Downloaded 1,094 times










































![Impact of Enteral nutrition on outcome
▪ A recently published systematic analysis reviewed data from 13 randomized controlled studies
comparing EN and PN in heterogeneous populations of ICU patients, including those with head
trauma, sepsis, and severe acute pancreatitis, among other conditions. When a meta-analysis was
carried out, there was no apparent difference in mortality rate between patients treated with EN
and those treated with PN (relative risk [RR] 1.08; 95% confidence interval [CI], 0.70-1.65).
However, compared with PN, EN was associated with a significant reduction in infectious
complications.
▪ Eight randomized controlled trials that compared early EN with more delayed forms of nutrition
were recently reviewed and analysed. When these studies were aggregated, early EN was
associated reduced mortality (RR 0.52; 95% CI, 0.25-1.08) and fewer infectious complications
(RR 0.66; 95% CI, 0.36-1.22) compared with delayed nutrient intake. However, there were no
differences in complications between the groups.
▪ In a recent meta-analysis, there were seven randomized trials that evaluated the effect of route of
feeding on rates of ventilator-associated pneumonia. When these results were aggregated,
there was a significant reduction in ventilator associated pneumonia with feeding distal to
the pylorus (RR 0.76; 95% CI, 0.59-0.99). These studies also demonstrated that small-bowel
feeding is associated with an increase in protein and calories delivered and a shorter time to attain
the target dose of nutrition.](https://image.slidesharecdn.com/nutritioninicu-150426065528-conversion-gate01/75/Nutrition-in-icu-46-2048.jpg)





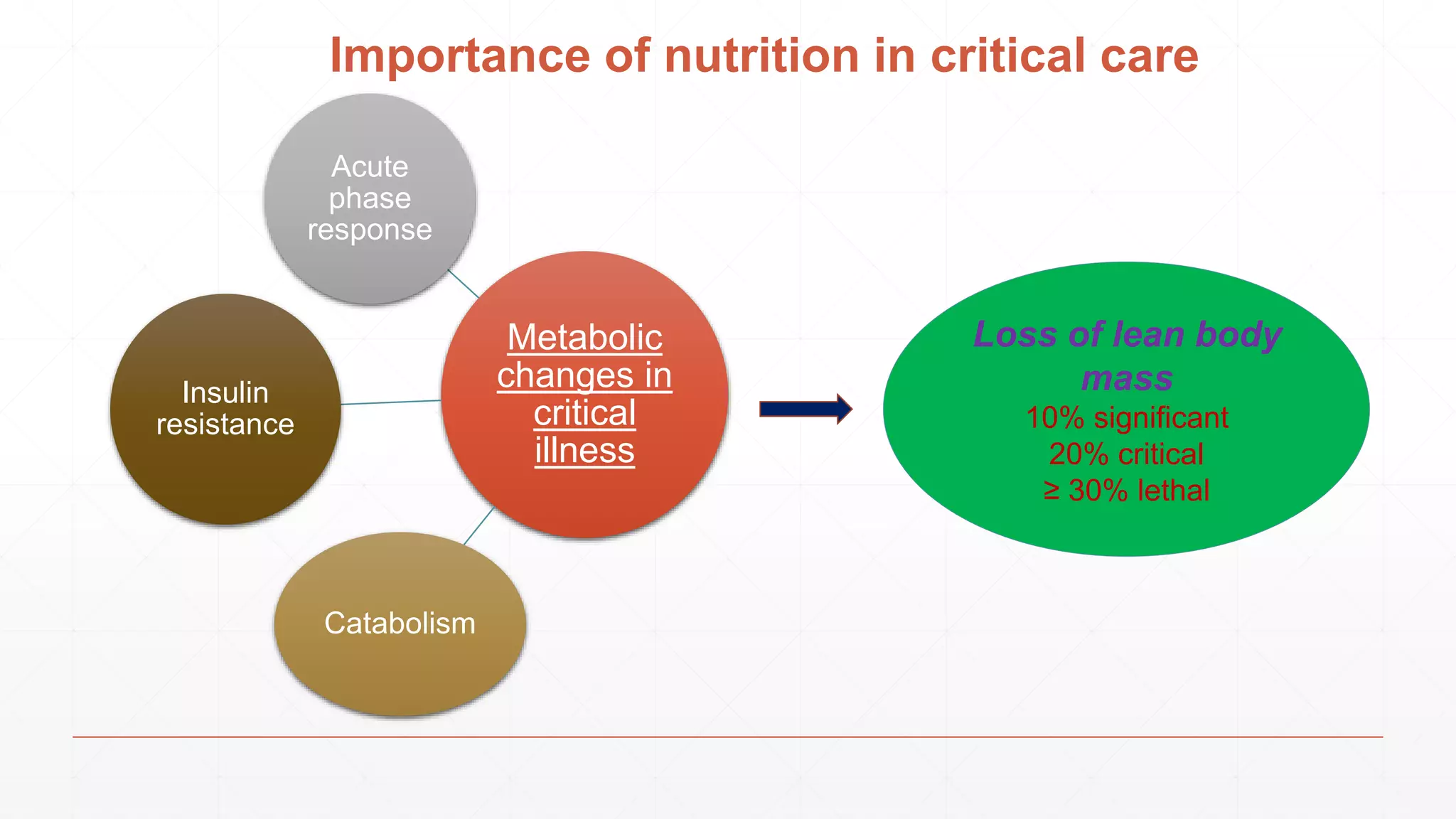
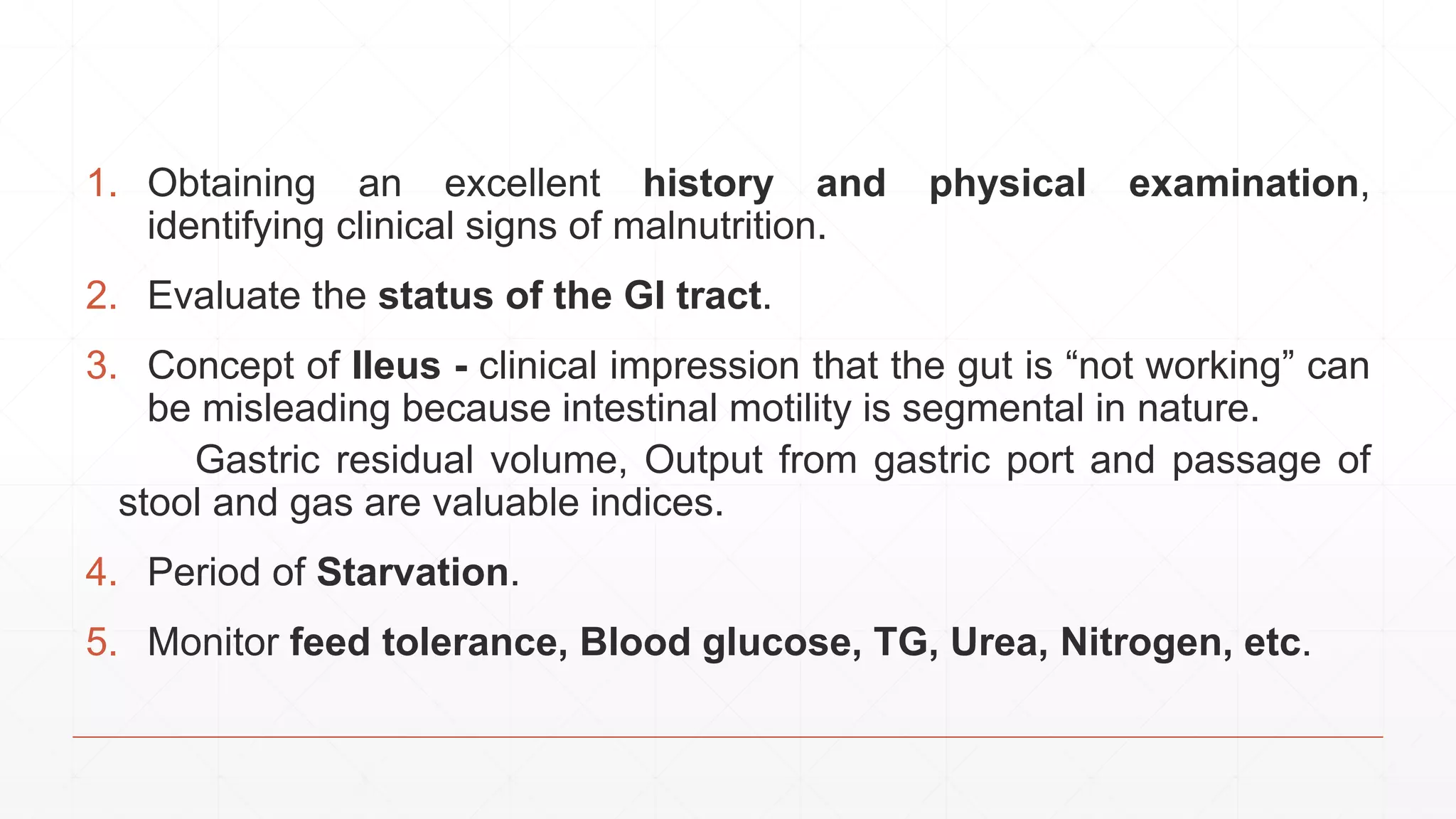
Nutritional support is essential for critically ill patients to combat malnutrition and preserve body mass, yet its efficacy varies based on individualized clinical factors. Early enteral feeding is now prioritized to improve patient outcomes, while assessing nutritional status remains challenging in the ICU. Parenteral nutrition is reserved for cases where enteral feeding fails, with careful monitoring needed to mitigate complications.




























































































