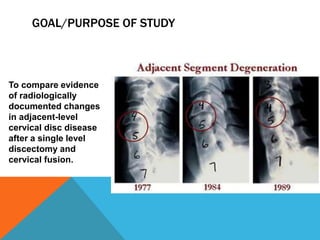
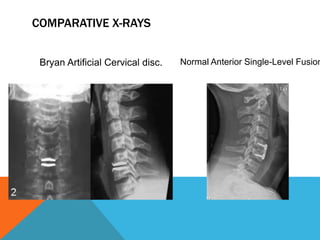
This study compared outcomes of 103 patients who received the Bryan artificial cervical disc replacement to 158 patients who received cervical fusion with the Affinity cervical cage system. Patients were examined at 24 months post-operation. The study found higher rates of new osteophyte formation, disc narrowing, and symptomatic adjacent segment disease in patients who received cervical fusion compared to those who received the artificial disc. Specifically, cervical fusion was associated with a 34.6% rate of new radiographic changes compared to 17.5% for artificial discs. The study concludes that preserving motion with an artificial disc may delay or prevent symptomatic adjacent segment disease compared to fusion.