Fospropofol
• Water-soluble prodrugof propofol
• Fospropofol Propofol
(Prodrug) (Active metabolite)
• 1.86 mg of fospropofol sodium is the molar equivalent of 1
mg propofol
• Not associated with pain on injection
• Mild to moderate perineal paresthesias and pruritis minutes
after a bolus injection of fospropofol ( due to Formaldehyde
byproduct )
• More potent , Slower onset , More Vd
5.
Mechanism of action
•Sedative hypnotic
• GABAA Modulator
• increases binding affinity of GABA for the GABAA receptor
• coupled to a chloride channel,
• Activation of the receptor leads to hyperpolarization of the
nerve membrane.
• No direct action on spinal cord
6.
Pharmacokinetics
• Intravenous administrationfor the induction of general
anesthesia and for moderate to deep sedation
• rapid onset of action
• Produce unconsciousness within 30 seconds
• Recovery from propofol is more rapid
• Minimal residual CNS effect
• Fast blood brain barrier achieved
7.
• Hepatic clearance:30-60 ml/kg/min
[If 50 kg patient= 1500-3000 ml/min]
• But, Hepatic blood flow : 800-1200 ml/min
• As propofol hepatic clearance > Hepatic blood flow,
Extrahepatic elimination does occur.i.e Renal and Pulmonary
• Under hepatic clearance,
Propofol glucoronidation Inactive metabolites
(Water soluble excreted
in urine)
9.
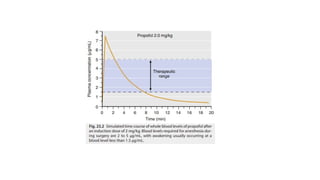
• T1/2 =30 – 90 min
• Context sensitive half life : 40 minutes
Drug Interactions:
• Midazolam can reduce the required propofol dose by more
than 10%
• Hence , Many clinicians administer a small amount of
midazolam (eg, 30 mcg/kg) prior to induction with propofol
10.
• Pharmacokinetics ofpropofol may be altered by various factors
(e.g., gender, weight, preexisting disease, age, and concomitant
medication )
Reduced cardiac output ( in elderly) ; hence Low Vd
Decreased
elimination
In a hemorrhagic shock , propofol concentrations increased 20
%.
Women have a larger volume of distribution and higher
clearance rates
Relatively larger central compartment volume (50%) and a more
rapid clearance (in children ) ; hence large dose requirement
11.
Pharmacodynamics
Effects on CNS:
• Decreases cerebral blood flow
• Decreases intracranial pressure
• Provide a comparable degree of cerebral protection
• Reduces intraocular pressure
• Has anticonvulsant properties
12.
• Effects onCardiovascular system
• decrease in arterial blood pressure
• Decease in preload and cardiac contractility
• markedly impairs the normal arterial baroreflex response to
hypotension
• Rarely, Vagally mediated reflex bradycardia
• Heart rate unaffected
• Decrease in arterial blood pressure from propofol during the
infusion phase is much less than intravenous bolus dose.
13.
Effects on Respiratorysystem
• Profound respiratory depressant
• Causes apnea following an induction dose
• Inhibits hypoxic ventilatory drive and depresses the normal
response to hypercarbia
• Depression of upper airway reflexes
• Decreases tidal volume
• Increases respiratory frequency
• Induces bronchodilation in patients with COPD
• Potentiates hypoxic pulmonary vasoconstriction
14.
Other Effects
• doesnot trigger malignant hyperthermia
• does not enhance neuromuscular blockade
• Possesses significant antiemetic activity ( 10 mg in adults )
• Associated with the development of pancreatitis, which may
be related to hypertriglyceridemia
• Intralipid : excellent culture medium,
• Hence , More infection associated with propofol
15.
Uses
• Induction :
intravenous induction dose is 1 to 2.5 mg/kg.
in elderly patients ;
1 mg/kg (with premedication)
1.75 mg/kg (without premedication)
In children ;
2-3 mg/kg
16.
