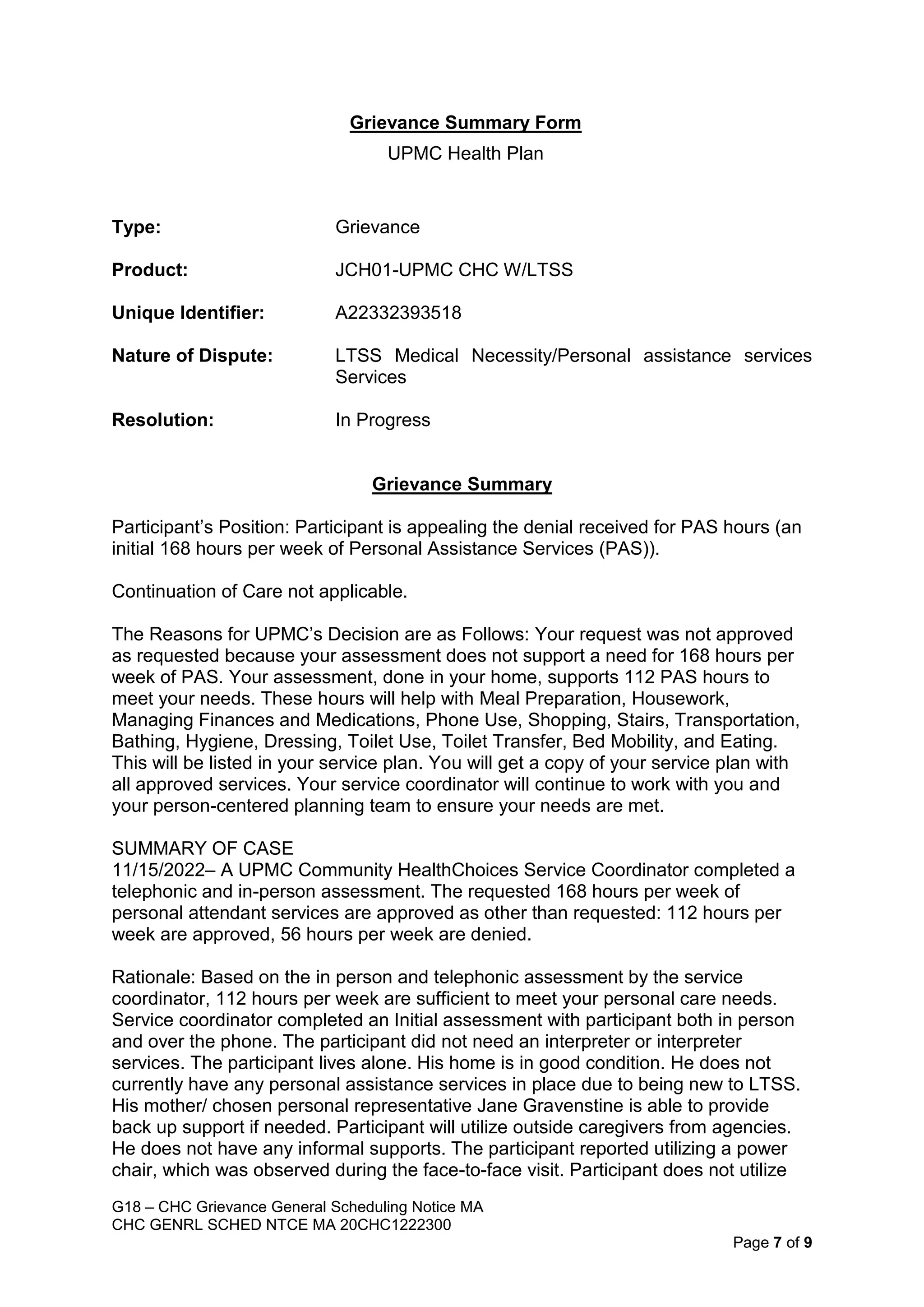
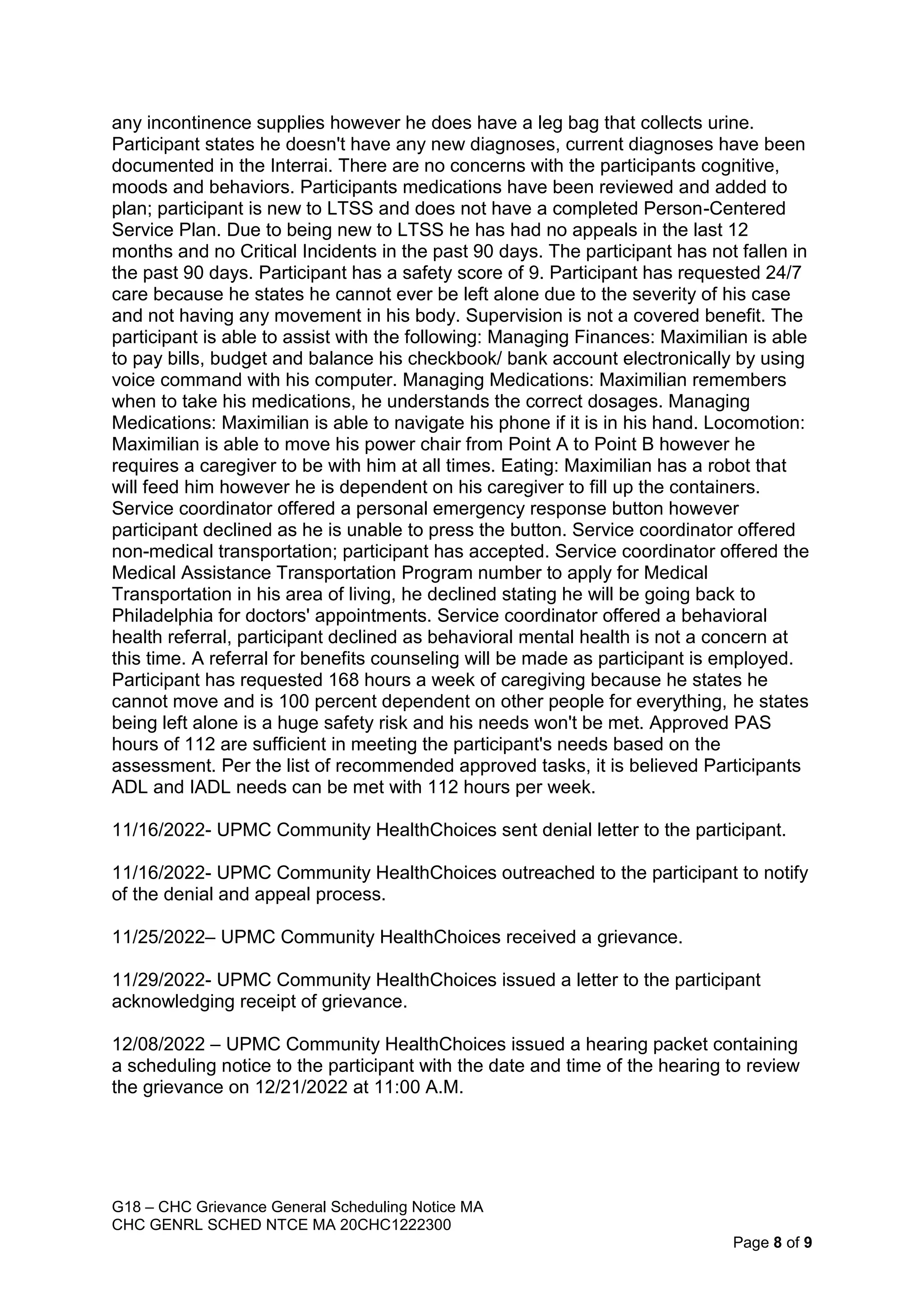
The document summarizes a grievance hearing scheduled for Maximilian Gravenstein regarding a denial of some requested personal assistance services. The hearing will be held on December 21st, 2022 at 11:00AM in Camp Hill, PA. The grievance review committee will consider information presented by UPMC Health Plan and Maximilian Gravenstein (or his representative) regarding the plan's denial of 56 hours per week of the originally requested 168 hours per week of personal assistance services. The committee will then make a decision on the grievance.



![CHC PARTIAL APPROVAL LTR N2 UM 20CHC1199233
[LTR-BD]
11/16/2022
MAXIMILIAN GRAVENSTEIN
17 S 2ND ST APT 103
HARRISBURG, PA 17101-2006
RE: MAXIMILIAN GRAVENSTEIN DOB: 02/11/1998
Dear MAXIMILIAN GRAVENSTEIN:
This is an important notice about your services. Read it carefully.
Call UPMC Community HealthChoices at 1-844-833-0523 (TTY: 711) if you have any
questions or need help. Representatives are available 24 hours a day, 7 days a week.
UPMC Community HealthChoices has reviewed the request for an initial 168 hours per week
of Personal Assistance Services (PAS) submitted by your Service Coordinator, Jillian Forscht,
for you on 11/15/2022. After physician review, the request is:
Approved other than as requested as follows:
112 hours per week of PAS are approved for your service plan.
56 hours per week of PAS are denied.
