbance in the synthesis of
Type 1 collagen which is the predominant
protein of the extracellular matrix of most
tissues
• Mutation in one of the two genes (COL1A1 and
COL1A2) that carry instructions for making Type
1 collagen
• Bones - this defect results in osteoporosis
thus increasing the tendency to fracture
• Besides bones, type 1 collagen is also a major
constituent of dentin, sclerae, ligaments,
blood vessels and skin
6.
TYPES/CLASSIFICATION
Four basic types
•Type I
• Type II
• Type III
• Type IV
• Type I & IV are the two principal forms
formerly known as Osteogenesis
Imperfecta Tarda
• Types II & III formerly known as
Osteogenesis Congenita
7.
Tarda Form
• Firstnoted during childhood because
of the usual tendency for fractures
• Lax joints and dislocations are
frequent
• Deafness caused by otosclerosis
becomes apparent
• Teeth are discolored, fragile, and
easily broken
• Blue sclerae also become more apparent
owing to the intraocular pigment
8.
Congenita form
•Develops in-uterowith the
infant born with multiple
fractures
•Diagnosis has been established
in-utero by ultrasound through
recognition of angular
deformities of long bones
•Most common 2nd
trimester
ultrasound diagnosis of short,
bent limbs
9.
SILLENCE ET AL
Fourbasic types with subtypes
• Type 1 – commonest
• Over 70% of cases fit into this category
• Autosomal dominant
• Blue sclerae
• Mild bone fragility
• Stature is only mildly reduced
• Deafness is in adult life
• 1A – Normal teeth with minor skeletal change
• 1B – Dentinogenesis imperfecta and more severe
skeletal change
10.
Type 2
• 10%of cases of osteogenesis imperfecta are due
to this spontaneous dominant new mutation
• Usually lethal in-utero or early infancy
• Sclerae are dark blue
• Overall, the bones are grossly demineralised
with thin cortices
• Skull is enlarged with numerous Wormian bones
• Numerous healed/healing fractures seen at birth
• Fractures also occur during delivery
• 2A – long bones are bowed, short and broad
• Ribs are broad with continuous beading
• Numerous fractures are seen
11.
• 2B –long bones same as in 2A but ribs show
less or no beading
• 2C – long bones are thinned, show numerous
fractures with thin and beaded ribs
12.
Type 3 -occurs in 15% of patients
• A severe and progressively deforming type
• Sclerae is blue at birth and normal in
adolescence
• Generally demineralized bone
• Vertebral compression is seen with
kyphoscoliosis
• Long bones are osteoporotic and thin
• Multiple fractures in childhood result in
bowing
• Skull bones show sutures diasthesis and
presence of wormian bones
• Associated dentinogenesis imperfecta
13.
• Type 4– occurs in 5% of patients
• Normal sclerae
• Fractures are seen at birth in 30% and bony
fragility is mild
• 4A – no dental lesion
• 4B – with dentinogenesis imperfecta
14.
CLINICAL FEATURES
• Rangesfrom mild (no deformity) to normal
stature and few fractures to a form that
is lethal during the perinatal period
1. Abnormal bone fragility
2. Blue sclerae
3. Poor teeth
4. Hearing impairment
5. Ligamentous laxity
6. Hypermobility of joints
7. Short stature
8. Easy bruising
15.
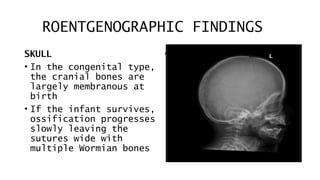
ROENTGENOGRAPHIC FINDINGS
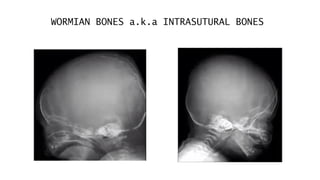
SKULL
• Inthe congenital type,
the cranial bones are
largely membranous at
birth
• If the infant survives,
ossification progresses
slowly leaving the
sutures wide with
multiple Wormian bones
•
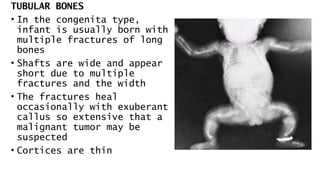
TUBULAR BONES
• Inthe congenita type,
infant is usually born with
multiple fractures of long
bones
• Shafts are wide and appear
short due to multiple
fractures and the width
• The fractures heal
occasionally with exuberant
callus so extensive that a
malignant tumor may be
suspected
• Cortices are thin
18.
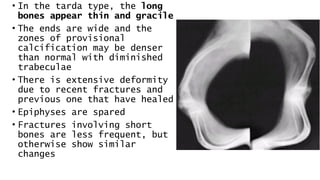
• In thetarda type, the long
bones appear thin and gracile
• The ends are wide and the
zones of provisional
calcification may be denser
than normal with diminished
trabeculae
• There is extensive deformity
due to recent fractures and
previous one that have healed
• Epiphyses are spared
• Fractures involving short
bones are less frequent, but
otherwise show similar
changes
20.
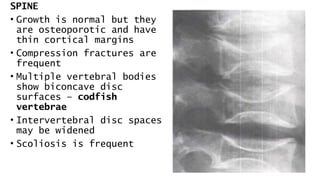
SPINE
• Growth isnormal but they
are osteoporotic and have
thin cortical margins
• Compression fractures are
frequent
• Multiple vertebral bodies
show biconcave disc
surfaces – codfish
vertebrae
• Intervertebral disc spaces
may be widened
• Scoliosis is frequent
21.
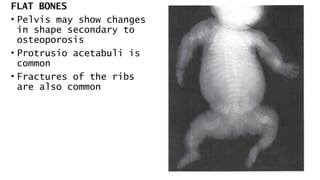
FLAT BONES
• Pelvismay show changes
in shape secondary to
osteoporosis
• Protrusio acetabuli is
common
• Fractures of the ribs
are also common
22.
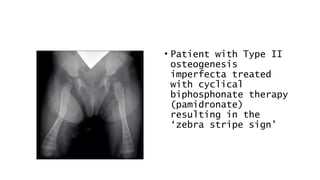
• Patient withType II
osteogenesis
imperfecta treated
with cyclical
biphosphonate therapy
(pamidronate)
resulting in the
‘zebra stripe sign’
23.
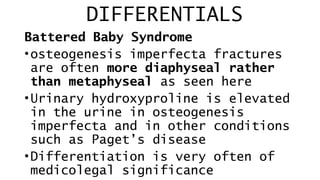
DIFFERENTIALS
Battered Baby Syndrome
•osteogenesisimperfecta fractures
are often more diaphyseal rather
than metaphyseal as seen here
•Urinary hydroxyproline is elevated
in the urine in osteogenesis
imperfecta and in other conditions
such as Paget’s disease
•Differentiation is very often of
medicolegal significance
24.
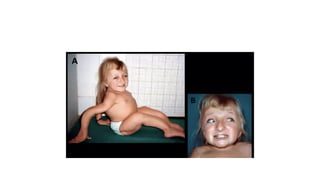
Idiopathic juvenile osteoporosis
•Startsjust before puberty and
usually self-limiting
•Vertebral compression and
characteristically metaphyseal
fractures especially of the
lower limb bones occur
Editor's Notes
#7 Otosclerosis is a localized disease of unknown etiology in which new bone replaces the endochondral bone of the otic capsule










![Osteogenesis Imperfecta [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/osteogenesisimperfectaautosaved-230505163031-62b018a2-thumbnail.jpg?width=640&height=640&fit=bounds)




