• Maintenance :
After an induction dose, an infusion dose : 100 to 200
μg/kg/min
If 50 kg patient ;
• 5 – 10 mg/min
• 300 - 600 mg/ hr
• 30 – 60 ml/ hr
17.
• For Sedation:
30-60 μg/kg/min
Infusion should be individually titrated to the desired effect
In 50 kg patient;
• 1.5 – 3 mg / min
• 90 – 180 mg / hr
• 9 – 18 ml / hr
Recommended maximal dose of propofol infusion rate :
80 μg/kg/min
18.
SIDE EFFECTS AND
CONTRAINDICATIONS
•Allergic reaction
• Abuse Potential
• During induction :
• pain on injection
• Myoclonus
• Apnea
• Hypotension
• rarely, thrombophlebitis of the vein
• Potential risks to fetal brain development
• Bacterial growth ; E.Coli & Pseudomonas aerogenosa
19.
Propofol Infusion Syndrome
•Rare but lethal syndrome
• Associated with infusion of propofol at 4 mg/kg/h or more
for 48 hours or longer
• Acute refractory bradycardia leading to asystole
• Along with 1 or more of following:
• metabolic acidosis (base deficit >10 mmol/ L 1)
−
• rhabdomyolysis
• Hyperlipidemia
• enlarged or fatty liver
20.
Ketamine
• structural analogueof phencyclidine
• one-tenth as potent, yet retains many of phencyclidine’s
psychotomimetic effects
• Highly lipid soluble
21.
Mechanism of action
•inhibit N-methyl-D-aspartate (NMDA) channels and neuronal
hyperpolarization-activated cationic (HCN1 ) channels
• functionally “dissociates” sensory impulses from the limbic
cortex (which is involved with the awareness of sensation)
• patient to appear conscious (eg, eye opening, swallowing,
muscle contracture) but unable to process or respond to
sensory input
• additional actions on endogenous analgesic pathways
22.
Pharmacokinetics
• administered orally,nasally, rectally, subcutaneously, and
epidurally, but in usual clinical practice it is given
intravenously or intramuscularly
• Peak plasma levels are usually achieved within 10 to 15 min
after intramuscular injection
23.
• Ketamine increasein cerebral blood flow and cardiac output
• Hence, rapid brain uptake and subsequent redistribution
• Awakening is due to redistribution from brain to peripheral
compartments.
• Biotransformed in the liver to several metabolites, one of
which is norketamine
• End products of ketamine biotransformation are excreted
renally.
24.
Pharmacodynamics
• Effects onCNS
• increases cerebral oxygen consumption
• increase in CMRO2
• Increases cerebral blood flow
• Increases intracranial pressure
• Dilates pupil moderately and causes nystagmus
• Lacrimation and Salivation common
25.
• Emergence reactions:
•vivid dreaming
• extracorporeal experiences (sense of floating out of body)
• illusions (misinterpretation of a real, external sensory experience)
• Occurs in 1st hour then abates
• Benzodiazepine attenuates incidence & severity of Emergence
rxn
• Antidepressant effects : 0.5 mg/kg, given as a 40-minute infusion
26.
• Effects onCardiovascular system
• Increases arterial blood pressure, heart rate, and cardiac
output
• Increases in pulmonary artery pressure and myocardial
work
• Causes systemic release of catecholamines
• Inhibition of the vagal nerve
• Inhibition of norepinephrine reuptake at peripheral nerves
• Direct myocardial depressant ; use cautiously in patient with
depleted catecholamine stores
27.
• Effects onRespiratory system:
• minimal response on the central respiratory drive
• Response to CO2 preserved
• Transient (1-3 minutes) decrease in minute ventilation after the
bolus administration
• Relaxes bronchial smooth muscle
• Increases oral secretions
• Can produce upper airway obstruction followed by laryngospasm
28.
Uses
• Induction andMaintenance of Anesthesia
• Desirable in:
• Unstable cardiovascular patients suffering from hypovolemia
• hemorrhagic shock
• cardiovascular depression in sepsis
• reactive airway disease
• Trauma patients with extensive blood loss
• In children with difficult vein access
29.
