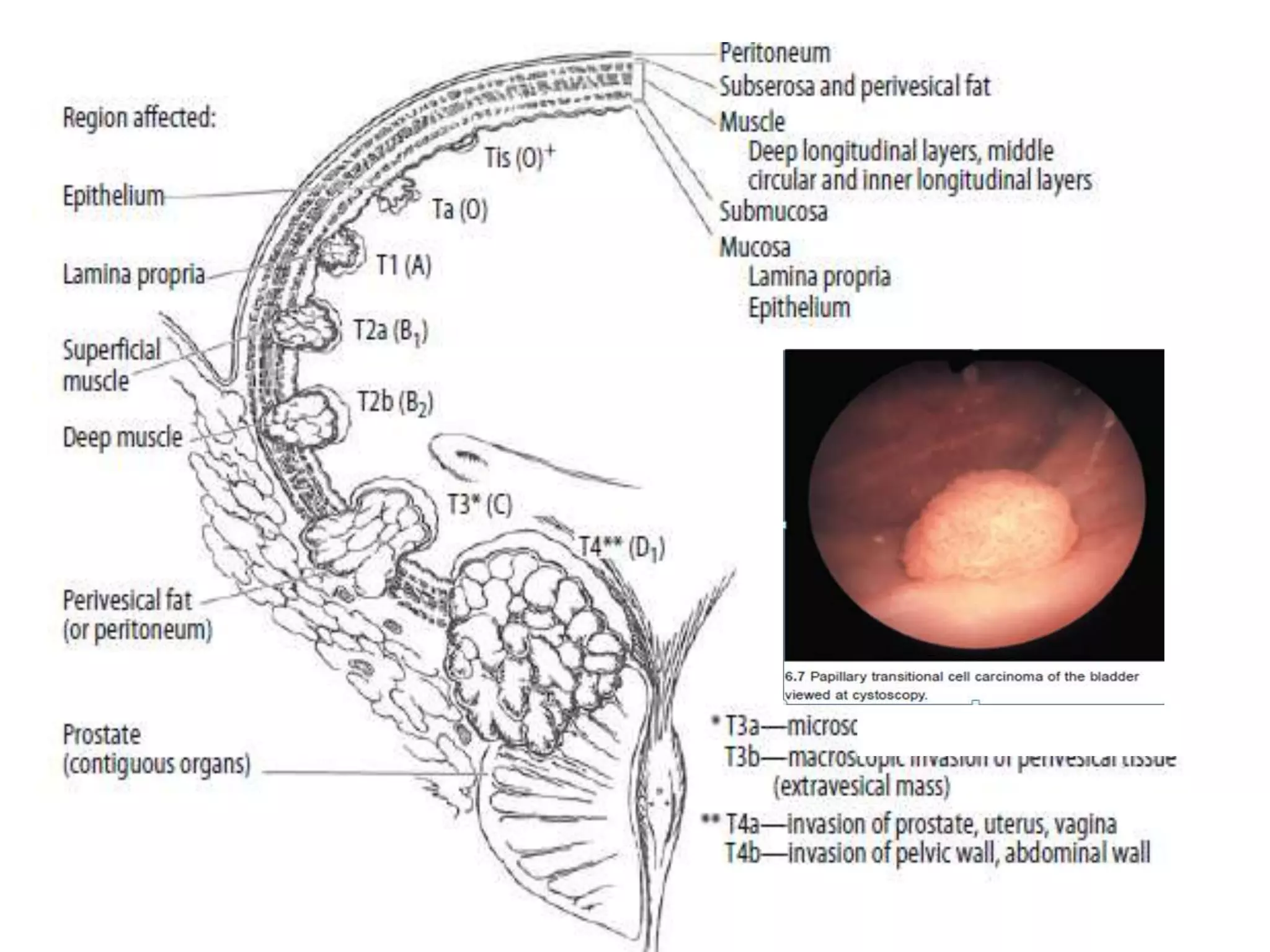
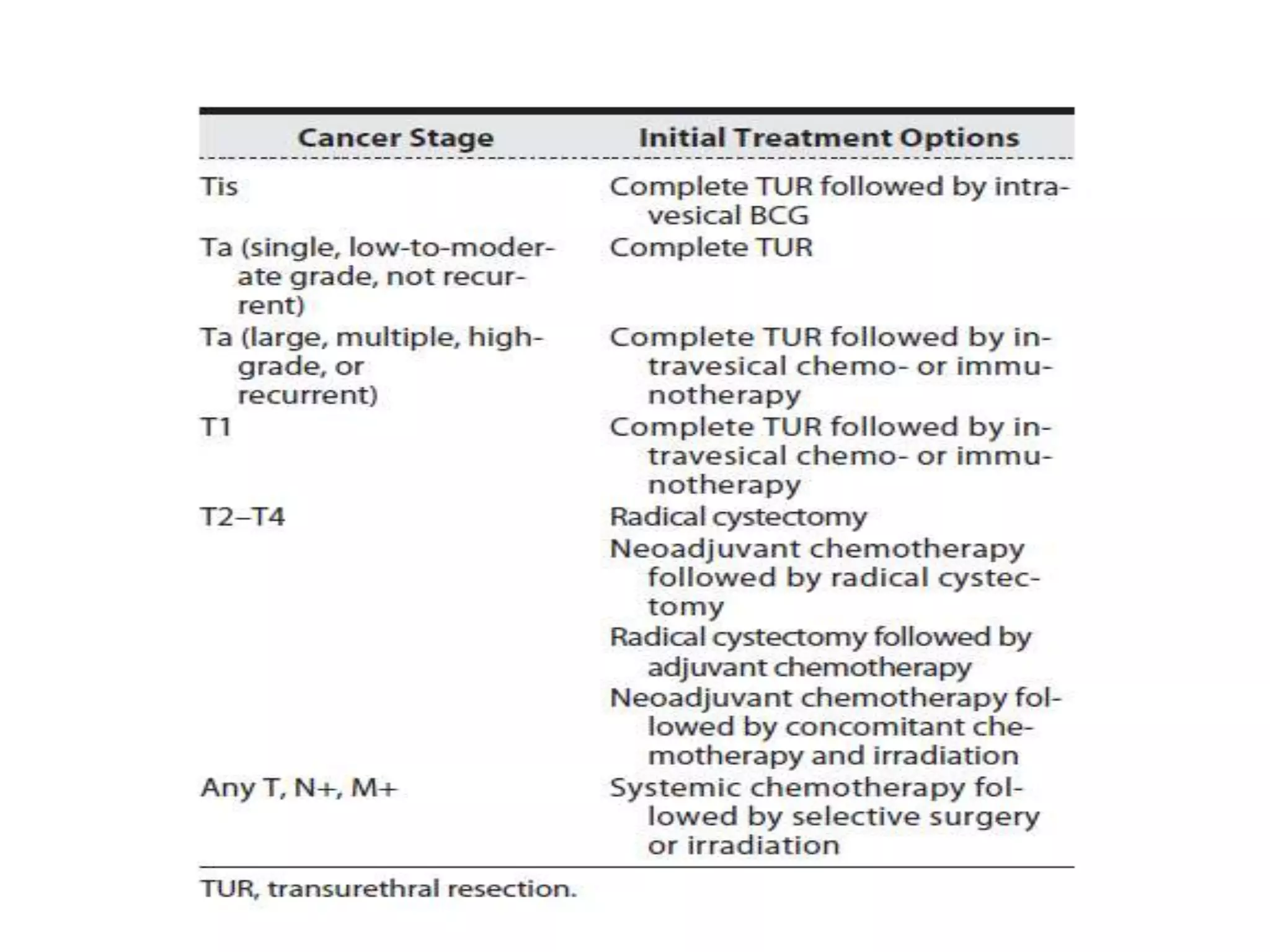
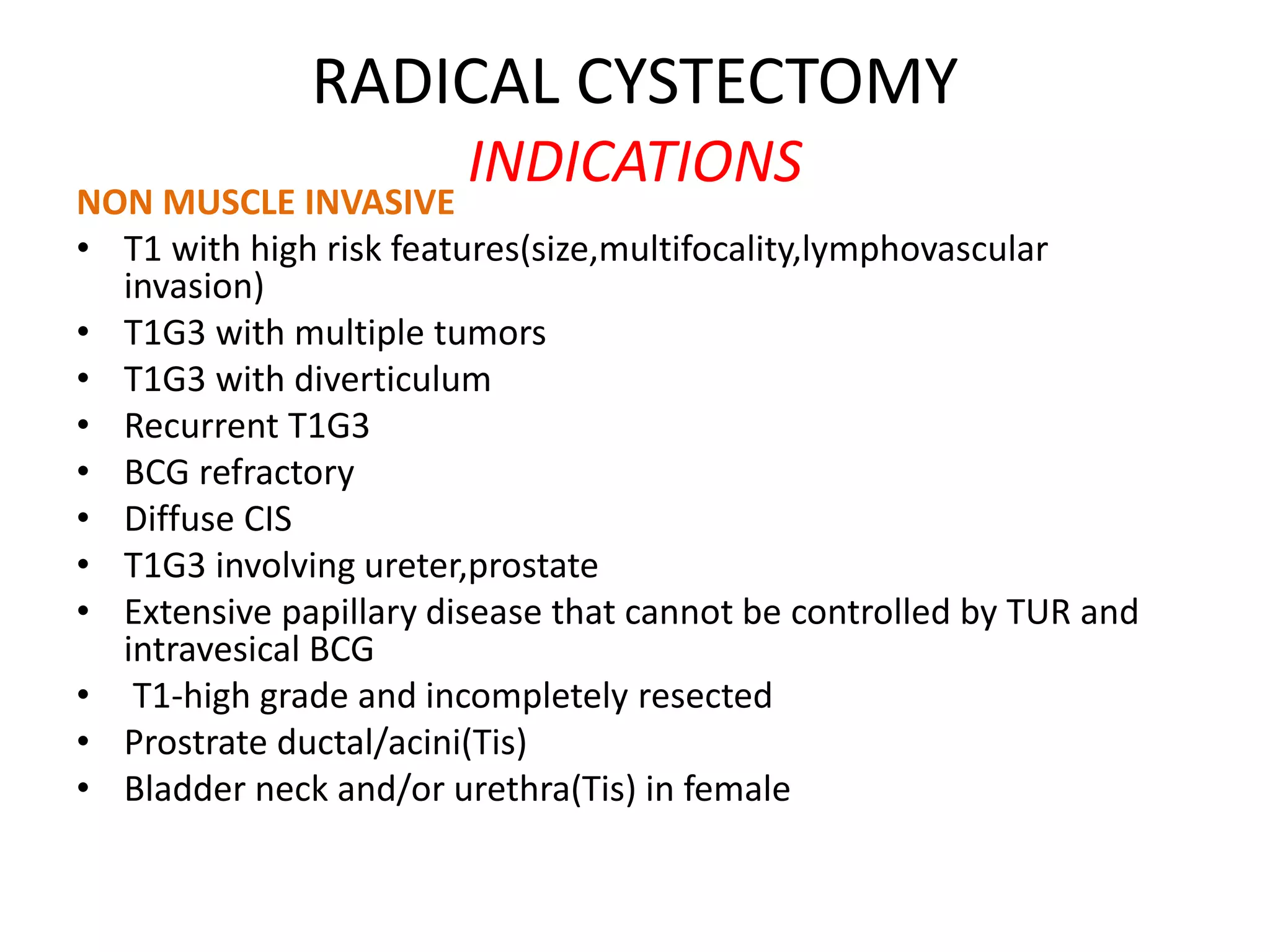
