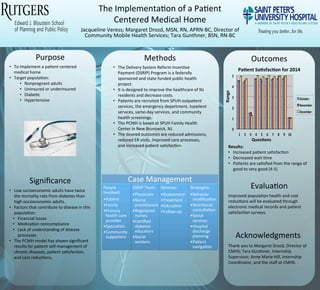
The document describes the implementation of a patient centered medical home (PCMH) at Saint Peter's University Hospital (SPUH) Family Health Center in New Jersey. The PCMH aims to improve healthcare for New Jersey residents and decrease costs through a federally sponsored public health project. Key goals of the PCMH include reducing admissions and emergency room visits, improving care processes, and increasing patient satisfaction. Initial results show increased patient satisfaction and decreased wait times.
SRF Webinar: Beyond DUP - Addressing Disengagement in Community-based Early I...wef
Presentation made March 22, 2017, during the live webinar hosted by Schizophrenia Research Forum (SRF). Event recording and additional slides at http://www.schizophreniaforum.org/forums/achieving-effective-treatment-early-psychosis-united-states
SRF Webinar - What It Will Take to Make Coordinated Specialty Care Available ...wef
Presentation made March 22, 2017, during the live webinar hosted by Schizophrenia Research Forum (SRF). Event recording and additional slides at http://www.schizophreniaforum.org/forums/achieving-effective-treatment-early-psychosis-united-states
SRF Webinar: Beyond DUP - Addressing Disengagement in Community-based Early I...wef
Presentation made March 22, 2017, during the live webinar hosted by Schizophrenia Research Forum (SRF). Event recording and additional slides at http://www.schizophreniaforum.org/forums/achieving-effective-treatment-early-psychosis-united-states
SRF Webinar - What It Will Take to Make Coordinated Specialty Care Available ...wef
Presentation made March 22, 2017, during the live webinar hosted by Schizophrenia Research Forum (SRF). Event recording and additional slides at http://www.schizophreniaforum.org/forums/achieving-effective-treatment-early-psychosis-united-states
Improving Discharge Care for Children with Special Health Care Needs through...LucilePackardFoundation
Being discharged from the hospital is a vulnerable time for families and caregivers of children with special health care needs (CSHCN). Appropriate resources and support are essential for care at home and can prevent complications or readmission. The California-based Nurse-led Discharge Learning (CANDLE) Collaborative brings together interdisciplinary clinicians to improve discharge care delivery for CSHCN. Learn about two new discharge practices: closed-loop medication reconciliation and tailored medication teaching, and multidisciplinary discharge rounds with early discharge notification. Speakers share how these innovative practices can be integrated into existing clinical workflows.
Advancing Team-Based Care: Complex Care Management in Primary CareCHC Connecticut
This webinar investigated the ways that team members can contribute to the care of patients with complex medical and/or social needs. The focus was on developing the expanded care team and ensuring ready communication between the core and expanded care teams. Models for effective care management were presented.
This webinar was presented May 5, 2016 3:00 p.m. Eastern Time
Advancing Team-Based Care: Enhancing the Role of the Medical AssistantCHC Connecticut
In this webinar, we explored the expanded role that medical assistants play in improving patient health outcomes. The role of the medical assistant was explored in population management, using electronic dashboards, and health coaching. We discussed how state-by-state variation and regulation may influence medical assistant practice.
We provide ongoing care coordination, transitional care management and concierge placement services combined with specialized senior real estate services.
By helping families and maturing adults navigate the aging process our goal is to alleviate the anxiety associated with the aging process and our current fragmented healthcare system.
General Practice Transformation Champions: Working as a teamNHS England
Workshops session 2 Presentation: Working as a team – working with pharmacists, paramedics, voluntary sector and community nurses to improve care by Steve Kell
Advancing Team-Based Care: The Emerging Role of Nurses in Primary CareCHC Connecticut
In this webinar, we explored the emerging role of nurses in primary care. We explored the role of nurses in the team, in complex care management, and in independent nurse visits.