• Sedation andanalgesia
• Dose : 0.3-0.6 mg/kg IV over 2-3 min
2-4 mg/kg IM
0.5 to 1 mg/kg via Epidural / Caudal (Safety
controversial)
• During burn dressing changes , debridement procedures
• Supplementation of regional anesthesia
30.
Side Effects
• IncreasesHR, BP ,CO
• Stimulates oral secretion ( Antisialogue ; Glycopyrolate
helpful )
• Increases ICP and IOP
• Increases muscle tone
• Potentiation of Neuromuscular blockade
31.
Contraindications
• Raised ICP
•Raised IOP and Penetrating eye injuries
• Psychiatric disorders
• As sole anesthetic agent in Hypertensives, IHD and CVA
patients
#4 Metabolized by alkaline phosphatases in the liver
#5 facilitation of inhibitory neurotransmission mediated by GABAA receptor binding
No direct action on spinal cord unlike inhalational agent
#8 After a single bolus dose, whole blood propofol levels decrease rapidly as a result of redistribution and elimination . The initial distribution halflife of propofol is 2 to 8 minutes
#10 patients aged 80 years or older generally need 50% of the propofol dose of patients aged 20 years old to target the same level of sedation or hypnosis
#11 By GABA modulation, inhibits acetylcholine release in the hippocampus and prefrontal cortex
#12 due to a drop in systemic vascular resistance (inhibition of sympathetic vasoconstrictor activity)
vasodilatory and myocardial depressant effects are concentration-dependent
#13 allowing intubation, endoscopy, or laryngeal mask placement in the absence of neuromuscular blockade.
Maintaince at 100 mcg/kg/min, 40% decrease in tidal volume and a 20% increase in resp frequency
#18 Pretreatment with a small dose of propofol, opiates, nonsteroidal anti-inflammatory drugs, ketamine, esmolol/metoprolol, magnesium, a flash of light, clonidine/ ephedrine combination, dexamethasone, and metoclopramide all have been tested with variable efficacy
#19 Other features include cardiomyopathy with acute cardiac failure, skeletal myopathy, hyperkalemia, hepatomegaly, and lipemia
#23 s N-demethylation to form norketamine (metabolite I), which is then hydroxylated to hydroxynorketamine, which is further conjugated to water-soluble glucuronide derivates and excreted in the urine.
#24 duration of ketamine anesthesia after a single IV administration of a general anesthetic dose (2 mg/kg) is 10 to 15 minutes and full orientation to person, place, and time occurs within 15 to 30 minutes
plasma levels of 0.6 to 2 μg/mL: minimum concentration for anesthesia but in children 0.8 to 4
pain thresholds 0.1 μg/ml
Increase in CMRO2 and CBF can be blocked by the use of thiopental or diazepam.
#25 lasting for 3 to 12 days. A maintenance dose every 2 to 4 days m
#26 due to central stimulation of the sympathetic nervous system and inhibition of the reuptake of norepinephrine after release at nerve terminals
administered carefully to patients with coronary artery disease, uncontrolled hypertension, congestive heart failure, or arterial aneurysms
prior administration of benzodiazepines attenuates ketamine-induced tachycardia and systemic hypertension
Inhalation anesthetics and propofol blunt the hemodynamic effect of ketamine
#27 as reflected by an unaltered response to carbon dioxide
#28 a patient susceptible to malignant hyperthermia
With propofol : TIVA
#29 Multimodal analgesia
Sedation in Critical care. Pediatric patient.

![• Hepatic clearance: 30-60 ml/kg/min
[If 50 kg patient= 1500-3000 ml/min]
• But, Hepatic blood flow : 800-1200 ml/min
• As propofol hepatic clearance > Hepatic blood flow,
Extrahepatic elimination does occur.i.e Renal and Pulmonary
• Under hepatic clearance,
Propofol glucoronidation Inactive metabolites
(Water soluble excreted
in urine)](https://image.slidesharecdn.com/intravenousanesthesia-250520152219-3f66f822/85/INTRAVENOUS-ANESTHESIA-presentation-pptx-7-320.jpg)