Duchenne muscular dystrophy is an X-linked recessive genetic disorder. For a mother who is a carrier and a father who does not have the gene, the chance that their son will have Duchenne muscular dystrophy is 25%.
Question #: 125Type II (beta) errors in clinical studies are minimized by performing which of the following? 1- Power analysis 2- Bonferroni correction 3- Mann-Whitney U test 4- Logistical regression analysis 5- Increase sample size by 20%
3.
Preferred Response: 1Type I error —Probability of rejecting the null hypothesis when it is really true. The probability of making a type I error is denoted by the Greek letter α Type II error —Probability of failing to reject a null hypothesis that is really false. The probability of making a type II error is denoted by the Greek letter β Power —Probability that the sample mean will be sufficiently different from the mean under null hypothesis to allow rejection of the null hypothesis Bonferroni correction is a method used to address the problem of multiple comparisons . The correction is based on the idea that if an experimenter is testing n dependent or independent hypotheses on a set of data, then one way of maintaining the familywise error rate is to test each individual hypothesis at a statistical significance level of times what it would be if only one hypothesis were tested Mann–Whitney U test a non-parametric test for assessing whether two independent samples of observations have equally large values. logistic regression (sometimes called the logistic model or logit model ) is used for prediction of the probability of occurrence of an event by fitting data to a logit function logistic curve . It is a generalized linear model used for binomial regression . Like many forms of regression analysis, it makes use of several predictor variables that may be either numerical or categorical. For example, the probability that a person has a heart attack within a specified time period might be predicted from knowledge of the person's age, sex and body mass index
4.
Question #: 132The immune response to metallic orthopaedic implants is typically what type? 1- Type I (Ig-E mediated) 2- Type II (antibody mediated) 3- Type III (immune complex mediated) 4- Type IV (delayed-type hypersensitivity reaction) 5- Type V (Ig-M mediated)
5.
Preferred Response: 4Type I hypersensitivity is mediated by IgE , which triggers degranulation of mast cells and basophils when cross-linked by antigen. [74] Type II hypersensitivity occurs when antibodies bind to antigens on the patient's own cells, marking them for destruction. This is also called antibody-dependent (or cytotoxic) hypersensitivity, and is mediated by IgG and IgM antibodies. [74] Type III hypersensitivity reactions- Immune complexes (aggregations of antigens, complement proteins, and IgG and IgM antibodies) deposited in various tissues trigger. [74] Type IV hypersensitivity (also known as cell-mediated or delayed type hypersensitivity ) usually takes between two and three days to develop. Type IV reactions are involved in many autoimmune and infectious diseases, but may also involve contact dermatitis ( poison ivy ). These reactions are mediated by T cells , monocytes , and macrophages A routine skin test reveals a prevalence of metal sensitivity of 0.2% for chromium, 1.3% for nickel, and 1.8% for cobalt. After placement of metal implants, sensitization (change from negative to positive) occurs in 2.7% for chromium, 3.8% for nickel, and 3.8% for cobalt. Desensitization (change from positive to negative) occurs in 0% for chromium, 2.1% for nickel, and 3.8% for cobalt. Many patients with implanted metal hardware have positive skin test results for those metals but are completely asymptomatic Type I hypersensitivity to latex involves IgE antibodies that are specific for proteins from the sap of the rubber tree (Hevea brasiliensis) used to make gloves Wiki/emedicine
6.
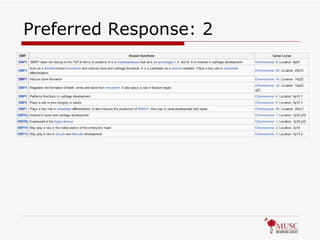
Question #: 139Which of the following bone morphogenetic proteins (BMP) exhibits no osteogenic activity? 1- BMP2 2- BMP3 3- BMP4 4- BMP6 5- BMP7
Question #: 149Marfan syndrome demonstrates what type of inheritance pattern? 1- Autosomal dominant 2- Autosomal recessive 3- X-linked dominant 4- X-linked recessive 5- Germline mutation
9.
Preferred Response: 1Autosomal Dominant; 25% new mutations Mutation is fibrillin 1 gene on chromosome 15q21 (contrast with Ehlers-Danlos which is COL5A1, COL5A2, or COL3A1; defect is in Type V collagen; may be AD or AR) + Walker sign (thumb & small finger overlap when encircling contralateral wrist + Steinburg thumb sign (adduct thumb, make fist, and thumb protrudes from ulnar side of hand) Scoliosis in 60-70% (hard to brace); 60% have dural ectasia so get MRI before OR Mitral valve prolapse, aortic root dilatation
10.
