Downloaded 2,446 times

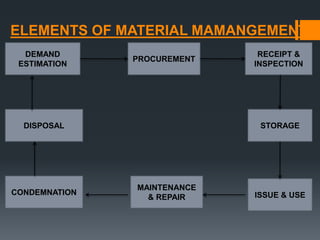


This document discusses material management in healthcare. It defines material management and lists its basic functions which include effective purchasing, inventory control, and distribution systems. The goals of material management are to have the right materials in the needed quantities and quality at the lowest possible price. Key aspects covered include demand forecasting, procurement, receipt and inspection of materials, storage, and issue and use of materials. Effective material management is important for delivering quality healthcare services on budget.







































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










