
Recommended
More Related Content
Similar to Examen de macros para el consejo de patologos
Similar to Examen de macros para el consejo de patologos (20)
Recently uploaded
Recently uploaded (20)
Examen de macros para el consejo de patologos
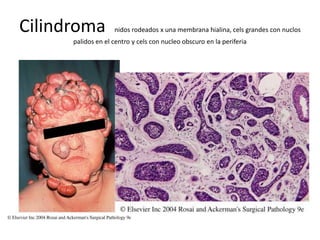
- 1. Cilindroma nidos rodeados x una membrana hialina, cels grandes con nuclos palidos en el centro y cels con nucleo obscuro en la periferia
- 3. LA MALFORMACIÓN ADENOMATOIDE QUÍSTICA es una alteración pulmonar congénita poco frecuente (1 de 25 a 30 mil embarazos) representa el 25% de malformaciones pulmonares congénitas y el 95% de las enfermedades quísticas pulmonares y consiste en una proliferación anormal de elementos mesenquimales pulmonares, conteniendo epitelio respiratorio de los bronquiolos terminales con formación de estructuras adenomatosas y quistes. Su presentación clínica es en la edad neonatal o primera infancia; el diagnóstico prenatal de esta anomalía está seguido por un pronóstico bueno cuando no se presentan signos de "distress" fetal severo (. No tiene predilección por sexo. Usualmente compromete un lóbulo pulmonar (inferior). Las paredes de las lesiones están constituidas por fibras elásticas y músculo liso, pocas veces se identifica la presencia de glándulas mucosas y cartílagos .
- 4. • There is both cytoplasmic and nuclear staining for S-100 protei
- 5. • Well-differentiated chondrosarcoma. The tumor has a distinctly lobulated quality The tumor retains a lobulated appearance, but nuclear atypicality is obvious. Chondrosarcoma.
- 6. Mesenchymal chondrosarcoma: shows an island of well-differentiated cartilage in the center
- 8. Siringoma En mujeres adolescentes Pápulas múltiples sobre los parpados y las mejillas Esferulosis colagena
- 9. Well-differentiated (Meyer’s type I) Sertoli–Leydig cell tumor
- 10. • Poorly differentiated (Meyer’s type III) Sertoli–Leydig cell tumo • ntermediate (Meyer’s type II) Sertoli–Leydig cell tumor
- 11. Células gigantes Café claro o café rojizo con trabeculas engrosadas. Engrosamiento de corteza. Areas de hemorragia • Specimen from giant cell tumor of bone fixed in formalin and embedded in paraffin, stained for acid phosphatase (Duray’s technique)
- 12. Osteosarcoma • Destructivo. • Hemorrágico • Necrótico • Quistico
- 14. Osteosarcoma. The malignant bone is more basophilic and has more irregular borders than the preexisting bone trabeculae
- 15. Microscopic appearance of osteosarcoma showing characteristic basophilic thin trabeculae of neoplastic bone with an appearance that is reminiscent of fungal hyphae
- 17. Juxtacortical osteosarcoma. Moderately atypical spindle tumor cells grow between irregularly shaped bone trabeculae
- 18. NEVO DE SPITZ, Ortoqueratosis 2)cels epiteliales o fusiformes,cuerpos de kamino y se distinguen vertices entre cels malignas y queratinocitos
- 19. RETROPERITONEAL WELL-DIFFERENTIATED LIPOSARCOMA (atypical lipomatous tumor) accompanied by foci of dedifferentiation, manifested by the solid whitish areas
- 20. Quistes teca _luteinizantes • • En embarazos. • En mola. • Coriocarcioma. • Son comunes en estas enfermedades.
- 21. CISTADENOCARCINOMA seroso (ovario) areás de hemorragia y necrosis
- 22. DESPUES DE LA PUBERTAD. FIBROMA.
- 23. • tecoma. • 65%despues de la menopausia, • Rojo oloeoso la grasa • Tincion de plata para las fibras de reticulina,
- 24. • Brenner. • Se diferencian de los fibromas o tecomas x q TIENEN QUISTES PEQUEÑITOS. • Unilaterales. • 40 años. • Hiperestrogenismo. • Sangrado.
