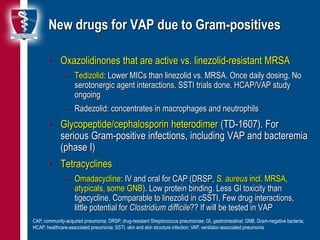
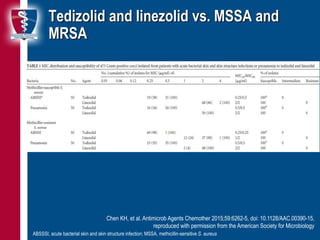
This document discusses new antibiotic developments for ventilator-associated pneumonia (VAP). It outlines several new drugs in development or approval that show promise for treating multi-drug resistant Gram-negative and Gram-positive pathogens commonly seen in VAP. These include novel beta-lactamase inhibitor combinations like ceftolozane-tazobactam and ceftazidime-avibactam, as well as other classes such as aminoglycosides and tetracyclines. Ongoing and completed clinical trials evaluating some of these new agents for the treatment of VAP are also summarized.