Your request was not approved as requested because your assessment does not support a
need for 168 hours per week of PAS. Your assessment, done in your home, supports 112 PAS
hours to meet your needs. These hours will help with Meal Preparation, Housework, Managing
Finances and Medications, Phone Use, Shopping, Stairs, Transportation, Bathing, Hygiene,
Dressing, Toilet Use, Toilet Transfer, Bed Mobility, and Eating. This will be listed in your
service plan. You will get a copy of your service plan with all approved services. Your service
coordinator will continue to work with you and your person-centered planning team to ensure
your needs are met.
What if I disagree with the decision to deny my request for services?
You may file a Complaint or Grievance with UPMC Community HealthChoices by
01/15/2023.](https://image.slidesharecdn.com/gravenstein-appeal-packetclean-221231204008-40d4c793/75/Appeal-Packet-7-2048.jpg)
![CHC PARTIAL APPROVAL LTR N2 UM 20CHC1199233
[LTR-BD]
You may ask for the medical necessity guidelines or other rules UPMC Community
HealthChoices used to make this decision, at no cost to you. To ask for a copy of the
medical necessity guidelines or other rules that UPMC Community HealthChoices used to
make the decision, call UPMC Community HealthChoices at 1-844-833-0523 (TTY: 711) or
write a letter. Representatives are available 24 hours a day, 7 days a week. If you file a
Complaint or Grievance, you can ask for a copy of this information by checking Box 3 on
the “Complaint/Grievance Request Form.”
• You may get a second opinion from another provider in UPMC Community HealthChoices
network. Call UPMC Community HealthChoices at 1-844-833-0523 (TTY: 711) to get a
referral for a second opinion. Asking for a second opinion will not give you more time to file
a Complaint or Grievance. It will not continue any service or item that you have been
getting.
How do I file a Complaint or Grievance?
You can file a Complaint or Grievance by phone, by using the “Complaint/Grievance Request
Form,” or by writing a letter.
To file a Complaint or Grievance:
By Phone: Call UPMC Community HealthChoices at 1-844-833-0523. TTY users should
call 711.
By Fax: Fax the “Complaint/Grievance Request Form” or a letter to 412-454-7920; or
By Mail: Mail the “Complaint/Grievance Request Form” or a letter to the following
address:
UPMC Community HealthChoices
Complaints, Grievances, and Appeals
P.O. Box 2939
Pittsburgh, PA 15230-2939
How long will it take to decide my Complaint or Grievance?
UPMC Community HealthChoices will send you a written notice of the decision on your
Complaint or Grievance within 30 days from when UPMC Community HealthChoices received
your Complaint or Grievance.
How do I ask for an early decision on my Complaint or Grievance?
If you or your doctor or dentist thinks waiting 30 days for a decision could harm your health,
call UPMC Community HealthChoices at 1-844-833-0523 (TTY: 711) to ask for an early
decision on your Complaint or Grievance.
You should also ask your doctor or dentist to fax a signed letter to 412-454-7920 within 72
hours of when you asked for an early decision on your Complaint or Grievance. The letter
should explain why waiting 30 days for a decision could harm your health.
UPMC Community HealthChoices will tell you the decision within 48 hours from when UPMC
Community HealthChoices gets your doctor’s letter, or within 72 hours from when you asked
UPMC Community HealthChoices for an early decision, whichever is sooner, unless you ask](https://image.slidesharecdn.com/gravenstein-appeal-packetclean-221231204008-40d4c793/75/Appeal-Packet-8-2048.jpg)
![CHC PARTIAL APPROVAL LTR N2 UM 20CHC1199233
[LTR-BD]
UPMC Community HealthChoices to take more time to decide your Complaint or Grievance.
You can ask UPMC Community HealthChoices to take up to 14 more days to decide your
Complaint or Grievance.
What happens after I file my Complaint or Grievance?
UPMC Community HealthChoices will hold a meeting within 30 days of when you filed your
Complaint or Grievance to review your Complaint or Grievance. You may attend the meeting
either in person, by phone, or by videoconference. You may also bring a family member,
friend, or lawyer to help you during the meeting.
How can I get help with my Complaint or Grievance?
If you need help filing a Complaint or Grievance, you can call UPMC Community
HealthChoices at 1-844-833-0523 (TTY: 711). Representatives are available 24 hours a day, 7
days a week.
To ask for free legal help with your Complaint or Grievance, contact:
Pennsylvania Health Law Project at 1-800-274-3258 (www.phlp.org); or
Pennsylvania Legal Aid Network at 1-800-322-7572 (www.palegalaid.net)
Sincerely,
UPMC Community HealthChoices
cc:](https://image.slidesharecdn.com/gravenstein-appeal-packetclean-221231204008-40d4c793/75/Appeal-Packet-9-2048.jpg)



















