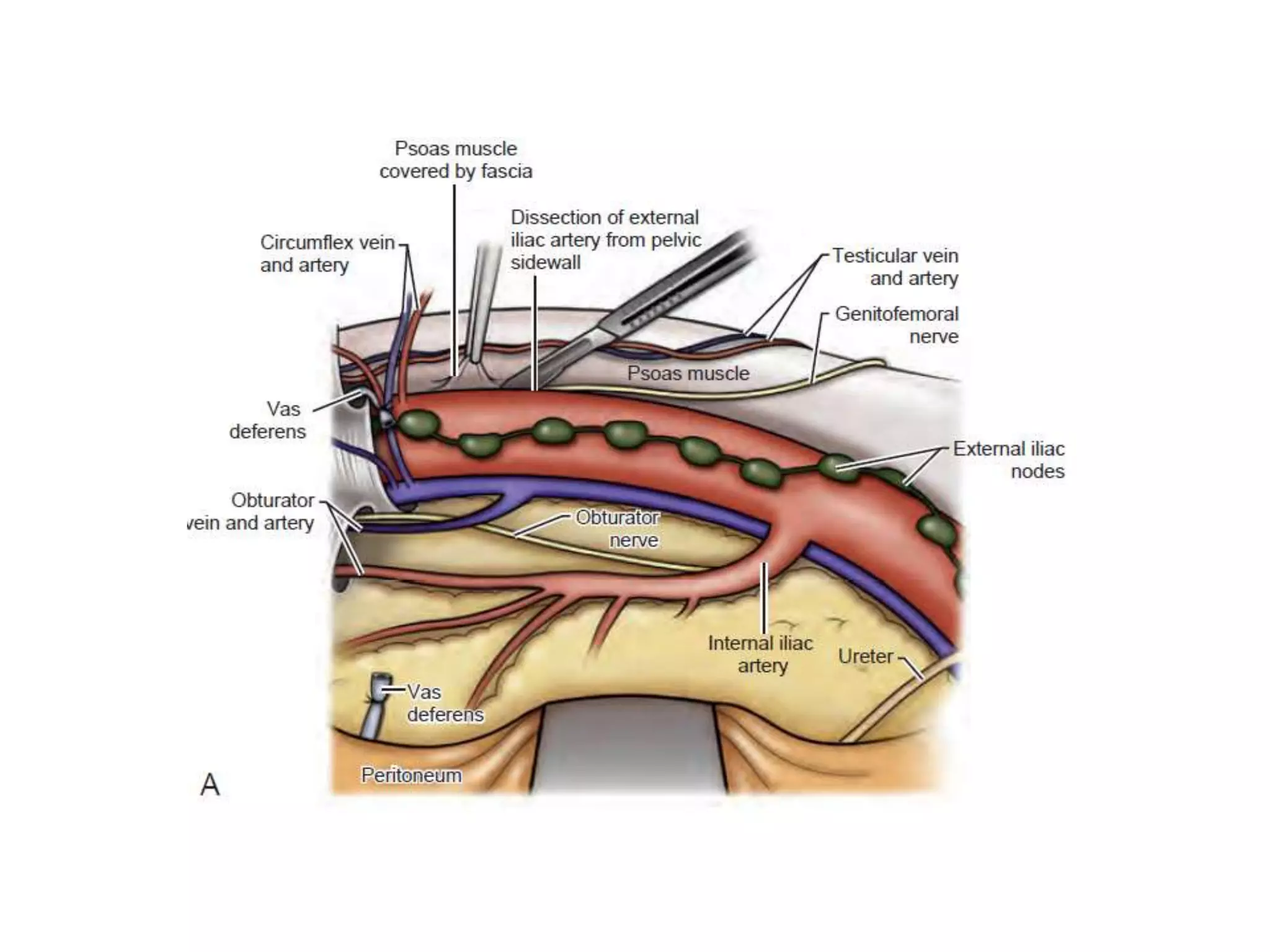
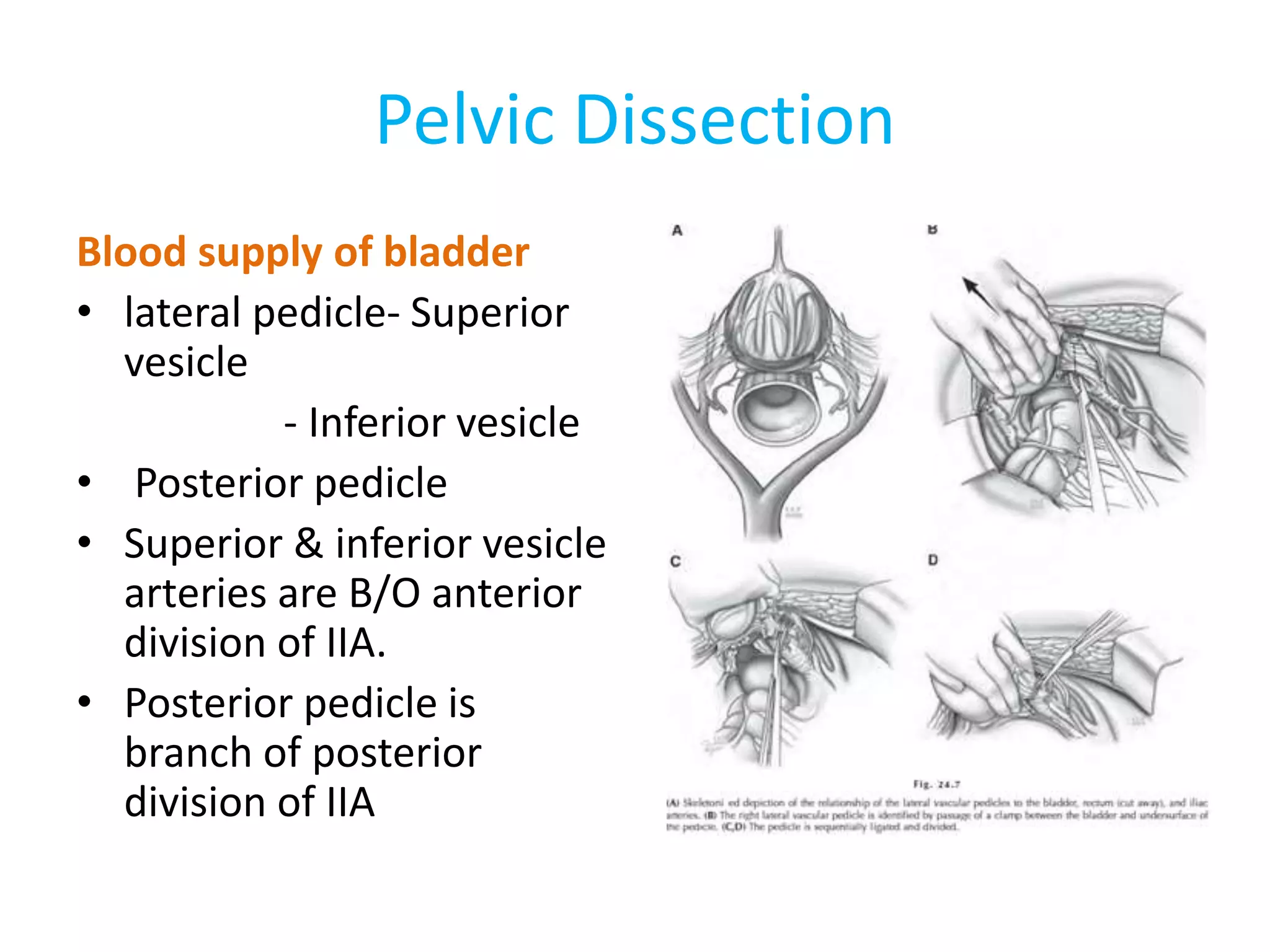
1) Radical cystectomy involves removal of the bladder and adjacent organs for muscle-invasive or high-risk non-muscle invasive bladder cancer.
