Downloaded 88 times

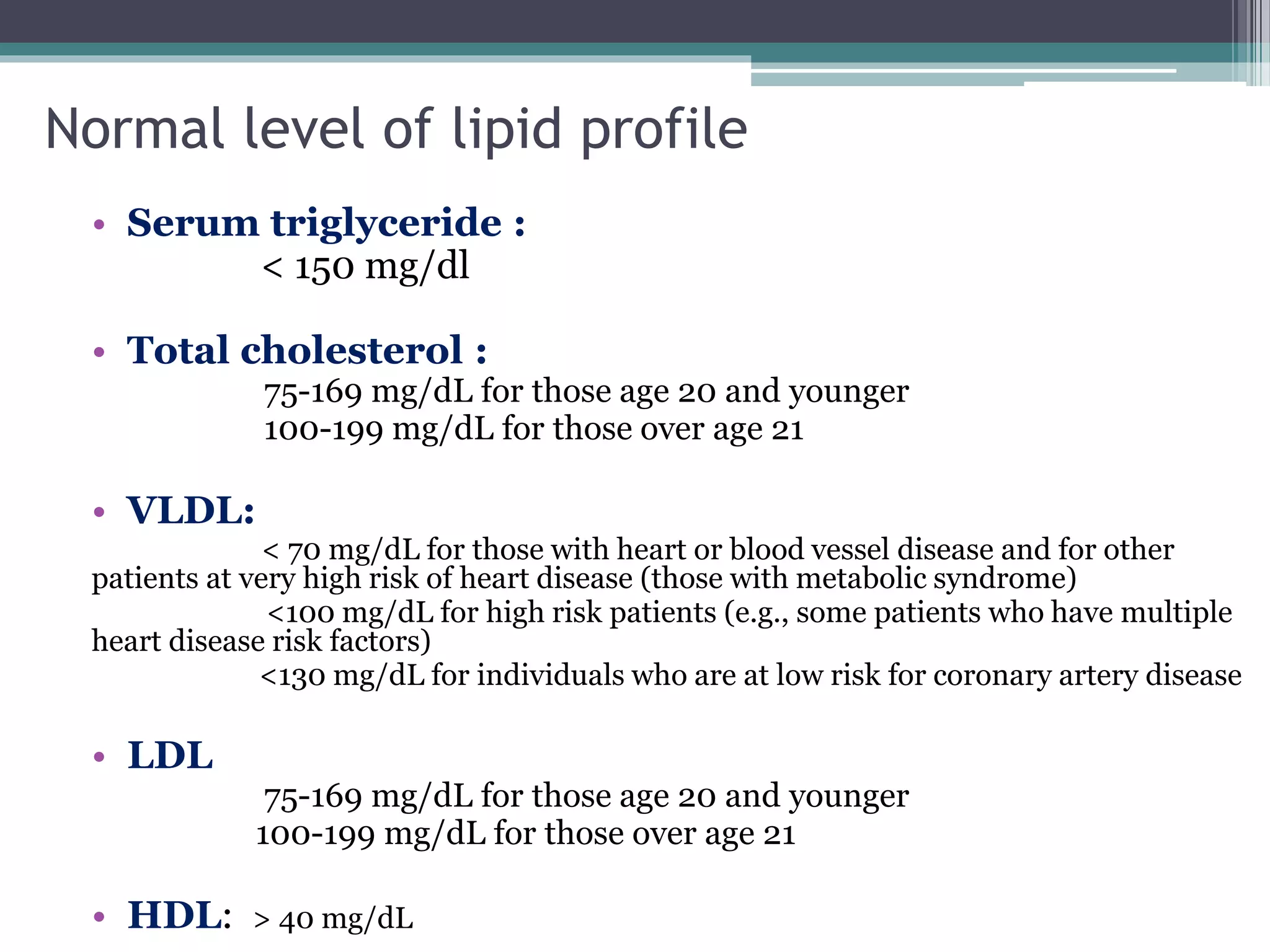
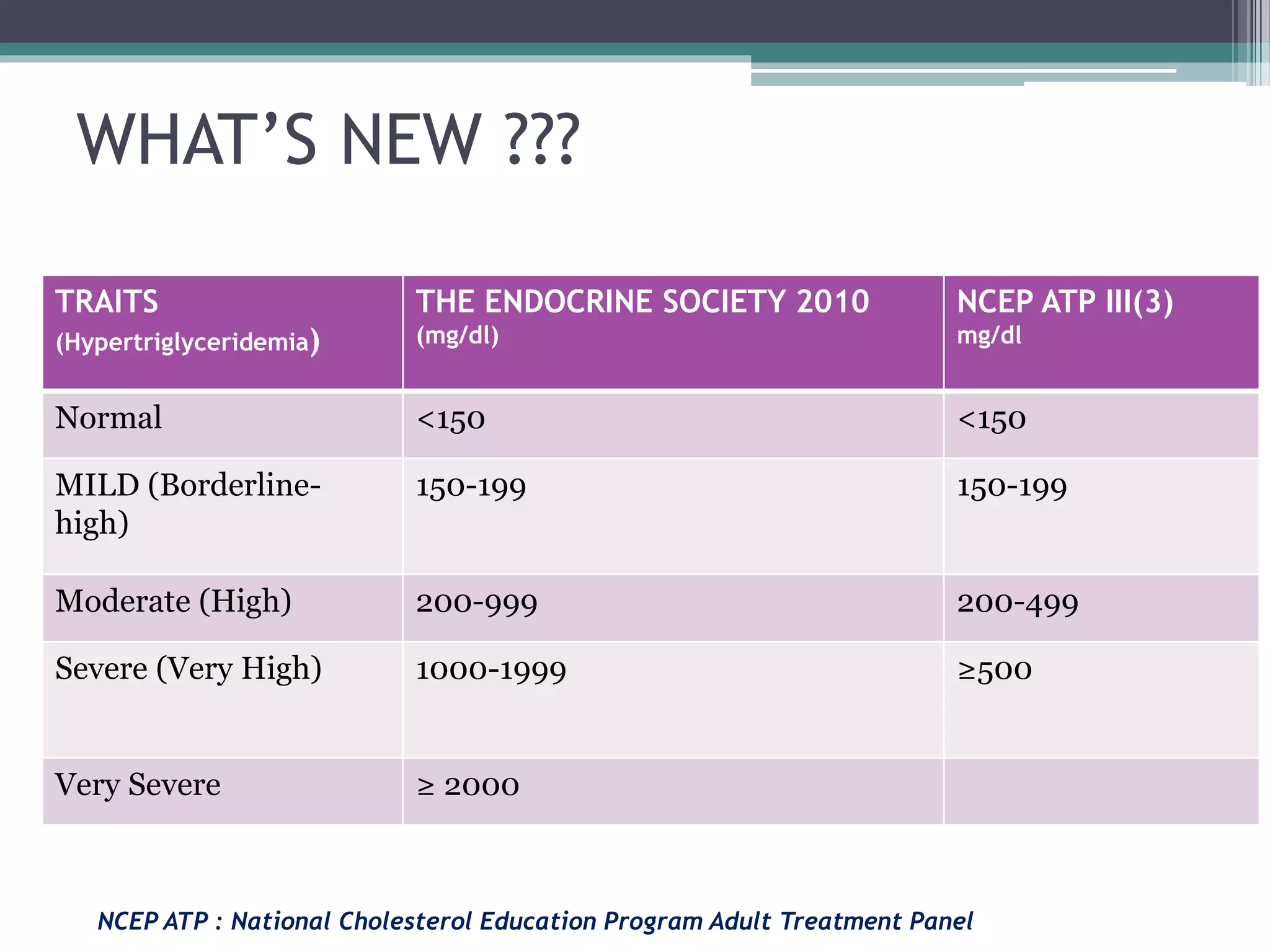
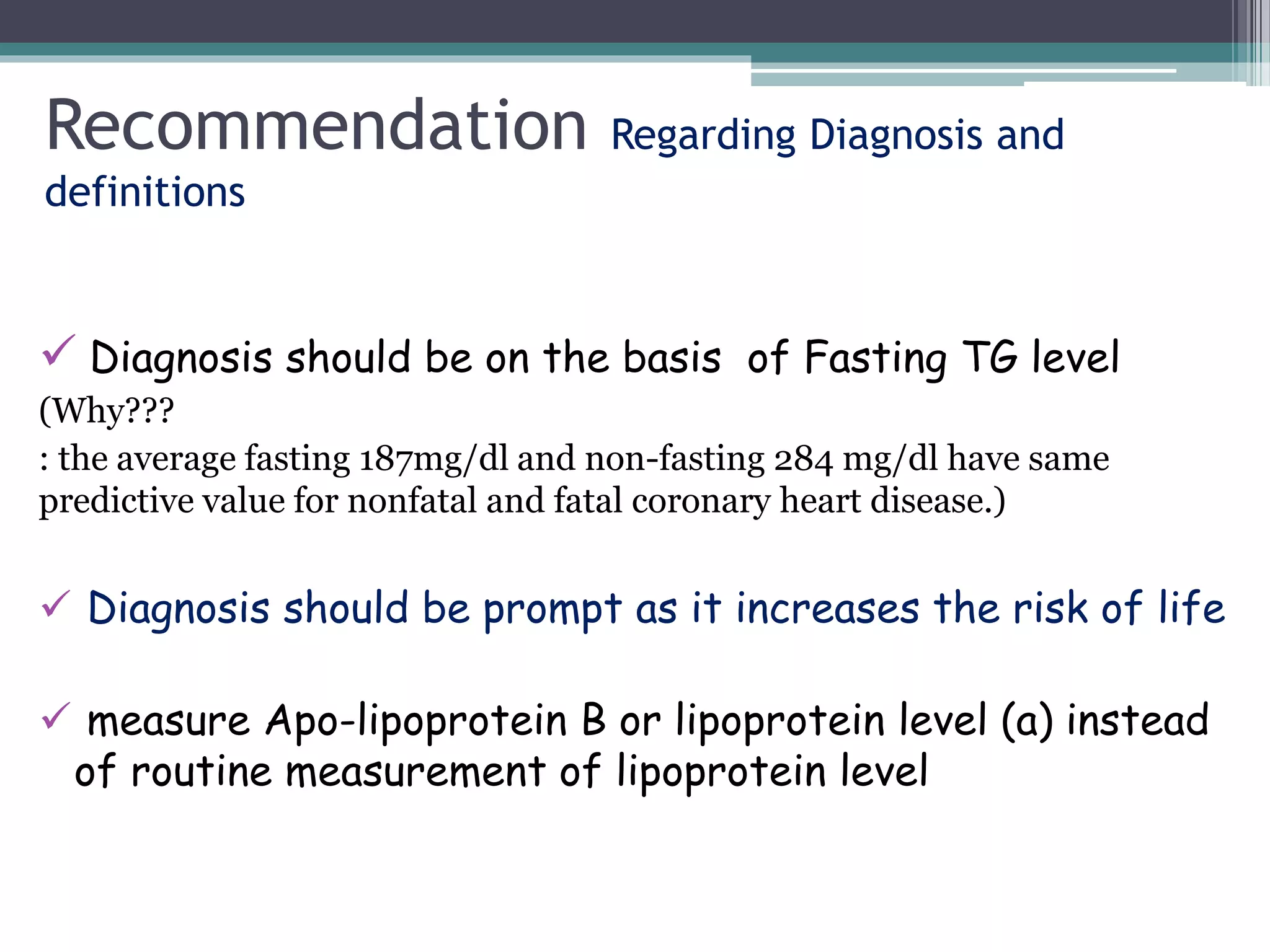
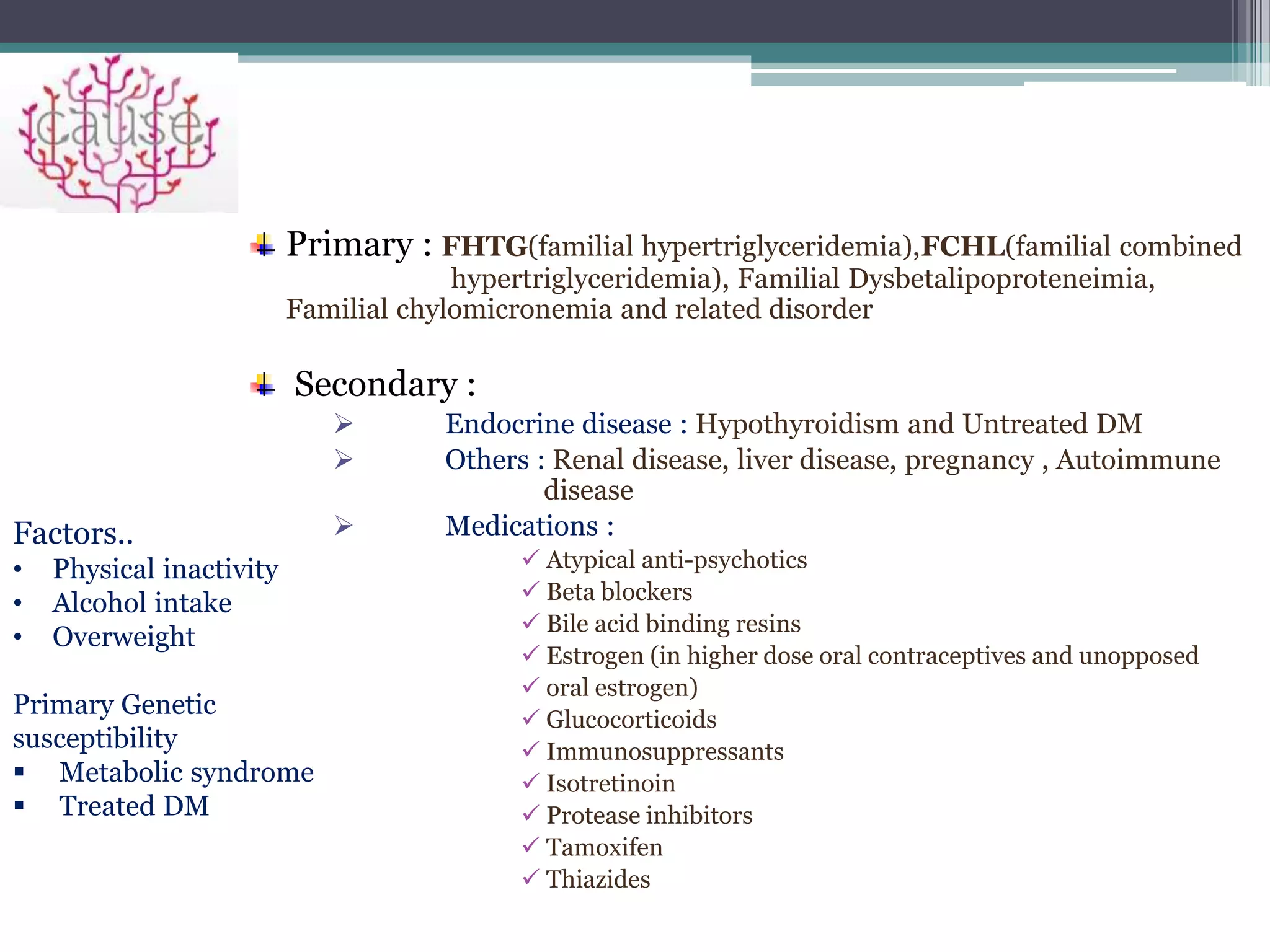
