Aiming for a Higher Performing Health Care System: Learning from Cross-National Comparisons
•Download as PPTX, PDF•
2 likes•1,550 views

Robin Osborn, Vice President and Director, International Program in Health Policy and Innovation at The Commonwealth Fund, discusses international health care systems. These slides were presented at the Queen’s Health Policy Change Conference, May 6, 2015 in Toronto, Canada.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (11)
Similar to Aiming for a Higher Performing Health Care System: Learning from Cross-National Comparisons
Similar to Aiming for a Higher Performing Health Care System: Learning from Cross-National Comparisons (20)
More from The Commonwealth Fund
More from The Commonwealth Fund (6)
Recently uploaded
Recently uploaded (20)
Aiming for a Higher Performing Health Care System: Learning from Cross-National Comparisons
- 1. Aiming for a Higher Performing Health Care System: Learning from Cross-National Comparisons Queen’s Health Policy Change Conference May 6, 2015 Toronto, Canada Robin Osborn Vice President and Director International Program in Health Policy and Practice Innovations The Commonwealth Fund 1
- 2. What is a High Performing Health System? • Goals of a High Performance Health System • Best possible health outcomes for everyone • Access to care for all • Excellent patient experiences – patient-centered, coordinated, high quality, safe care for all • Lower cost – accountable for use of resources and elimination of waste • Encourages innovation • Learning health care system 2
- 3. Why Do We Do Cross-National Comparisons? • Benchmark performance • Track policies and reforms • Highlight best practices • Identify variations • Know what is possible 3
- 4. 0 2 4 6 8 10 12 14 16 18 1980 1983 1986 1989 1992 1995 1998 2001 2004 2007 2010 US (16.9%) NET (12.1%)* FR (11.6%) SWIZ (11.4%) GER (11.3%) DEN (11.0%) CAN (10.9%) JPN (10.3%) NZ (10.0%)* SWE (9.6%) NOR (9.3%) UK (9.3%) AUS (9.1%)* GDP refers to gross domestic product. Source: OECD Health Data 2014. Health Care Spending as a Percentage of GDP, 1980–2012 Percent * 2011 4
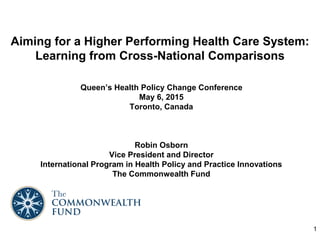
- 5. Mortality Amenable to Health Care, 2006-07 55 57 60 61 61 64 66 76 79 80 83 96 0 20 40 60 80 100 120 140 FR AUS ITA JPN SWE NOR NETH GER NZ DEN UK US 5 * Countries’ age-standardized death rates before age 75; including ischemic heart disease, diabetes, stroke, and bacterial infections. Analysis of World Health Organization mortality files and CDC mortality data for U.S. Source: Adapted from E. Nolte and M. McKee, “Variations in Amenable Mortality—Trends in 16 High-Income Nations,” Health Policy, published online Sept. 12, 2011. Deaths per 100,000 population*
- 6. 6 Overall Views of Health Care System, 2013 Source: 2013 Commonwealth Fund International Health Policy Survey in Eleven Countries. Percent
- 7. Learning from International Surveys 7
- 8. Commonwealth Fund Annual International Surveys: What We Track 8 – QI/Performance feedback – Chronic illness – Use of the ED – Hospital care – Medications – Physician payment/Incentives – System complexity – Health care coverage – Demographics • General themes: – Views of the health system – Access and affordability – Primary care/Medical home – Doctor-patient relationship – Prevention/health promotion – Care coordination – Electronic Health Record – Patient safety • Focus on objective measures rather than opinions.
