Downloaded 89 times
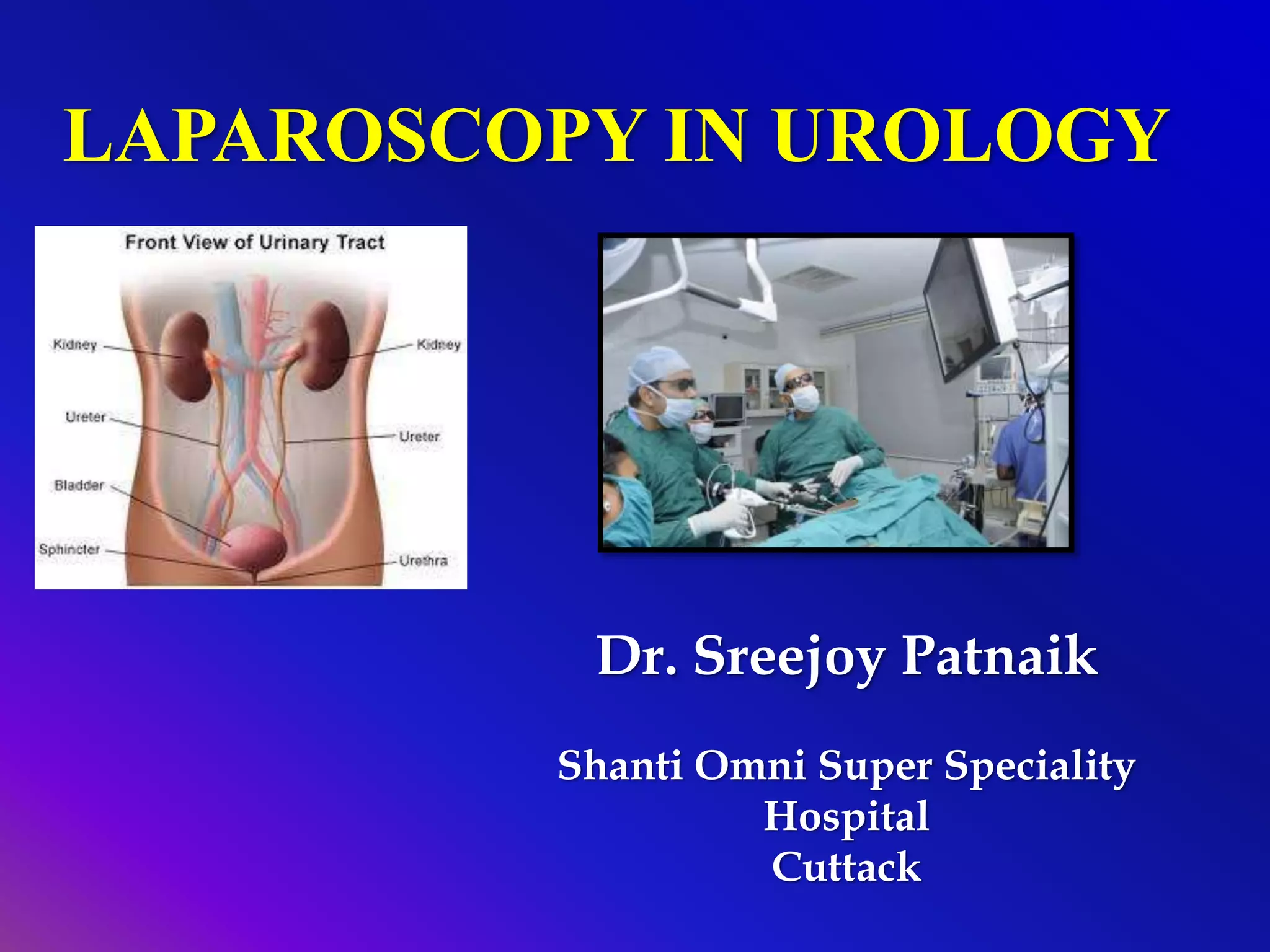
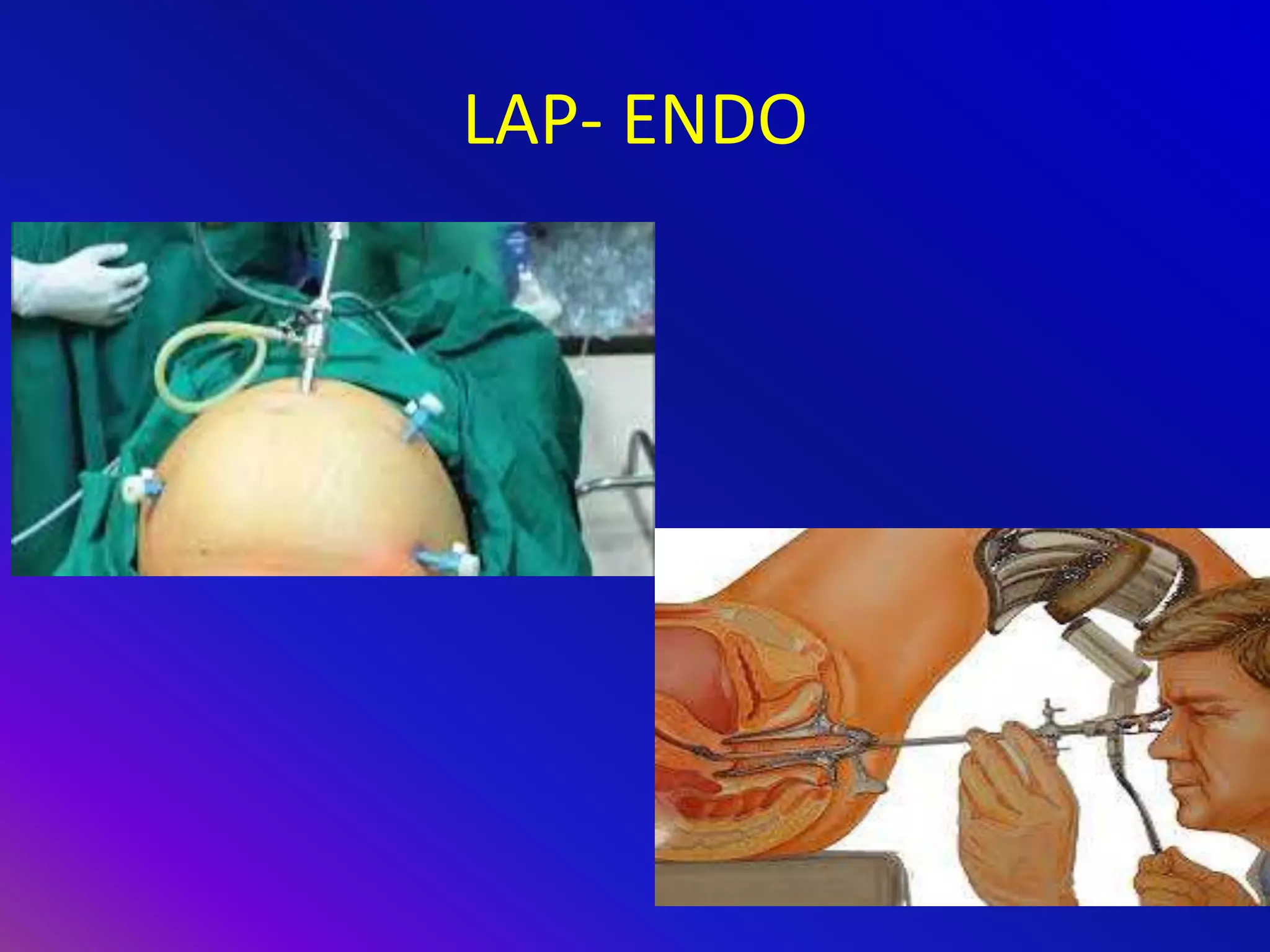


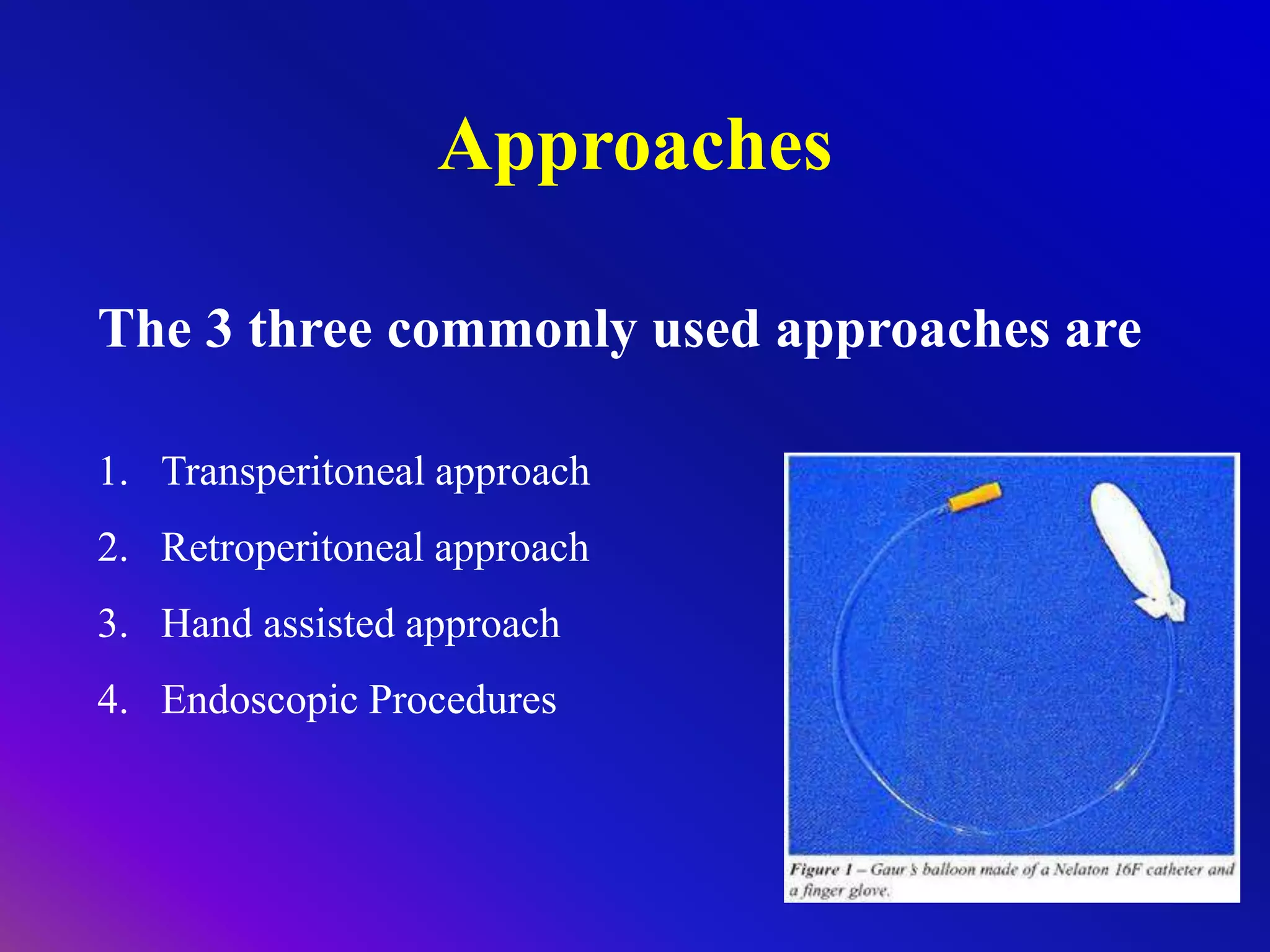

