This webinar was presented March 31, 2016 2:00 PM ET
Improving Discharge Care for Children with Special Health Care Needs through...LucilePackardFoundation
Being discharged from the hospital is a vulnerable time for families and caregivers of children with special health care needs (CSHCN). Appropriate resources and support are essential for care at home and can prevent complications or readmission. The California-based Nurse-led Discharge Learning (CANDLE) Collaborative brings together interdisciplinary clinicians to improve discharge care delivery for CSHCN. Learn about two new discharge practices: closed-loop medication reconciliation and tailored medication teaching, and multidisciplinary discharge rounds with early discharge notification. Speakers share how these innovative practices can be integrated into existing clinical workflows.
Advancing Team-Based Care: Complex Care Management in Primary CareCHC Connecticut
This webinar investigated the ways that team members can contribute to the care of patients with complex medical and/or social needs. The focus was on developing the expanded care team and ensuring ready communication between the core and expanded care teams. Models for effective care management were presented.
This webinar was presented May 5, 2016 3:00 p.m. Eastern Time
Advancing Team-Based Care: Enhancing the Role of the Medical AssistantCHC Connecticut
In this webinar, we explored the expanded role that medical assistants play in improving patient health outcomes. The role of the medical assistant was explored in population management, using electronic dashboards, and health coaching. We discussed how state-by-state variation and regulation may influence medical assistant practice.
We provide ongoing care coordination, transitional care management and concierge placement services combined with specialized senior real estate services.
By helping families and maturing adults navigate the aging process our goal is to alleviate the anxiety associated with the aging process and our current fragmented healthcare system.
General Practice Transformation Champions: Working as a teamNHS England
Workshops session 2 Presentation: Working as a team – working with pharmacists, paramedics, voluntary sector and community nurses to improve care by Steve Kell
Advancing Team-Based Care: The Emerging Role of Nurses in Primary CareCHC Connecticut
In this webinar, we explored the emerging role of nurses in primary care. We explored the role of nurses in the team, in complex care management, and in independent nurse visits.
This webinar was presented March 31, 2016 2:00 PM ET
Kevin Waida, a business graduate of the University of Missouri-Columbia, is an avid football fan. Kevin Waida follows NFL and college football and has had success playing in fantasy football leagues.
Valeo Transmission Systems Clutch SAT-HEC valeoscope product focus 998121Hugo Vallet
Valeo Transmission Systems’ mission is to be the supplier of choice for all powertrain architectures with innovative technologies developed for efficient and comfortable power transfer from the engine to the transmission, whilst reducing fuel consumption.
• Find Valeo clutch offer on spare parts on http://www.valeoservice.com
Discover other valeoscope brochures:
• Air Conditioning: http://www.slideshare.net/ValeoService/valeo-air-conditioning-valeoscope-technical-brochure-ac-handbook-part-1-998321
• Clutch KIT4P conversion kits: http://www.slideshare.net/ValeoService/valeo-transmission-systems-clutch-kit4p-valeoscope-technical-handbook-998100
• Clutch hydraulics CSC, CMC & CRC: http://slideshare.net/ValeoService/valeo-transmission-systems-clutch-hydraulics-valeoscope-product-focus-998123
• Dual-Mass flywheel technology: http://www.slideshare.net/ValeoService/valeo-transmission-systems-dualmass-flywheel-valeoscope-product-focus-998120
• Lighting System technologies: http://www.slideshare.net/ValeoService/valeo-lighting-systems-from-light-to-advanced-vision-technologies-valeoscope-technical-handbook-998542
• Truck brake pad diag & fit: http://www.slideshare.net/ValeoService/truck-brake-pad-fault-assessment-valeoscope-diagfit-brochure-957100
Valeo, automotive technology, naturally.
