Downloaded 57 times

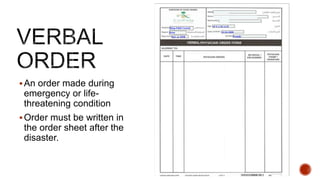
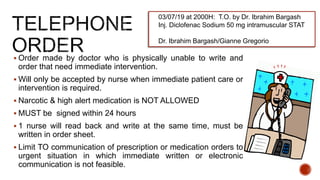

This document discusses nursing documentation policies and procedures. It covers the purposes of documentation which are to serve as communication between healthcare members, provide a permanent legal record, and ensure continuity of care. It also discusses different types of documentation like the problem-oriented charting format and flowsheets. The document provides guidance on documenting verbal/telephone orders, panic lab results, and handovers. It emphasizes adhering to hospital policies and procedures to maintain patient and staff safety.












![[1] documentation and reporting](https://cdn.slidesharecdn.com/ss_thumbnails/1documentationandreporting-150205213856-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)


































