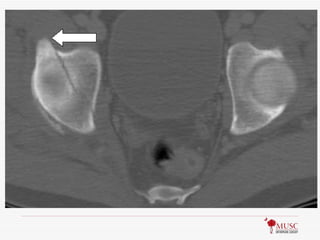
Question #: 160A patient sustains a fracture of the acetabulum. An axial CT scan is shown in Figure 160. What structure takes origin from the region depicted by the arrow? 1- Pectineus 2- Sartorius 3- Iliopectineal fascia 4- Direct (straight) head of the rectus femoris 5- Indirect (reflected) head of the rectus femoris
11.
12.
Preferred Response: 4Rectus femoris has 2 heads: Direct/straight takes origin from AIIS, Indirect/reflected takes origin from groove on the upper brim of the acetabulum Femoral nerve (L2,3,4) Arterial supply: ascending branch of lateral femoral circumflex Pectineus origin from superior surface of pubis; innervated by femoral & obturator (L2,3,4); acts to adduct thigh Sartorius origin from ASIS; innervated by femoral (L2,3); inserts into pes anserinus
13.
Question #: 165Polymorphisms in the genes for the calcitonin receptor, estrogen receptor-1, type I collagen alpha-1 chain, or the vitamin D receptor have been shown to be associated with which of the following bone diseases? 1- Osteopetrosis 2- Osteoporosis 3- Osteomalacia 4- Vitamin D-deficient rickets 5- X-linked hypophosphatemic rickets
14.
Preferred Response: 2Osteopetrosis-failure of osteoclasts resulting in dense bone with no medullary canal; 3 deactivating mutations are known: carbonic anhydrase II, alpha 3 subunit of proton pump; Chloride channel 7 Osteoporosis-normal bone in reduced quantity; >2.5 SDs below peak bone mass (T score <-2.5; remember osteopenia is 1.0-2.5 SDs below peak or T score of -1 to -2.5); multifactorial disease but associated gene defects are Vit D receptor, COL1A1, and LRP5 (low density lipoprotein receptor related protein) Osteomalacia-adult form of rickets; normal quantity, but abnormal bone; cause is related to Vit D pathway Vitamin D-deficient rickets-low intake of Vit D produces bone with poor mineralization X-linked hypophosphatemic rickets-X-linked dominant disorder that leads to phosphate wasting due to mutation in phosphate regulating endopeptidase (PHEX) gene
15.
Question #: 175Of the available osteoconductive bone graft substitutes, which is most rapidly resorbed? 1- Calcium sulfate 2- Calcium phosphate 3- Tricalcium phosphate 4- Coralline hydroxyapatite 5- Collagen-based matrices
16.
Question #: 175Of the available osteoconductive bone graft substitutes, which is most rapidly resorbed? 1- Calcium sulfate : 1-3 Months 2- Calcium phosphate : 6-21 months 3- Tricalcium phosphate : 6-21 months 4- Coralline hydroxyapatite : upto 10 yrs 5- Collagen-based matrices : ? De Long, et al 2007, J Bone Joint Surg Am. 2007;89:649-658.
17.
Preferred Response: 1Bell WH: Oral Surgery, Oral Medicine, Oral Pathology , 650-657, 1964 Resorption of ninety intramuscular implants of different types of bone and bone substitutes were studied radiographically in twenty-two adult mongrel dogs. On the basis of mean resorption time, the implants were resorbed in the following order: plaster of Paris (Calcium sulfate) , autogenous cancellous bone, cathode-ray-sterilized canine cancellous bone, cathode-ray-sterilized human cancellous bone, homologous cancellous bone, fetal bovine bone, bovine cancellous bone, freeze-dried cancellous bone, collapatite, anorganic bone, and polyurethane foam.
18.
Question #: 180Which of the following is an inhibitor of particle-induced osteolysis? 1- Interleukin-1 alpha 2- Interleukin-6 3- Osteoprotegerin 4- Tumor necrosis factor (TNF)-alpha 5- Receptor-activator of nuclear factor KB(RANK) ligand
19.