• Follow Valeo on facebook : http://www.facebook.com/Valeo.Group
Proyecto Smart ICU. Dr. Francisco Murillo_ Espanoleveris/ ehCOS
ehCOS SmartICU: Una solución innovadora para las unidades de cuidados intensivos usando big data y análisis predictivo. Ver más información del producto en: http://www.ehcos.com/productos/ehcos-icu/
Safe transition for young people to adulthood
Dr Jacqueline Cornish,
National Clinical Director Children, Young People and Transition to
Adulthood - NHS England
NHS Improving Quality held an event in London on 31 July 2013 to progress the children and young people transition to adult services work with a focus on turning the rhetoric into practice entitled “Working to Define a Generic Service Specification for Transition”
Northumberland County Project Presentation February 2024.pdfDataNB
Primary healthcare often lacks the integration and coordination of care for complex-needs patients: patients with a combination of multiple chronic conditions, who are high-cost users, and are often older. Care is benefitted from coordination among health and social services, and community organizations. A new care coordination model is needed to assist these complex-needs patients.
This presentation will discuss and summarize this project, which developed a new care coordination model, with the goal to strengthen primary healthcare in the community for complex-needs patients. Using a novel, technology-enabled, integrated case-management approach, the overall goal was to decrease rates of ER visits and acute hospital admissions.
Can we solve the adult primary care shortage without more physicians? CHC Connecticut
Tom Bodenheimer,of the Center for Excellence in Primary Care at UCSF Dep’t of Family and Community Medicine talks about addressing the primary care shortage at the 2014 Weitzman Symposium
Person Centered Care through Integrating a Palliative Approach: Lessons from ...BCCPA
Aging adults are entering residential care facilities with more advanced disease than in the past and their length of stay is shorter. Most health care providers in these facilities do not receive targeted education and training in palliative care, nor are they confident to have crucial conversations about goals of care and end of life challenges with residents and their families. Due to limited capacity to manage predictable symptoms related to end of life and insufficient planning, many residents are transferred to hospital in crisis and die in the Emergency Department or acute care wards.
This presentation will showcase some of the initiatives by identifying common themes, unique features of each and strategies for success. Opportunity will be given for delegates to ask questions and brainstorm how lessons learned from these initiatives could inform the care provided at their own facility.
Presented by:
- Jane Webley, RN LLB Regional lead, End of Life, Vancouver Coastal Health (EPAIRS and the Daisy project)
- Dr Christine Jones, Island Health (SSC project: Improving end of life outcomes in residential care facilities: A palliative approach to care)
- Kathleen Yue, RN, BSN, MN, CHPCN (c) Education Coordinator, BC Center for Palliative Care
Reducing Health Disparities: The Journey of Brightpoint HealthBrightpoint Health
Brightpoint Health's CEO and President, Paul Vitale and Chief Clinical Officer, Dr. Barbara Zeller, share Brightpoint's journey, strategies and best practices to reduce health disparities in New York City's high-need neighborhoods.
Improvement Story session at the 2013 Saskatchewan Health Care Quality Summit. For more information about the summit, visit www.qualitysummit.ca. Follow @QualitySummit on Twitter.
Better Care
Germain Bukassa Kazadi
Sussex Partnership NHS Foundation Trust - one of the partners working with NHS Improving Quality on the Winterbourne Medicines Programme
Presentation from the Winterbourne Medicines Programme Launch held in London on 10 September 2014
Ensuring safe, appropriate and optimised use of medication for people with learning disabilities who demonstrate behaviour that can challenge
National Conference on Health and Domestic Violence. Plenary talk Paul Grundy
explaining how the Patient Centered Medical Home (PCMH) platform for healthcare deliver is more likely to support domestic violence prevention and creat a safer environment than the FFS episode of care system we are in now. The medical Home is a home for the data where the all the data goes and is held accountable this idea was first articulated by Dr. Calvin C.J. Sia, a Honolulu-based pediatrician in 1967.
This concept of the medical home was integrated with Ed Wagners Chronic disease Model and Thomas Bodenheimer Kevin Grumbach advanced/proactive primary care at the request of the Patient Centered Primary care Collaborative into a set of principles Know as the Joint principles of the Patient centered medical home.