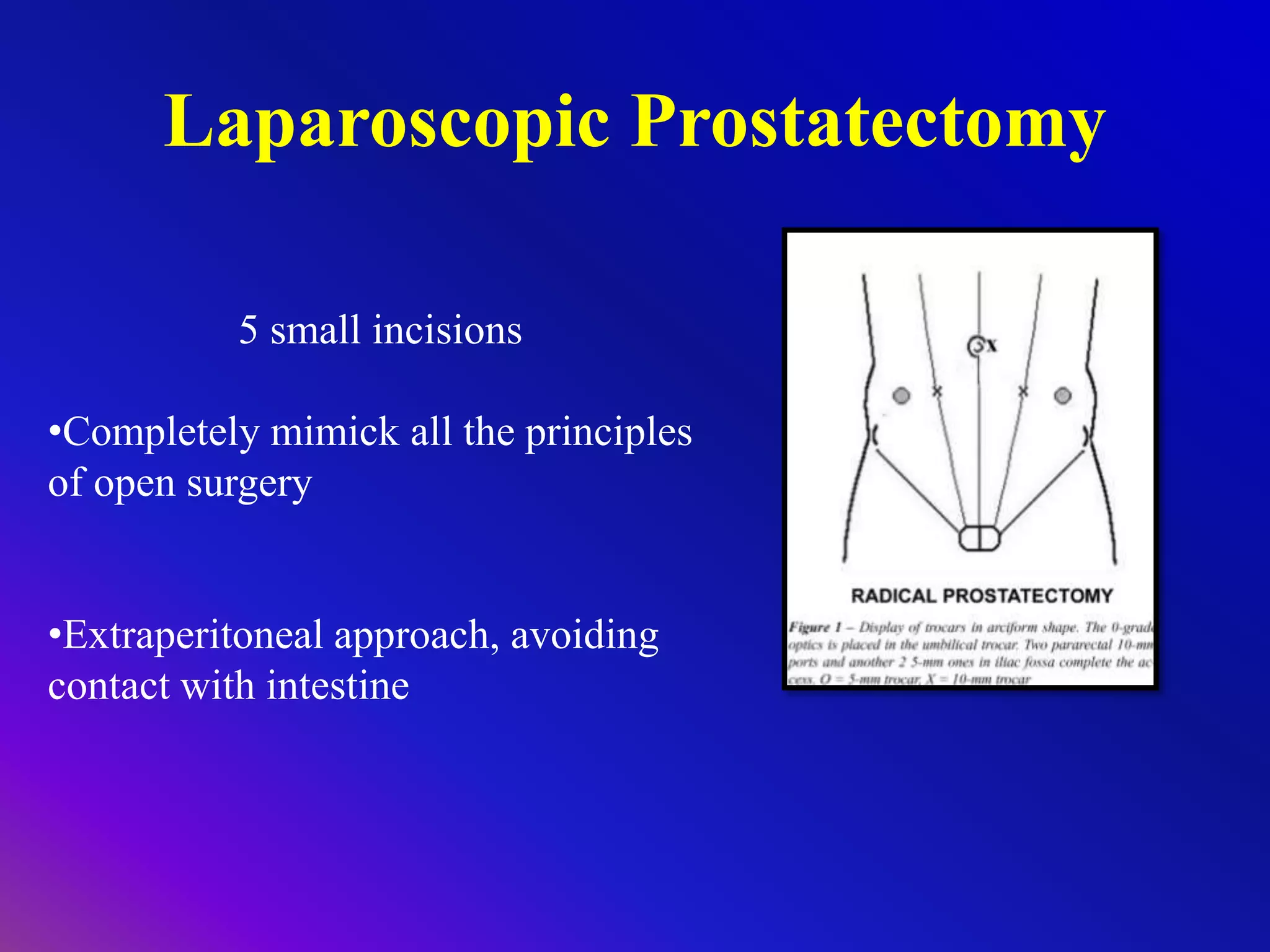




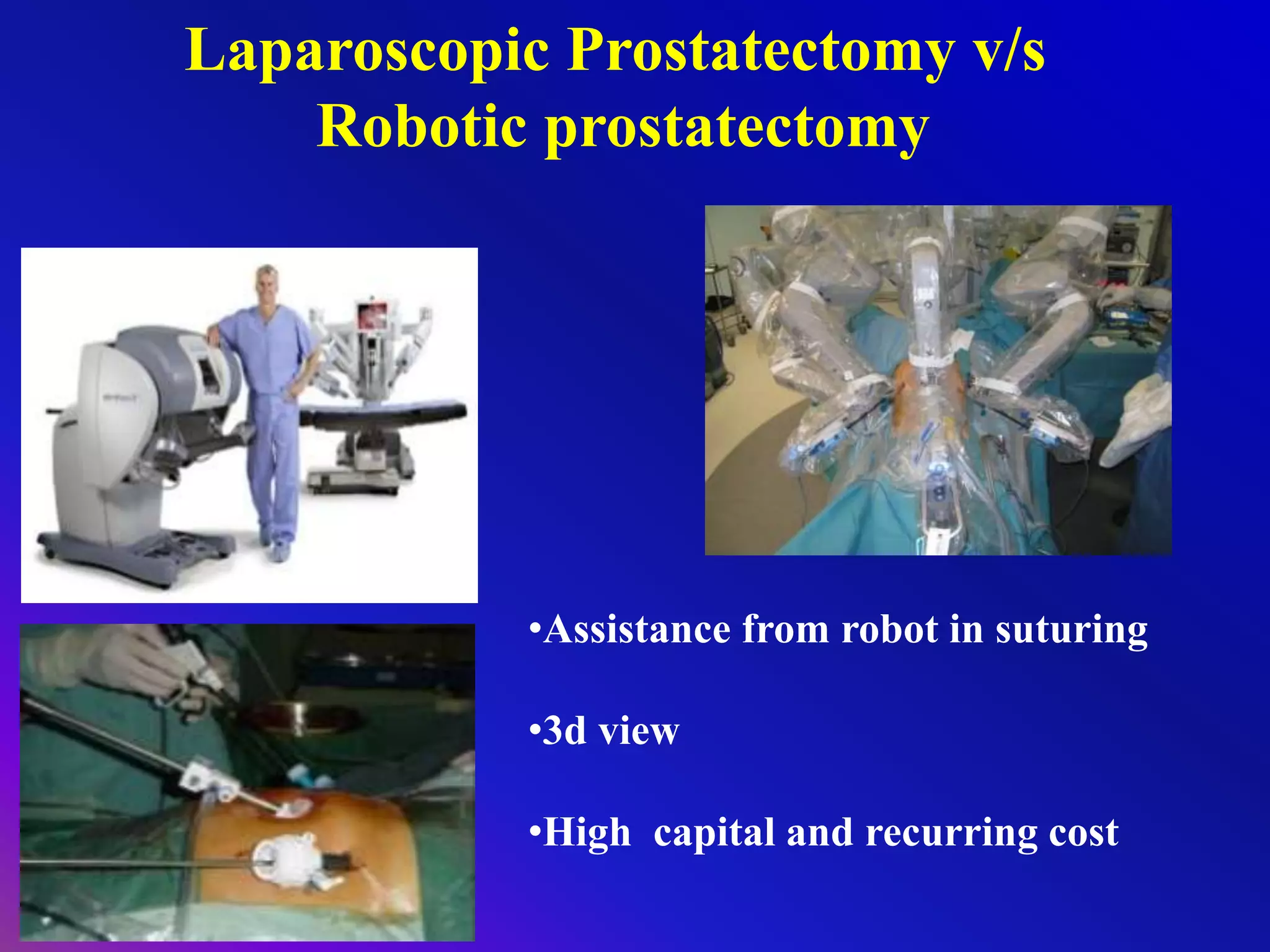

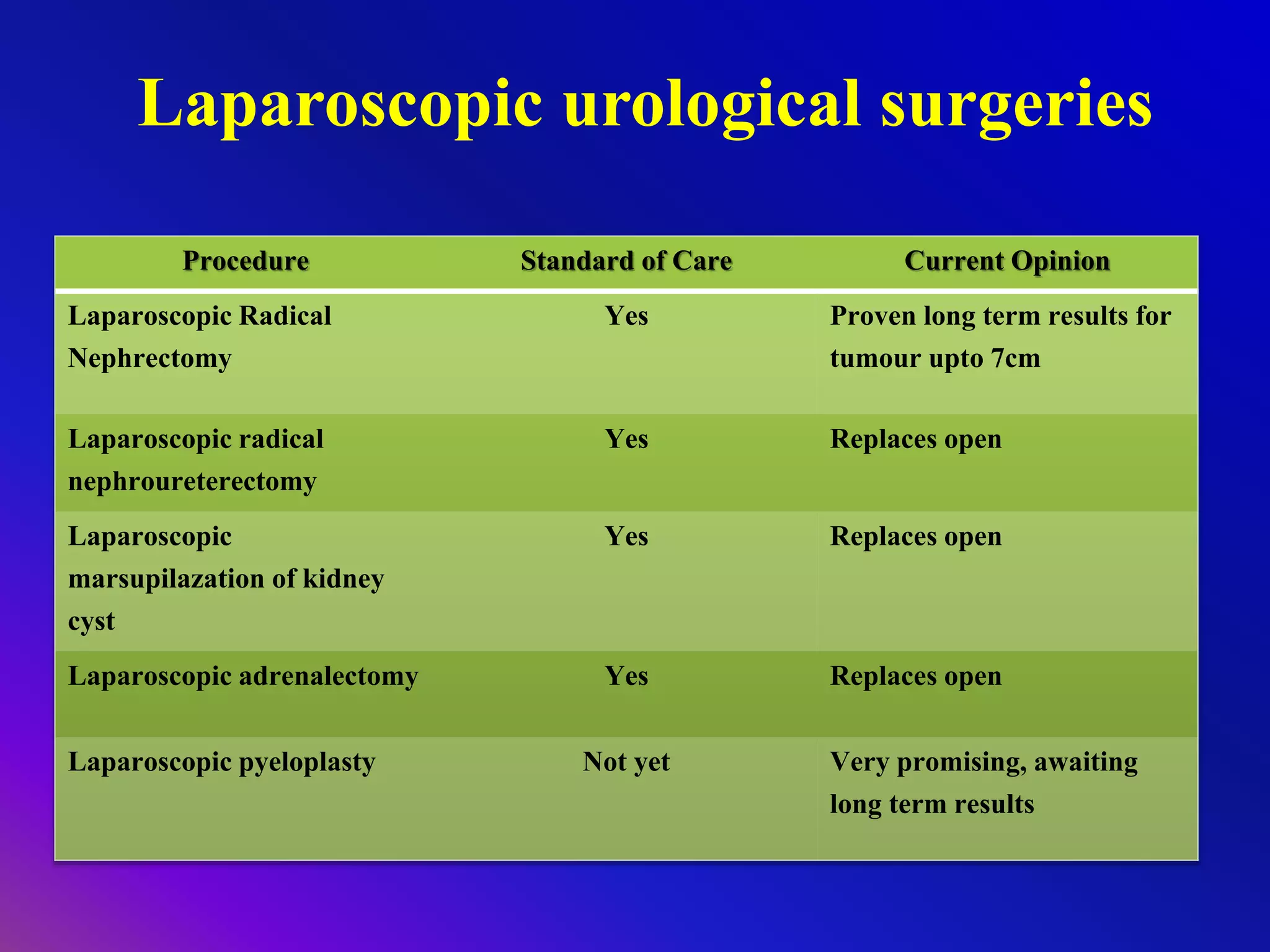