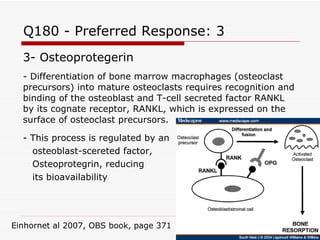
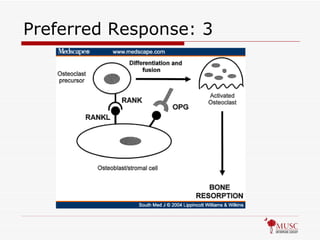
Q180 - PreferredResponse: 3 3- Osteoprotegerin - Differentiation of bone marrow macrophages (osteoclast precursors) into mature osteoclasts requires recognition and binding of the osteoblast and T-cell secreted factor RANKL by its cognate receptor, RANKL, which is expressed on the surface of osteoclast precursors. - This process is regulated by an osteoblast-scereted factor, Osteoprotegrin, reducing its bioavailability Einhornet al 2007, OBS book, page 371
20.
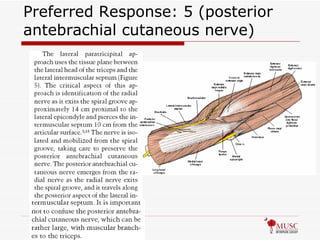
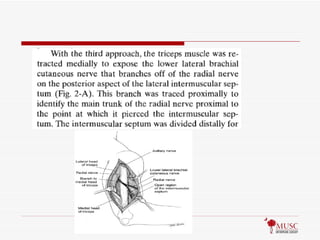
Question #: 188Which of the following nerves serves as an anatomic landmark leading to the radial nerve during a paratricipital approach for humeral shaft fracture fixation? 1- Musculocutaneous 2- Lateral antebrachial cutaneous 3- Medial antebrachial cutaneous 4- Medial brachial cutaneous 5- Posterior antebrachial cutaneous
Question #: 215The Heuter-Volkmann Law is summarized best by which of the following statements? 1- Bone remodels in response to mechanical stimuli. 2- Bone formation is induced in an electronegative zone and resorbed in an electropositive zone. 3- Compression across the growth plate slows longitudinal growth. 4- Tensile load across the growth plate increases longitudinal growth. 5- The bending strength of diaphyseal bone is determined by its diameter raised to the third power.
24.
Preferred Response: 3The Hueter-Volkmann law : Compression across the growth plate slows longitudinal growth, ( and tensile load across the growth plate increases longitudinal growth according to every source I can find…not sure why this was not also correct). Wolff’s Law: bone remodels in response to mechanical stimuli Peizoelectric Theory: Bone formation is induced in an electronegative zone and resorbed in an electropositive zone.
25.
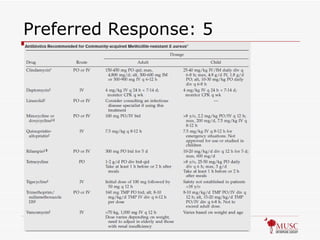
Question #: 239An otherwise healthy 17-year-old wrestler suspects that he has been bitten on the neck by a spider. He has no recent history of hospitalization. Other members of his wrestling team have also recently reported skin lesions. Examination reveals superficial abscess formation on the right side of his neck. No other skin lesions are noted. The patient is afebrile. What is the most likely cause of the abscess? 1- Highly drug-resistant Pseudomonas aeruginosa 2- Extremely drug-resistant Mycobacterium tuberculosis 3- Vancomycin-resistant Enterococcus faecium 4- Penicillin-resistant Clostridium perfringens 5- Methicillin-resistant Staphylococcus aureus
Community-acquired Methicillin-resistant Staphylococcus aureus : An Emerging Pathogen in Orthopaedics J Am Acad Orthop Surg Marcotte and Trzeciak 16 (2): 98. 2008 See dirty rednecks from Colleton and call room showers. See JB
28.
Question #: 262Which of the following conditions is a contraindication to the use of most bisphosphonates? 1- Paget’s disease 2- Osteomyelitis 3- Bone infarct 4- Myasthenia gravis 5- Severe renal insufficiency/failure
29.
Preferred Response: 5Approximately 50% to 80% of disphosphanates are cleared from the blood stream by renal excretion , and approx 1% through biliary excretion Remainder of the drug is incorporated into the crystalline structure of bone and may persist for the lifetime of the patient, with an estimated half-life in bone of 10 years. Risks: Osteonecrosis of Jaw, Subtroch fractures (look for this one on upcoming tests! The orthopaedic implications of diphosphonate therapy. Weaver MJ , Miller MA , Vrahas MS . J Am Acad Orthop Surg . 2010 Jun;18(6):317-8.
30.
Question #: 275Osteoclasts are the primary cells involved in bone resorption. What is one of the most critical factors for osteoclast differentiation and activation? 1- PTH 2- BMP2 3- RANKL 4- Calcitonin 5- TNF-alpha
Question #: 59Paget’s disease of bone is associated with abnormal function of which of the following cell types? 1- Osteoblasts 2- Osteoclasts 3- Osteocytes 4- Histiocytes 5- Megakarocytes
34.