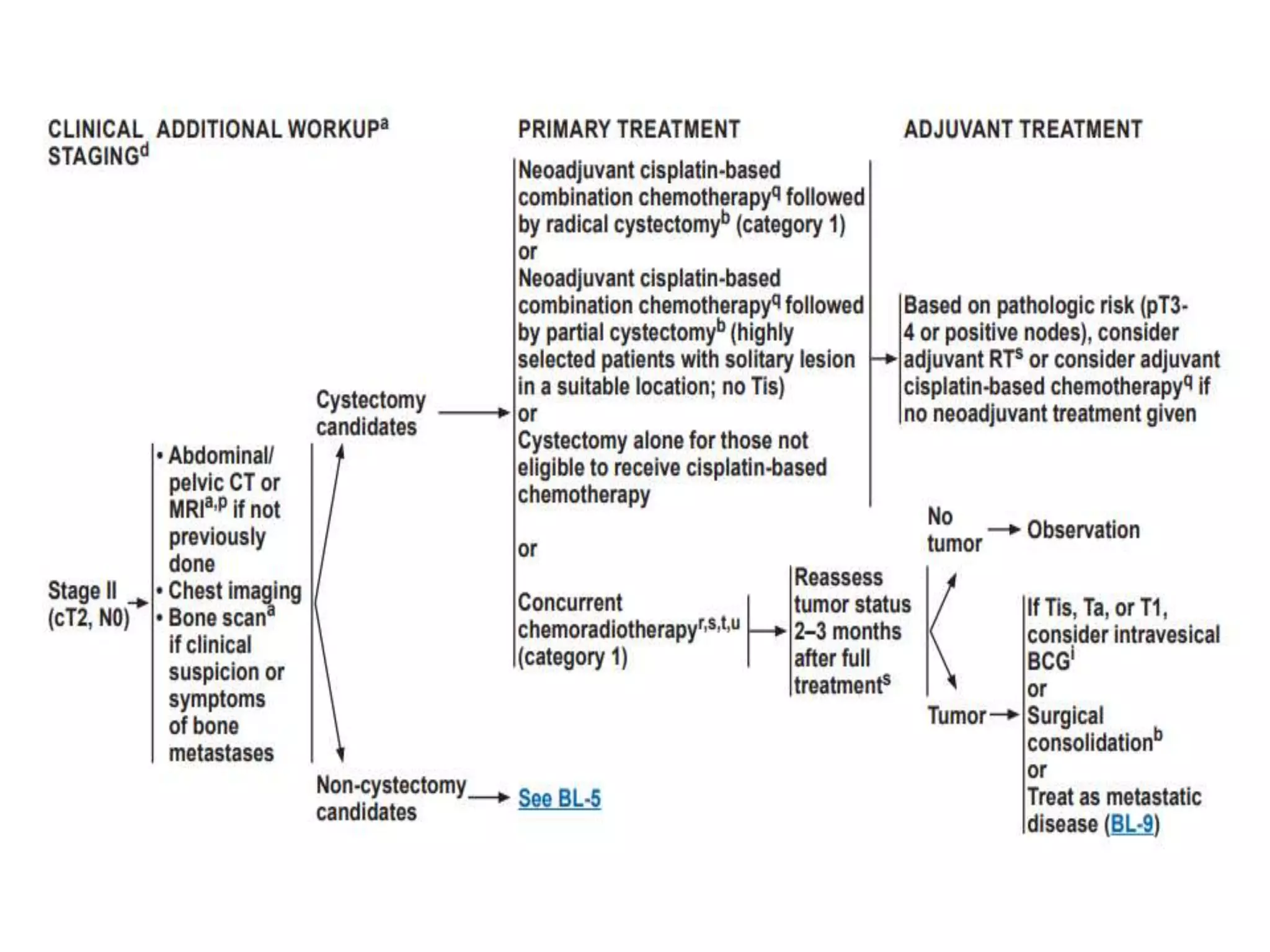
2) Neoadjuvant chemotherapy prior to surgery offers benefits like improved survival and early control of micrometastases for muscle-invasive tumors.
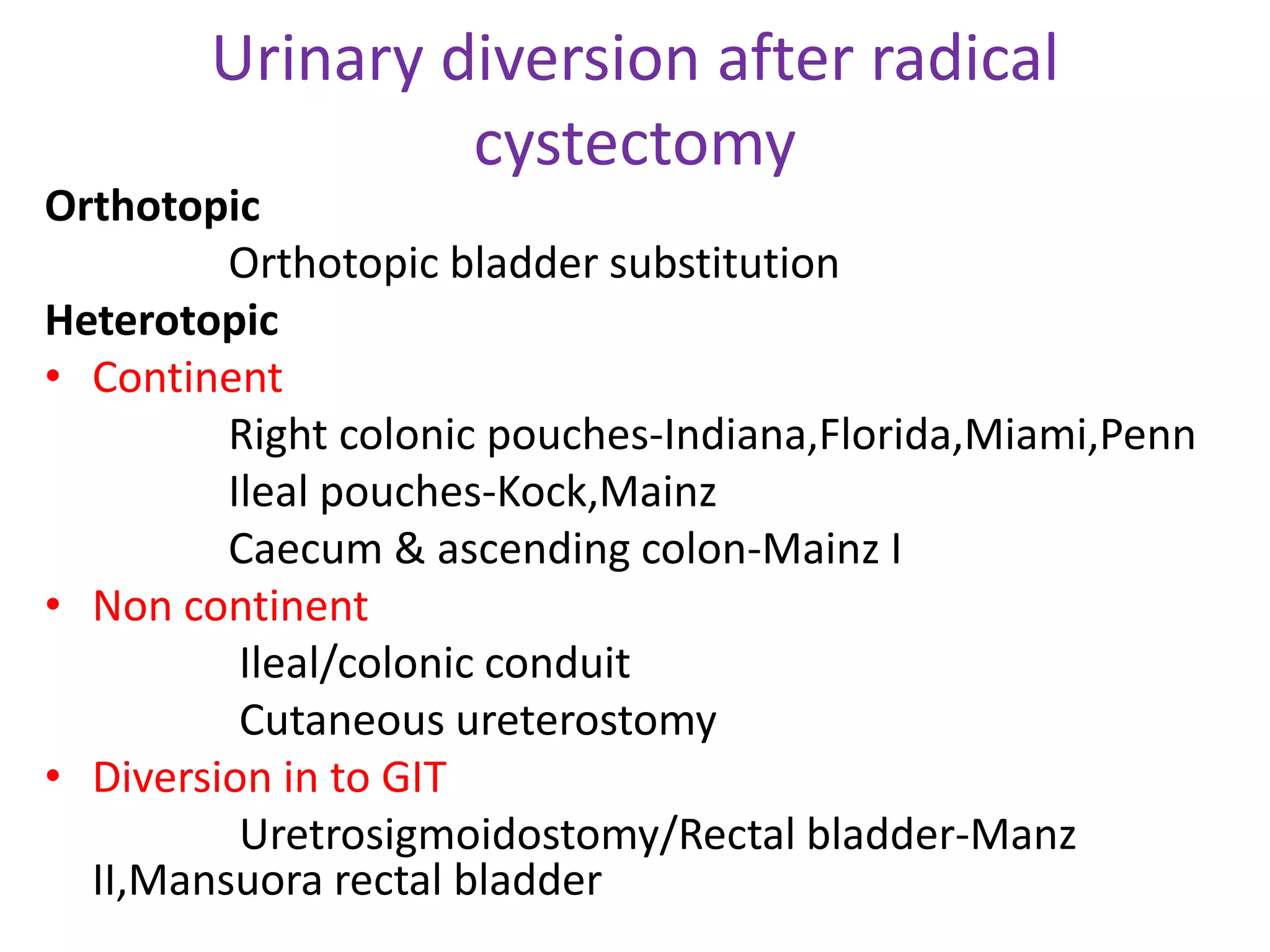