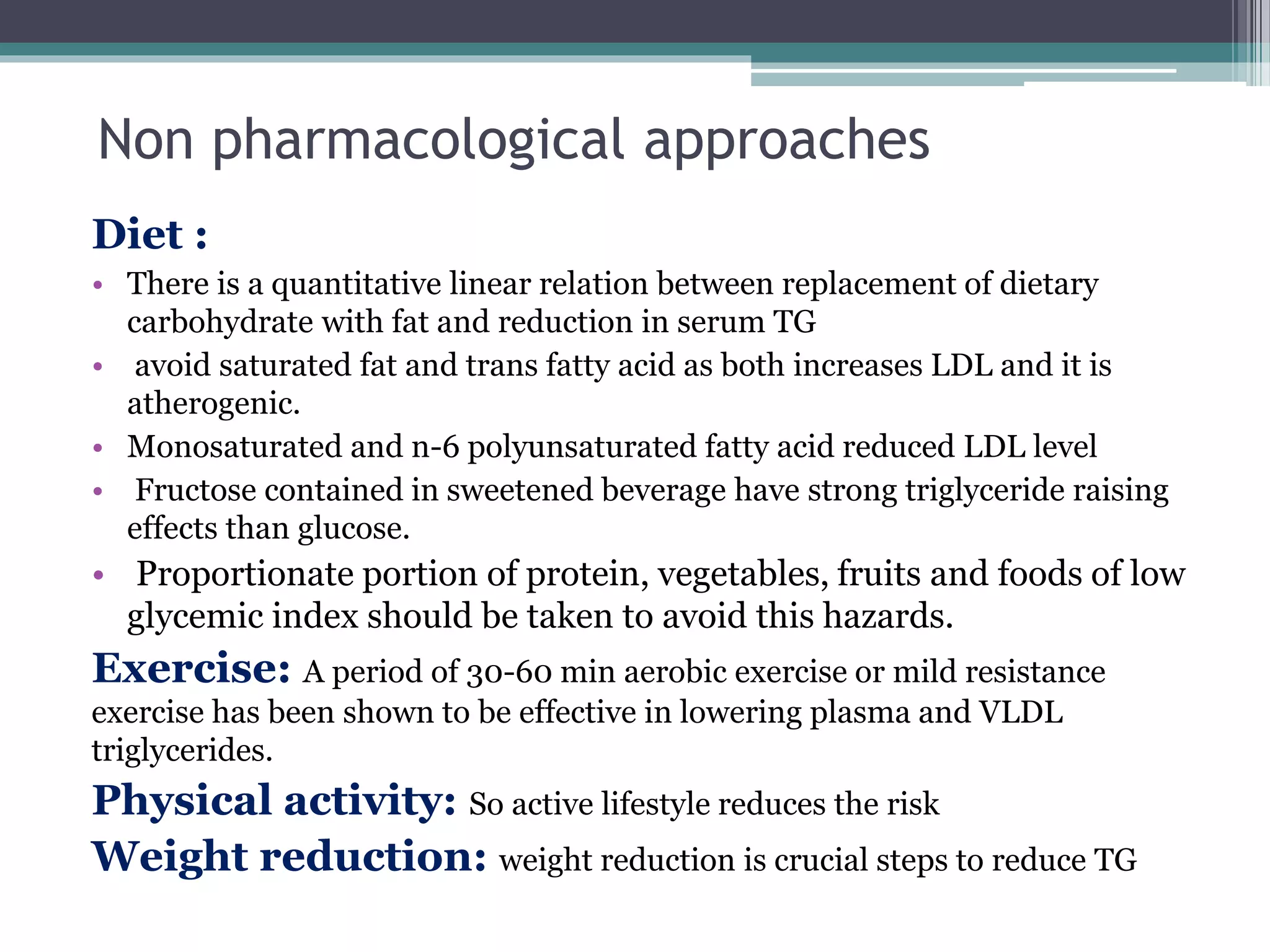
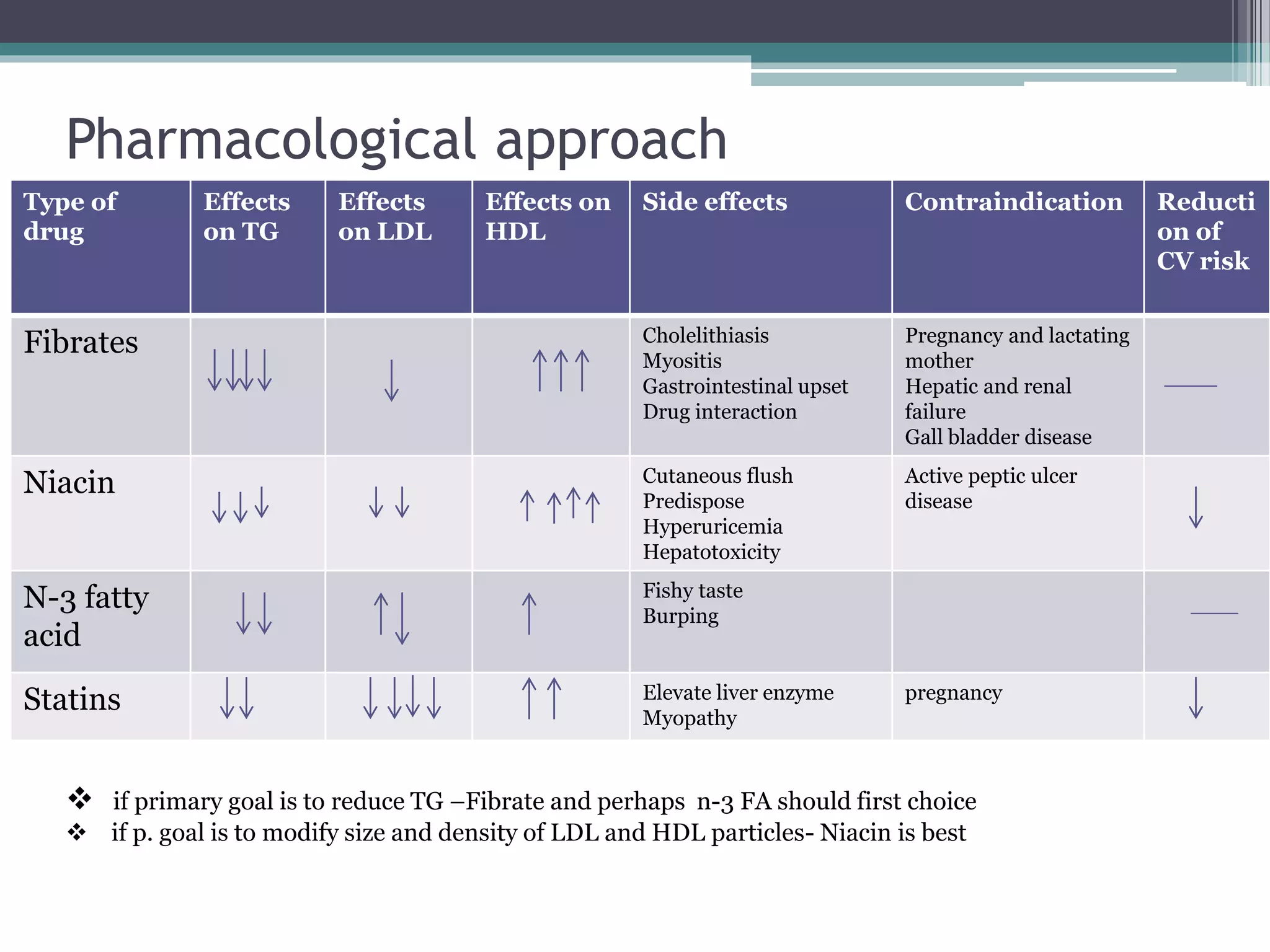



This document provides recommendations for the evaluation and treatment of hypertriglyceridemia. It defines normal triglyceride levels and categories of mild, moderate, severe and very severe hypertriglyceridemia. Primary causes include genetic factors while secondary causes include endocrine diseases, medications and lifestyle factors. Management involves addressing the underlying cause, lifestyle modifications like diet and exercise, and pharmacological treatment including fibrates, niacin, omega-3 fatty acids and statins depending on the severity of hypertriglyceridemia and cardiovascular risk factors. The goal is to lower triglyceride levels and cardiovascular risk through a combination of lifestyle and medical interventions.














































