Preferred Response: 2Histology: - demonstrates excess osteoclasts resorptive activity; (occurs predominantly in the early resorptive phase); - bone marrow is replaced by fibrous tissue and disorganized trabeculae; - paratrabecular fibrosis; - irregular - highly celluar lamellar bone w/ irregular cement lines; - woven bone with osteoblastic rimming; - occasional prominent cement lines. Radiographs: - aggressive bone resorption; - lytic lesions w/ sharp borders that destroy the cortex; - new bone formation and sclerosis which causes thickening of the cortex and course trabeculae; - cortices will appear thickened and trabeculae will appear coarse; Labs – increased alk phos, increase urine and serum hydroxyproline Treament – bisphosphonates, calcitonin prior to elective surgery
35.
Question #: 116Which of the following postoperative modalities to prevent deep venous thrombosis is associated with the highest risk of hematoma? 1- Aspirin 2- Dipyridamole 3- Compression device 4- Clopidogrel bisulfate 5- Low-molecular-weight heparin
36.
Question #: 116Which of the following postoperative modalities to prevent deep venous thrombosis is associated with the highest risk of hematoma? 1- Aspirin 2- Dipyridamole 3- Compression device 4- Clopidogrel bisulfate 5- Low-molecular-weight heparin
37.
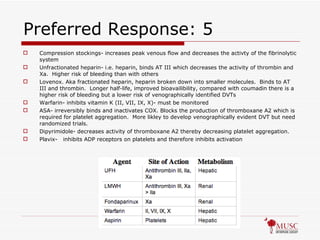
Preferred Response: 5Compression stockings- increases peak venous flow and decreases the activty of the fibrinolytic system Unfractionated heparin- i.e. heparin, binds AT III which decreases the activity of thrombin and Xa. Higher risk of bleeding than with others Lovenox. Aka fractionated heparin, heparin broken down into smaller molecules. Binds to AT III and thrombin. Longer half-life, improved bioavailibility, compared with coumadin there is a higher risk of bleeding but a lower risk of venographically identified DVTs Warfarin- inhibits vitamin K (II, VII, IX, X)- must be monitored ASA- irreversibly binds and inactivates COX. Blocks the production of thromboxane A2 which is required for platelet aggregation. More likley to develop venographically evident DVT but need randomized trials. Dipyrimidole- decreases activity of thromboxane A2 thereby decreasing platelet aggregation. Plavix- inhibits ADP receptors on platelets and therefore inhibits activation
38.
39.
Question #: 131In the case of a mother (who is a carrier for Duchenne’s muscular dystrophy gene) and a father (who does not have the Duchenne’s muscular dystrophy gene), what is the chance that the son will be affected by Duchenne’s muscular dystrophy? 1- 25% 2- 50% 3- 75% 4- 100% 5- Unable to determine since the father may be a carrier.
40.
Question #: 131In the case of a mother (who is a carrier for Duchenne’s muscular dystrophy gene) and a father (who does not have the Duchenne’s muscular dystrophy gene), what is the chance that the son will be affected by Duchenne’s muscular dystrophy? 1- 25% 2- 50% 3- 75% 4- 100% 5- Unable to determine since the father may be a carrier.
41.
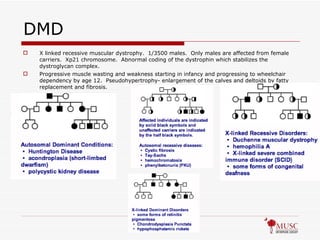
DMD X linkedrecessive muscular dystrophy. 1/3500 males. Only males are affected from female carriers. Xp21 chromosome. Abnormal coding of the dystrophin which stabilizes the dystroglycan complex. Progressive muscle wasting and weakness starting in infancy and progressing to wheelchair dependency by age 12. Pseudohypertrophy- enlargement of the calves and deltoids by fatty replacement and fibrosis.
42.
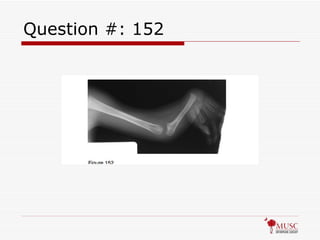
Question #: 152A newborn infant is brought to the office with the features shown in Figure 152. Many children with this condition have multiple systemic anomalies. Which of the following body sites is most likely to have associated abnormalities? 1- Vertebral complex 2- Renal system 3- Cardiac system 4- Hematopoetic system 5- Central nervous system
Question #: 152A newborn infant is brought to the office with the features shown in Figure 152. Many children with this condition have multiple systemic anomalies. Which of the following body sites is most likely to have associated abnormalities? 1- Vertebral complex 2- Renal system 3- Cardiac system 4- Hematopoetic system 5- Central nervous system
45.
