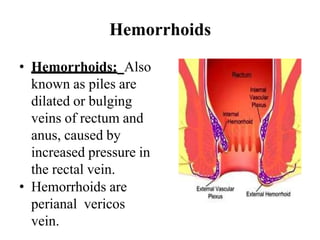
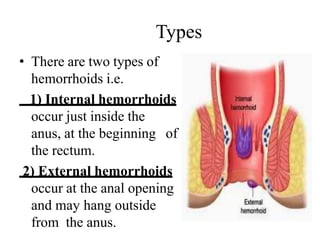
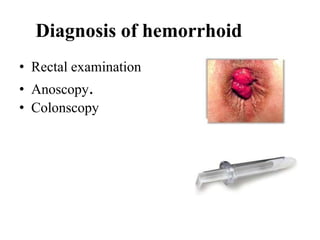
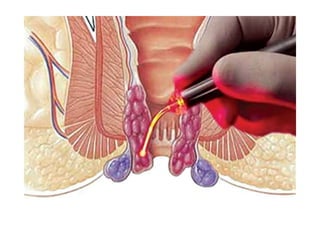
Hemorrhoids are swollen veins in the lower rectum or anus that can cause pain, itching and bleeding. There are two types - internal hemorrhoids located inside the rectum and external hemorrhoids under the skin around the anus. Risk factors include chronic constipation or diarrhea, prolonged sitting, pregnancy and obesity. Symptoms include pain, itching and bleeding with bowel movements. Treatment depends on the severity but may include increasing fiber, warm baths, creams/ointments, rubber band ligation or surgery. Nursing focuses on pain management, preventing complications and teaching about proper diet, bowel habits and hygiene.