- 10. Cost-Related Access Problems in the Past Year, Among Adults Age 65 or Older * Had a medical problem but did not visit doctor, skipped medical test or treatment recommended by doctor, and/or did not fill prescription or skipped doses because of the cost. 3 4 4 5 6 6 7 8 9 10 19 0 10 20 30 FR SWE NOR UK NETH SWIZ GER AUS CAN NZ US Percent* Source: 2014 Commonwealth Fund International Health Policy Survey of Older Adults in Eleven Countries. 10
- 11. Could Get Same- or Next-Day Appointment with Doctor or Nurse When Sick or Needed Care, Among Adults Age 65 or Older 11 83 83 81 76 71 69 65 57 54 53 45 0 20 40 60 80 100 FR NZ GER NETH AUS SWIZ UK US NOR SWE CAN Percent Source: 2014 Commonwealth Fund International Health Policy Survey of Older Adults in Eleven Countries.
- 12. Waited Less Than Four Weeks for Specialist Appointment, Among Adults Age 65 or Older 12 86 82 71 64 62 61 60 60 50 46 46 0 20 40 60 80 100 US SWIZ NETH AUS NZ GER FR UK SWE CAN NOR * Base: Saw/Needed to see a specialist in the past two years. Percent* Source: 2014 Commonwealth Fund International Health Policy Survey of Older Adults in Eleven Countries.
- 13. Access to After-Hours Care, Among Adults Age 65 or Older 13 77 71 69 69 66 66 62 55 54 41 37 0 20 40 60 80 100 NETH UK FR NZ SWIZ NOR GER US AUS CAN SWE Source: 2012 and 2014 Commonwealth Fund International Health Policy Surveys. * Base: Needed after-hours care. Percent who said it was somewhat or very easy to get after-hours care without going to the emergency department*
- 14. Emergency Department Use in the Past Two Years, Among Adults Age 65 or Older 14 15 19 21 27 27 29 30 33 35 39 39 0 10 20 30 40 50 FR UK GER NOR SWIZ NETH AUS NZ SWE CAN US Percent Source: 2014 Commonwealth Fund International Health Policy Survey of Older Adults in Eleven Countries.
- 15. 15 Care Coordination and Transitions
- 16. Experienced a Coordination Problem in the Past Two Years, Among Adults Age 65 or Older 16 7 20 21 21 24 24 29 32 35 37 41 0 10 20 30 40 50 FR NZ NETH AUS UK SWE SWIZ CAN US NOR GER * Test results/records not available at appointment or duplicate tests ordered; received conflicting information from different doctors; and/or specialist lacked medical history or regular doctor was not informed about specialist care. Percent* Source: 2014 Commonwealth Fund International Health Policy Survey of Older Adults in Eleven Countries.
- 17. Experienced Gaps in Hospital Discharge Planning in the Past Two Years, Among Adults Age 65 or Older 17 28 38 41 44 54 56 56 59 67 70 0 20 40 60 80 100 US UK AUS CAN FR SWIZ GER NETH SWE NOR * When discharged from the hospital: you did not receive written information about what to do when you returned home and symptoms to watch for; hospital did not make sure you had arrangements for follow-up care; someone did not discuss with you the purpose of taking each medication; and/or you did not know who to contact if you had a question about your condition or treatment. Base: hospitalized overnight in the past two years. Percent* Note: NZ omitted because of small N (fewer than 100 respondents). Source: 2014 Commonwealth Fund International Health Policy Survey of Older Adults in Eleven Countries.
- 18. Primary Care Doctors’ Receipt of Information from Specialists 18 Source: 2012 Commonwealth Fund International Health Policy Survey of Primary Care Physicians. 47 44 44 41 30 24 22 16 13 12 5 0 20 40 60 80 FR NZ SWIZ UK AUS CAN NOR US SWE GER NETH Percent who reported after their patient visits a specialist they always receive information about changes to patient’s drugs or care plan
- 19. 19 Chronic Care and Self-Management
- 20. Patient Engagement in Chronic Care Management, Among Adults Age 65 or Older 20 83 80 76 73 64 62 53 47 41 41 30 0 20 40 60 80 100 Percent who have a chronic condition and had a treatment plan for their condition they could carry out in their daily life Source: 2014 Commonwealth Fund International Health Policy Survey of Older Adults in Eleven Countries.