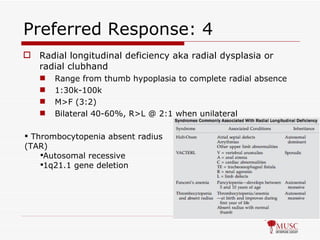
Preferred Response: 4Radial longitudinal deficiency aka radial dysplasia or radial clubhand Range from thumb hypoplasia to complete radial absence 1:30k-100k M>F (3:2) Bilateral 40-60%, R>L @ 2:1 when unilateral Thrombocytopenia absent radius (TAR) Autosomal recessive 1q21.1 gene deletion
46.
Question #: 179Rheumatoid factors are antibodies directed against 1- multiple immunoglobulins. 2- IgA. 3- IgE. 4- IgM. 5- IgG.
47.
Question #: 179Rheumatoid factors are antibodies directed against 1- multiple immunoglobulins. 2- IgA. 3- IgE. 4- IgM. 5- IgG.
48.
Preferred Response: 5RF is an IgM antibody directed against the Fc portion of the patient’s own IgG Purpose of RF is unknown but though to help clear immune complexes through stabilization and opsinization RF is commonly secreted during acute infections and probably is part of the normal immune response RF is present in 70% to 90% of patients with RA; a negative RF result does not rule out rheumatoid arthritis. Sensitive but not specific. RF may take several months to appear in the serum after arthritis develops. The level of RF is prognostic, that is, the higher the level, the worse the prognosis.
49.
Question #: 274Disease modifying antirheumatic drug therapy such as infliximab is primarily targeted against 1- leukocytes. 2- rheumatoid factor. 3- antinuclear antibodies. 4- C-reactive protein. 5- tumor necrosis factor-alpha.
50.
Preferred Response: 5 (TNF-alpha) Rheumatoid Arthritis : 90% positive for RF Morning stiffness, pain, joint swelling, hand deformities such as subluxation, ulnar drift, swan-neck deformity Periarticular osteopenia Juxta-articular erosion Joint space narrowing Treatment NSAIDS, Aspirin Disease-modifying antirheumatic drugs Methotrexate (inhibits dihydrofolate reductase and folate metabolism, is current treatment choice) Cytokine-neutralizing Etanercept (soluble p75 TNF receptor immunoglobulin G fusion protein) Infliximab (chimeric monoclonal antibody to TNf-alpha) Rituximab (monoclonal antibody to CD20 antigen;inhibits B-cells) From COR Book
![Preferred Response: 4 Type I hypersensitivity is mediated by IgE , which triggers degranulation of mast cells and basophils when cross-linked by antigen. [74] Type II hypersensitivity occurs when antibodies bind to antigens on the patient's own cells, marking them for destruction. This is also called antibody-dependent (or cytotoxic) hypersensitivity, and is mediated by IgG and IgM antibodies. [74] Type III hypersensitivity reactions- Immune complexes (aggregations of antigens, complement proteins, and IgG and IgM antibodies) deposited in various tissues trigger. [74] Type IV hypersensitivity (also known as cell-mediated or delayed type hypersensitivity ) usually takes between two and three days to develop. Type IV reactions are involved in many autoimmune and infectious diseases, but may also involve contact dermatitis ( poison ivy ). These reactions are mediated by T cells , monocytes , and macrophages A routine skin test reveals a prevalence of metal sensitivity of 0.2% for chromium, 1.3% for nickel, and 1.8% for cobalt. After placement of metal implants, sensitization (change from negative to positive) occurs in 2.7% for chromium, 3.8% for nickel, and 3.8% for cobalt. Desensitization (change from positive to negative) occurs in 0% for chromium, 2.1% for nickel, and 3.8% for cobalt. Many patients with implanted metal hardware have positive skin test results for those metals but are completely asymptomatic Type I hypersensitivity to latex involves IgE antibodies that are specific for proteins from the sap of the rubber tree (Hevea brasiliensis) used to make gloves Wiki/emedicine](https://image.slidesharecdn.com/oite9-14-2010-110419082802-phpapp01/85/Oite-9-14-2010-5-320.jpg)






























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