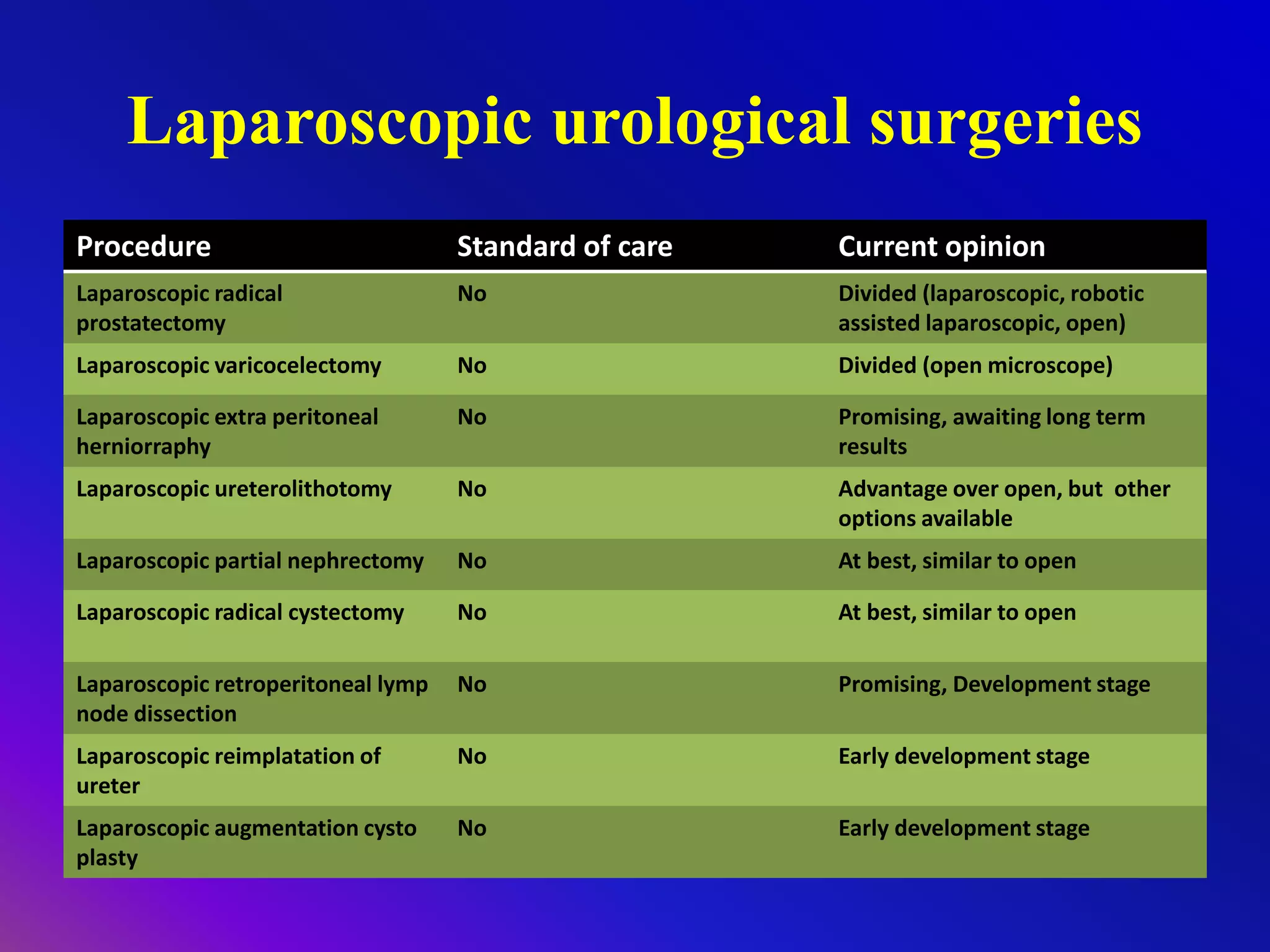


The document details the history and advancements of laparoscopic surgery in urology, highlighting its advantages over traditional open surgery, such as smaller wounds, reduced pain, and quicker recovery times. It discusses various laparoscopic techniques, common procedures, and approaches, such as transperitoneal and retroperitoneal techniques, along with the role of robotic assistance in enhancing surgical precision. The overall trend indicates a shift towards minimally invasive techniques in urology, with ongoing developments and varying opinions on specific procedures' standards of care.


































































