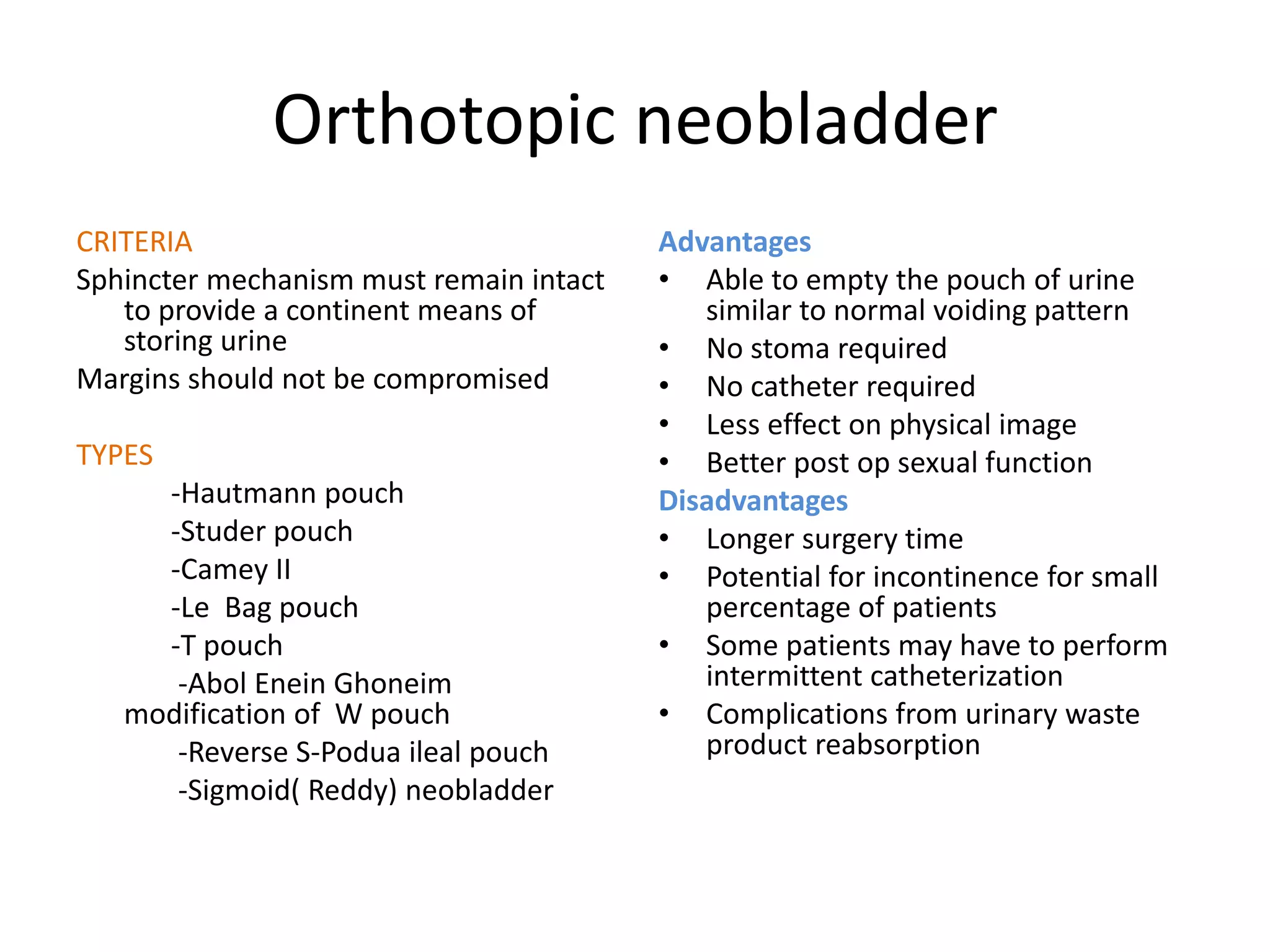
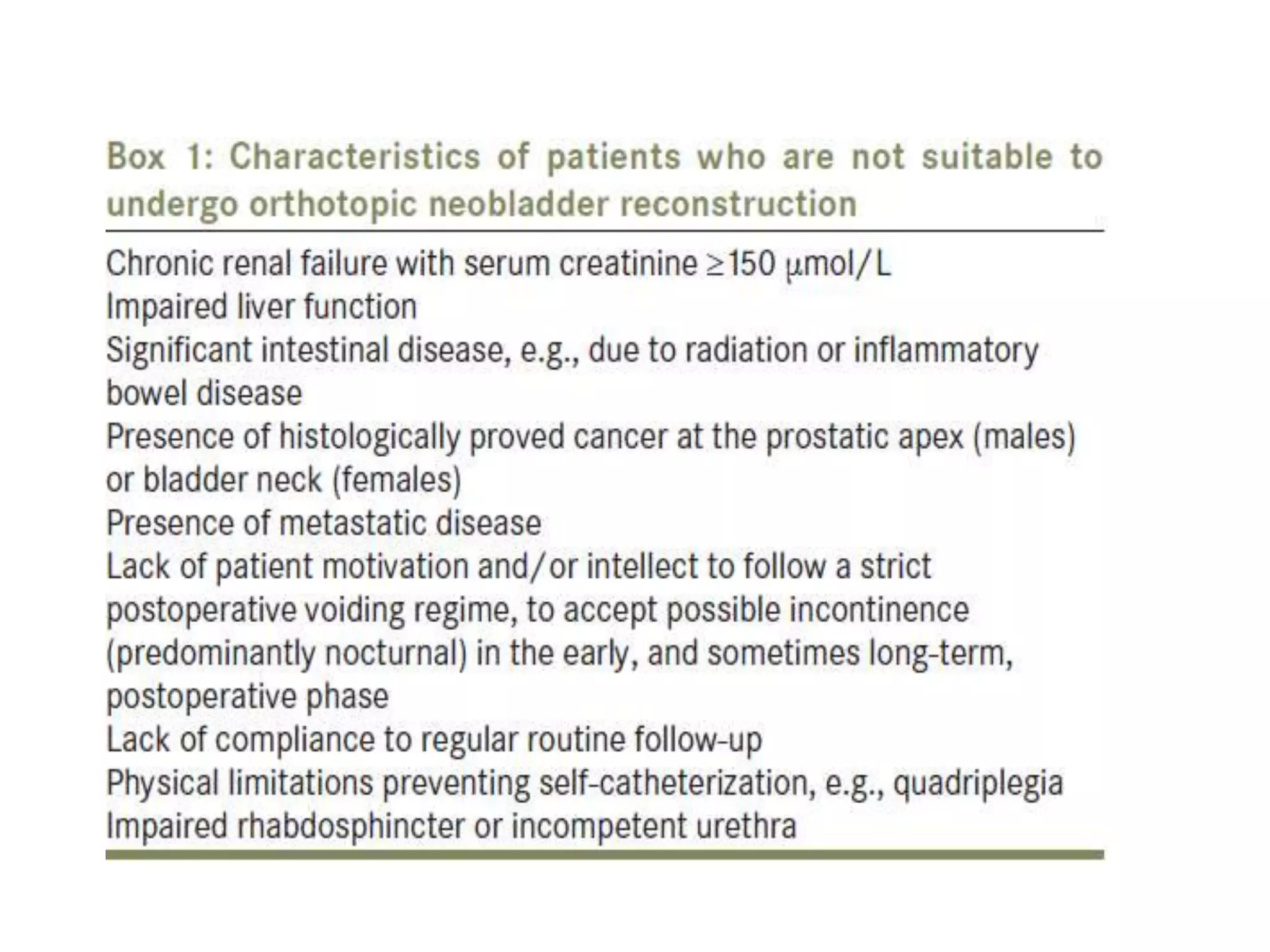
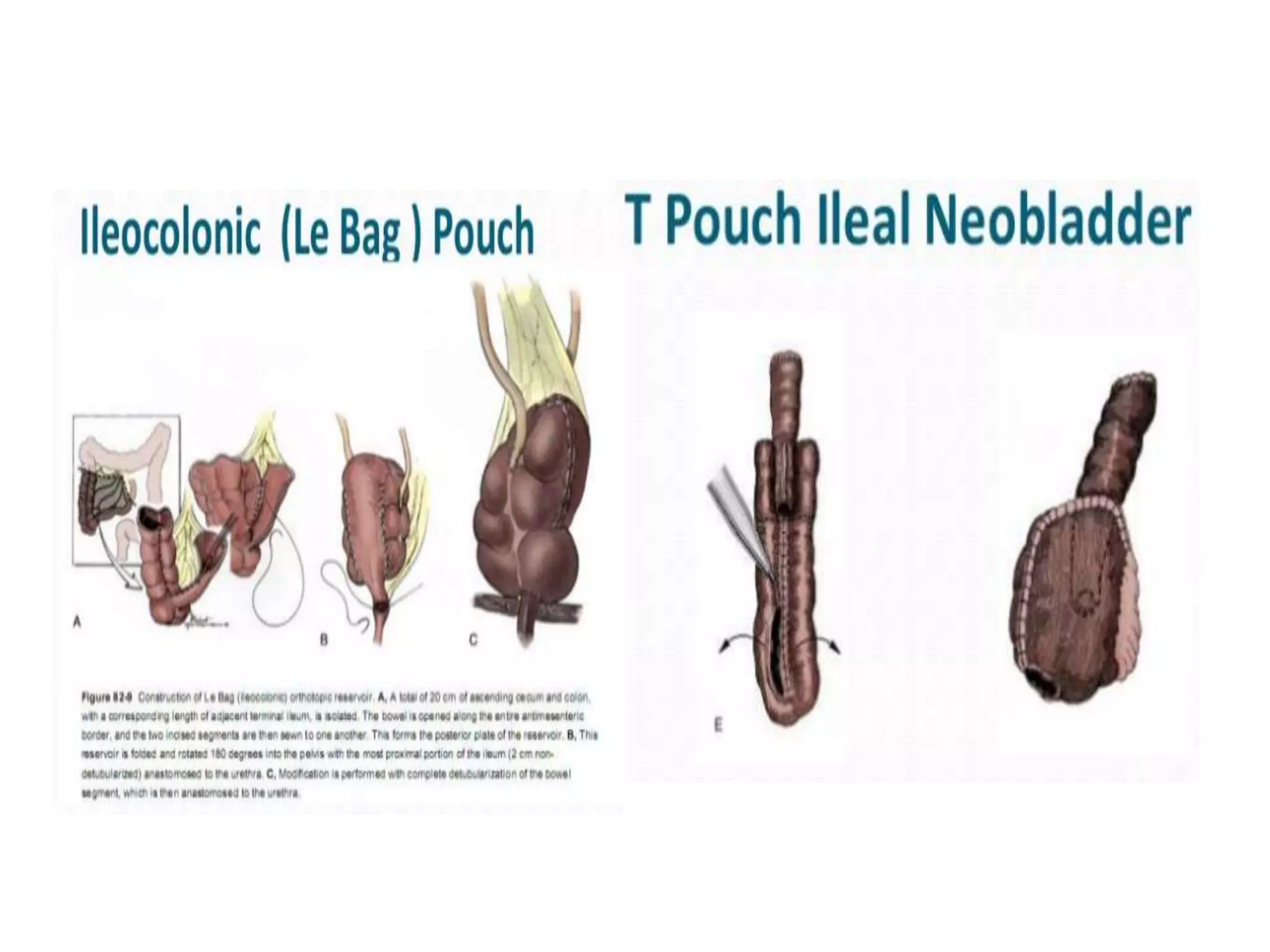
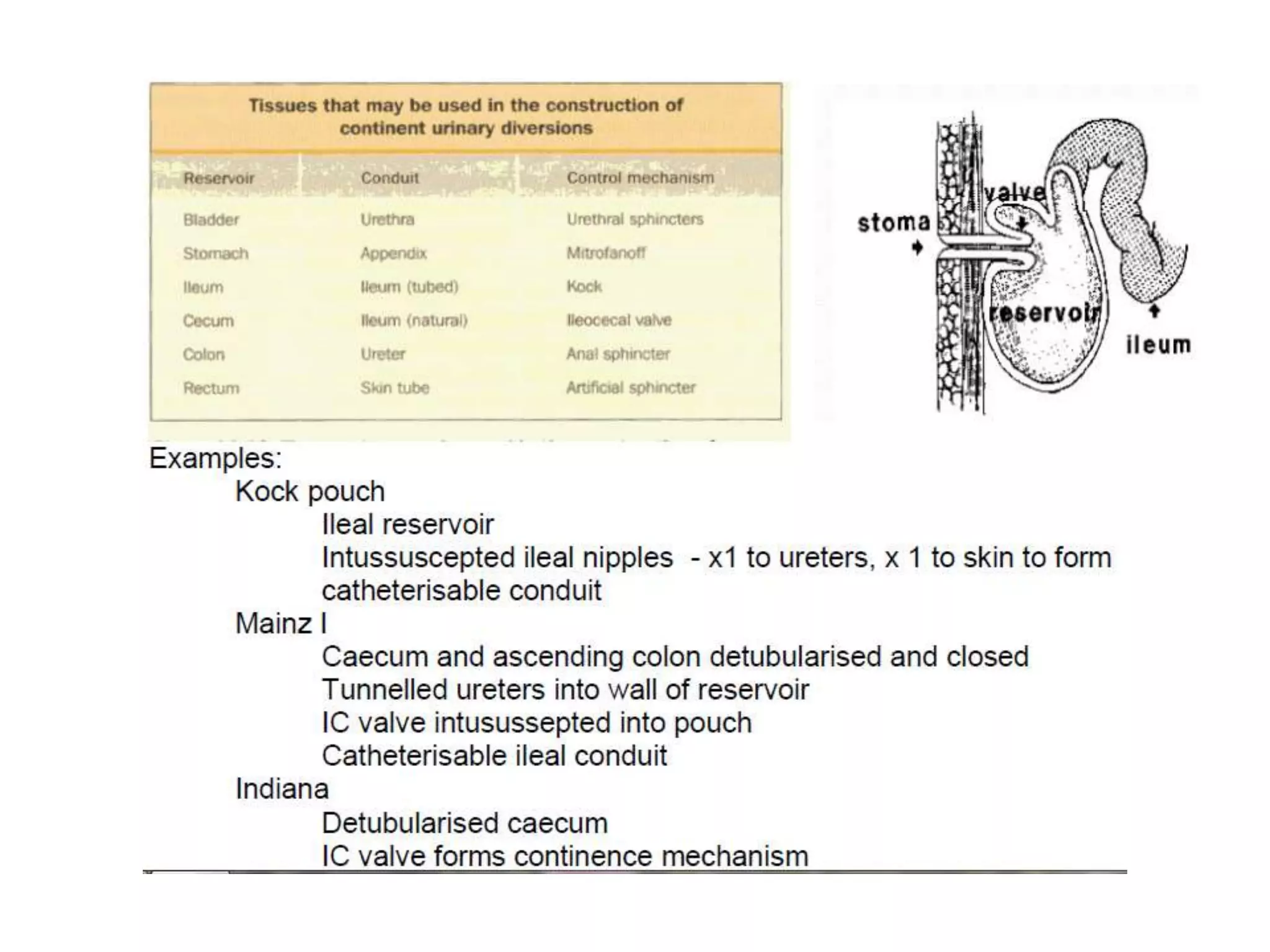
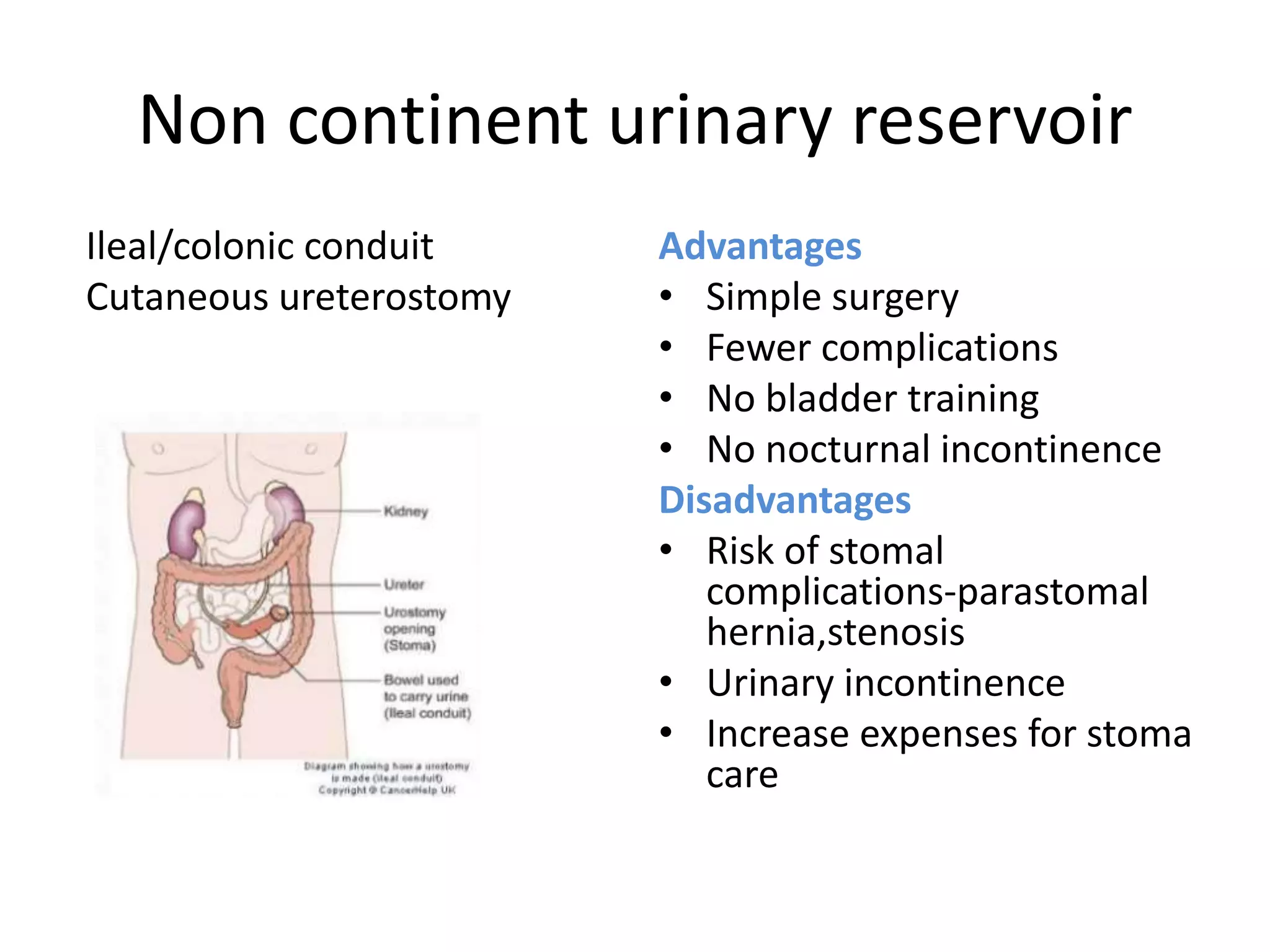
3) Urinary diversion options after cystectomy