- 21. Support for Self-Management Between Doctor Visits, Among Adults Age 65 or Older 21 47 30 28 24 24 23 17 16 15 14 9 0 20 40 60 80 100 Contacts them to check in They can contact to ask questions or get advice 84 83 75 75 71 67 65 58 55 53 43 Percent who have a chronic condition and had a health care professional that between doctor visits: Source: 2014 Commonwealth Fund International Health Policy Survey of Older Adults in Eleven Countries.
- 22. 22 Medical Homes
- 23. Patients with a Regular Doctor versus a Medical Home, 2011 Patients with a medical home have a regular practice who is accessible, knows them, and helps coordinate their care Percent Source: 2011 Commonwealth Fund International Health Policy Survey of Sicker Adults in Eleven Countries. 23
- 24. Medical, Medication, or Lab Test Errors in Past Two Years, by Medical Home Percent* * Reported medical mistake, medication error, and/or lab test error or delay in past two years. Source: 2011 Commonwealth Fund International Health Policy Survey of Sicker Adults in Eleven Countries. 24
- 25. 25 Primary Care Practice Infrastructure and Capacity for Improvement
- 26. Doctors’ Use of Electronic Medical Records in Their Practice, 2009 and 2012 26 Source: 2009 and 2012 Commonwealth Fund International Health Policy Survey of Primary Care Physicians. Percent
- 27. Doctor Can Electronically Exchange Patient Summaries and Test Results with Doctors Outside their Practice 27 55 52 49 49 45 39 38 31 27 22 14 0 20 40 60 80 100 NZ SWE NETH SWIZ NOR FRA UK US AUS GER CAN Percent Source: 2012 Commonwealth Fund International Health Policy Survey of Primary Care Physicians.
- 28. Doctor Routinely Receives Electronic Prompts About Potential Problems with Rx Dose or Interaction 28 93 89 88 85 70 58 41 30 26 25 22 0 20 40 60 80 100 NETH NZ AUS UK SWE US FRA CAN GER SWIZ NOR Percent Source: 2012 Commonwealth Fund International Health Policy Survey of Primary Care Physicians.
- 29. Practice Uses Nurse Case Managers or Navigators for Patients with Serious Chronic Conditions 29 Percent 78 73 68 68 59 51 44 43 41 20 0 20 40 60 80 100 UK NETH NZ SWIZ AUS NOR CAN US SWE GER Note: Question asked differently in France. Source: 2012 Commonwealth Fund International Health Policy Survey of Primary Care Physicians.
- 30. Practice Routinely Receives and Reviews Data on Clinical Outcomes 30 Source: 2012 Commonwealth Fund International Health Policy Survey of Primary Care Physicians. 84 81 78 64 54 47 42 23 14 12 0 20 40 60 80 100 UK NETH SWE NZ GER US AUS CAN FR SWIZ Percent
- 31. Financial Incentives and Targeted Support 31 Percent can receive financial incentives* for: AUS CAN FR GER NETH NZ NOR SWE SWIZ UK US Managing patients w/ chronic disease or complex needs 75 70 37 60 77 83 15 49 4 50 21 Enhanced preventive care activities** 42 42 12 23 28 40 17 55 5 37 14 Adding nonphysician clinicians to practice 53 33 3 5 60 36 9 33 4 17 10 Making home visits 57 53 16 51 50 36 45 49 32 20 9 * Including special payments, higher fees, or reimbursements. ** Including patient counseling or group visits. Source: 2012 Commonwealth Fund International Health Policy Survey of Primary Care Physicians.