The patient-centered medical home (PCMH), is a team based health care delivery set of principles led by a physician that provides comprehensive and continuous medical care to patients with the goal of obtaining maximized health outcomes. It is "an approach to providing comprehensive primary care for children, youth and adults" The provision PCMH medical homes allow better access to health care, increase satisfaction with care, and improve health. Joint principles that define a PCMH have been established through the cohesive efforts of the American Academy of Pediatrics (AAP), American Academy of Family Physicians (AAFP), American College of Physicians (ACP), and American Osteopathic Association (AOA).[10] Care coordination is an essential component of the PCMH. Care coordination requires additional resources such as health information technology, and appropriately trained staff to provide coordinated care through team-based models. Additionally, payment models that compensate PCMHs for their effort devoted to care coordination activities and patient-centered care management that fall outside the face-to-face patient encounter may help encourage coordination.
Children and Young People with Diabetes A National Approach to Improving Care and Outcomes
Dr Fiona M Campbell
Consultant Paediatric Diabetologist
Leeds Teaching Hospitals Trust & NHS Diabetes Clinical Lead for Paediatric Diabetes Network Development
NHS Improving Quality held an event in London on 31 July 2013 to progress the children and young people transition to adult services work with a focus on turning the rhetoric into practice entitled “Working to Define a Generic Service Specification for Transition”
DFCM Top 5 research studies that will impact clinical practice
Jacqui Veress - Internship Poster
1. The
Implementa,on
of
a
Pa,ent
Centered
Medical
Home
Jacqueline
Veress;
Margaret
Drozd,
MSN,
RN,
APRN-‐BC,
Director
of
Community
Mobile
Health
Services;
Tara
Gunthner,
BSN,
RN-‐BC
• The
Delivery
System
Reform
Incen,ve
Payment
(DSRIP)
Program
is
a
federally
sponsored
and
state
funded
public
health
project.
• It
is
designed
to
improve
the
healthcare
of
NJ
residents
and
decrease
costs.
• Pa,ents
are
recruited
from
SPUH
outpa,ent
services,
the
emergency
department,
inpa,ent
services,
same-‐day
services,
and
community
health
screenings.
• The
PCMH
is
based
at
SPUH
Family
Health
Center
in
New
Brunswick,
NJ.
• The
desired
outcomes
are
reduced
admissions,
reduced
ER
visits,
improved
care
processes,
and
increased
pa,ent
sa,sfac,on.
Results:
• Increased
pa,ent
sa,sfac,on
• Decreased
wait
,me
• Pa,ents
are
sa,sfied
from
the
range
of
good
to
very
good
(4-‐5)
• Low
socioeconomic
adults
have
twice
the
mortality
rate
from
diabetes
than
high
socioeconomic
adults.
• Factors
that
contribute
to
disease
in
this
popula,on:
• Financial
issues
• Medica,on
noncompliance
• Lack
of
understanding
of
disease
processes
• The
PCMH
model
has
shown
significant
results
for
pa,ent
self-‐management
of
chronic
diseases,
pa,ent
sa,sfac,on,
and
cost
reduc,ons.
• To
Implement
a
pa,ent
centered
medical
home
• Target
popula,on:
• Nonpregnant
adults
• Uninsured
or
underinsured
• Diabe,c
• Hypertensive
Purpose
Significance
Methods
Evalua,on
Outcomes
Improved
popula,on
health
and
cost
reduc,ons
will
be
evaluated
through
electronic
medical
records
and
pa,ent
sa,sfac,on
surveys.
Pa+ent
Sa+sfac+on
for
2014
Ques+ons
Range
Acknowledgments
Thank
you
to
Margaret
Drozd,
Director
of
CMHS;
Tara
Gunthner,
Internship
Supervisor;
Anne
Marie
Hill,
Internship
Coordinator;
and
the
staff
at
CMHS.
Case
Management
People
Involved:
• Pa,ent
• Family
• Primary
health
care
provider
• Specialists
• Community
supporters
DSRIP
Team:
• Physicians
• Nurse
prac,,oners
• Registered
nurses
• Cer,fied
diabetes
educators
• Social
workers
Services:
• Assessment
• Treatment
• Educa,on
• Follow-‐up
Strategies:
• Behavior
modifica,on
• Nutri,onal
consulta,on
• Social
services
• Hospital
discharge
planning
• Pa,ent
naviga,on