include orthotopic neobladder reconstruction to allow near-normal voiding or continent reservoirs requiring clean intermittent catheterization, or non-continent options like ileal conduit that require a stoma.



















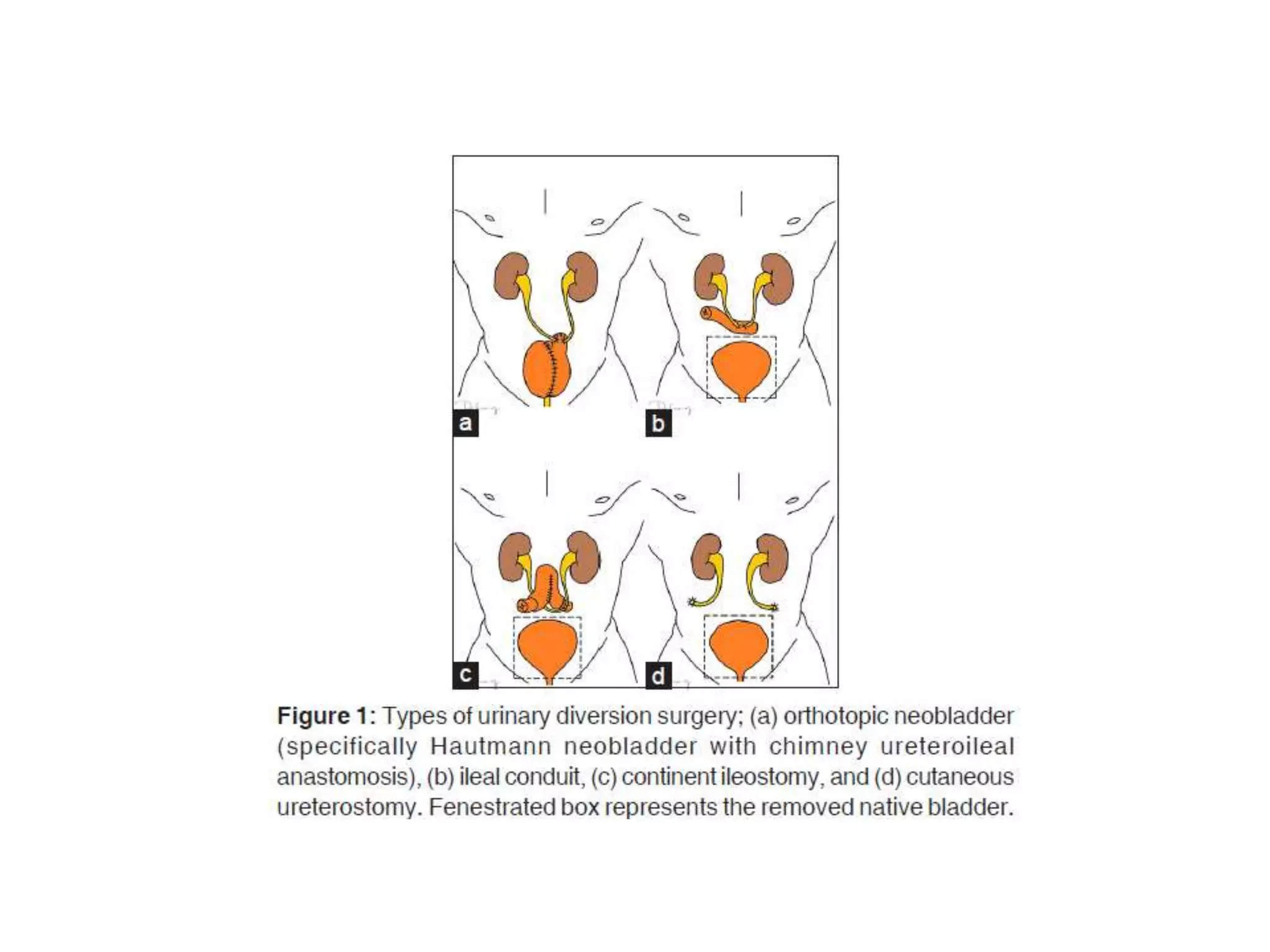



















![Urinary Diversion after cystectomy [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/urinarydiversionedmond-140716212817-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
























![Muscle invasive bladder Cancer [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/muscleinvasivebladdertumoredmond-140716213247-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






