- 32. Policy Implications 32 • Insurance design matters • Having a “medical home” and after-hours care arrangements make a difference • Innovations in payment and delivery system models are needed to encourage care coordination and better management of complex patients • Chronically ill patients need to be further empowered and supported in self- management, including between scheduled visits • Having electronic medical records is not enough – “meaningful use” matters • More use of performance data and feedback are needed to help primary care practices improve care and patient experiences • And, as countries innovate and transform their health care systems, there is a tremendous opportunity for cross-national learning
- 33. Limitations of Current Cross-National Comparisons • Imperfect performance measures: o Rely heavily on Commonwealth Fund surveys o Outcome indicators are scarce o Few measures of hospital quality o Data does not always lead to a value judgment (e.g., are more MRI machines good or bad?) • Proliferation of country measures but not typically adopted based on international comparability • We need more patient-reported outcome measures • Defining high performance requires subjective judgments • Numbers don’t tell the full story 33
- 34. Monitoring & Tracking Performance: U.S. Efforts 34
- 35. Overall Health System Performance, 2014 35 Source: The Commonwealth Fund State Scorecard Ranking based on access & affordability, prevention & treatment, avoidable hospital use and cost, healthy lives, and equity
- 36. Long Term Supports: Overall Health System Performance, 2014 36 Source: The Commonwealth Fund Scorecard on Long Term Support Services Ranking based on access & affordability, choice of setting and provider, quality of life and quality of care, support for family caregivers, and effective transitions
- 37. Quality: Mortality Amenable to Health Care, by Race and State, 2009-10 37 Source: Commonwealth Fund State Scorecard on State Health System Performance, 2014
- 38. Access: Out-of-Pocket Mean Expenditures, by Race/Ethnicity 38 Source: Center for Financing, Access, and Cost Trends, AHRQ, Household Component of the Medical Expenditure Panel Survey, 2012 Annual out-of-pocket mean expenditures by race/ethnicity
- 39. Quality: Preventable Hospitalizations in New York State, by County 39 Age Adjusted Preventable Hospitalizations Rate per 10,000, Ages 18+ Years, 2008-10 Source: Health Data NY The Prevention Quality Indicators (PQIs) are a set of measures developed by the federal Agency for Healthcare Research and Quality (AHRQ) for use in assessing the quality of outpatient care for "ambulatory care sensitive conditions" (ACSCs). This indicator is defined as the combination of the 12 PQIs that pertain to adults: (1)Short-term complication of diabetes (2)Long-term complication of diabetes (3)Uncontrolled diabetes (4)Lower-extremity amputation among patients with diabetes (5)Hypertension (6)Congestive heart failure (7)Angina (8)Chronic obstructive pulmonary disease (9)Asthma (10)Dehydration (11)Bacterial pneumonia (12)Urinary tract infection. 1st & 2nd Quartiles (<144 per 10,000) 3rd Quartile (144-<162 per 10,000) 4th Quartile (162+ per 10,000)
- 40. Quality: Readmission Rates, by Hospital 40 Heart Failure 30 Day Readmission Rate, by Hospital, 2010-13 Source: CMS Hospital Compare Percent High Performing Hospitals* Low Performing Hospitals** * Examples from top 10% of hospitals **Examples from bottom 10% of hospitals
- 41. Quality: Falls in Long Term Care Institutions, by Nursing Home 41 Percent of Long-Stay Residents Experiencing One or More Falls with Major Injury, 2014 Source: CMS Nursing Home Compare Percent High Performing Nursing Homes* Low Performing Nursing Homes** * Examples in top 10% of nursing homes ** Examples from bottom 10% of nursing homes
- 42. Acknowledgements With appreciation to Dana Sarnak, David Squires, and Michelle Doty for their contributions to this presentation. And, to our International Survey Partners for their support and expertise: • Australia: New South Wales Bureau of Health Information • Canada: Canadian Institute for Health Information, Canadian Institutes of Health Research, Health Quality Ontario, Commissaire à la Santé et au Bien- être du Québec, and Health Quality Council of Alberta • France: Haute Autorité de Santé and Caisse Nationale d’Assurance Maladie des Travailleurs Salariés • Germany: Federal Ministry of Health and the German National Institute for Quality Measurement in Health Care • Netherlands: Ministry of Health, Welfare, and Sport and the Scientific Institute for Quality of Healthcare at Radboud University Nijmegen Medical Centre • Norway: Norwegian Knowledge Centre for the Health Services • Sweden: Ministry of Health and Social Affairs • Switzerland: Federal Office of Public Health • United Kingdom: The Health Foundation