- 25. BRENER MALIGNO
- 26. Sarcoma endometrial de bajo y alto grado 45 a. Vimentina es la regla. CD10+/ H Caldesmon (–) • Cels dispuestas concentricamente alredededor de las arterias espirales.
- 27. FILODES. Areás de necrosis degeneracion quistica y hemorragia, foleas
- 30. SEMINOMA
- 32. ESTRONGILOIDES
- 33. Fig. 18.72 Embryonal carcinoma showing solid nodular , MAL DELIMITADO Y PUNTEADO DE FOCOS DE hemorragia y necrosis siempre. • Diferenciación temprana e estructuras embrionarias . • Las cels son + anaplasicas q seminom,+ pleomorficas, y muchos nucléolos. . Ck 19,+ CD30 +(Ki.1) NUNCA 117 x eso se hace el dif con seminoma
- 34. appearance of pure yolk sac tumor in an infan, NO ES ENCAPSULADO
- 35. LEYDING benigno. COLOR CAFÉ pardo dorado CARACTERISTICOS , EN CRIPTORQUIDIA, KLINERFELTER, producen ESTROGENOS O ANDROGENOS o esteroides • Ginecomastia puede ser 1 sintoma en adultos. • Precosidad sexual en niños. • 10%mets • Citoplasmo-lipidos, vacuolas, lipofuschina • en 25% de los tumores Cristaloides REINKE en forma baston
- 37. Fibrosis hepática congénita (autosimico resecivo) Los espacios portales estan unidos x puentes fibrosos. Tractos portales inmaduros, no hay inflamacion
- 39. Primary biliary cirrhosis, stage 3. The picture shows portal–portal septal fibrosis (septal stage 3), portal inflammation with lymphoid aggregate, absence of interlobular bile duct (ductopenia), and cholate stasis in periportal and periseptal parenchyma. (H&E
- 40. Enfermedad poliquistica autosomica renal, no tiene caracteristicas embrionarias lo hace dif a displasia
- 44. Cambios minimos*IgM-C3 x lo regular la inmofluoresencia es (-)
- 45. focal and segmental glomerulosclerosis. One of the glomeruli shows segmental sclerosis, while the other appears unremarkable. Tubular atrophy is also seen.IgM-C3
- 46. Glomerulonefritis membranosa(IgG-C3) Depositos granular pared capilar Silver preparation showing spike formation along the thickened basement membrane
- 47. Early diffuse diabetic glomerulosclerosis showing a mild increase in mesangial matrix and thickened capillary walls. The arteriole shows the typical hyaline appearance of an insudative lesion.IgG
- 48. Glomerulus with prominent mesangial and vascular deposition of amyloid, notese la ausencia de esclerosis y vasos q la diferencian con Diabetes.
- 50. Type I membranoproliferative glomerulonephritis. There is an increase in lobulation, diffuse mesangial hypercellularity, and thickening of the capillary walls
- 51. Silver preparation showing marked increase in mesangial matrix in the centrolobular areas with peripheral extension of the mesangium producing a double contour pattern in the loops IgG-C3
- 52. Mesangial enlargement with increase in mesangial matrix and mesangial hypercellularity in IgA nephropath
- 53. Acute postinfectious glomerulonephritis with intracapillary proliferation and crescent formation
- 56. LUPUS IV asas de alambre.Es la + + fte 30-65% de la bx
- 57. LP V
- 58. Fibrinoid necrosis involving two medium-sized arteries in polyarteritis nodosa
- 61. Wilms’ tumor. A, Low-power microscopic view showing a combination of blastema, stroma, epithelial tubular formation, and immature glomerul
- 67. .121 Collecting duct carcinoma showing branching tubules lined by cuboidal cells
- 73. Cryptococcus neoformans by their mucicarmine-stained capsules
- 74. Toxoplasmosis. Minute, basophilic structures representing bradyzoites fill a protozoal pseudocyst lying among infiltrating lymphocytes, plasma cells, and macrophage BRADIZOITO
- 86. RETINOBLASTOMA
- 90. LOBULO TEMPORAL. NINOS GRANDES ADULTOS TEMPRANOPleomorphic xanthoastrocytoma. Spindle and giant cells, including bizarre multinucleated forms, combine to give this relatively indolent neoplasm a most disturbing appearance. Note hyaline, granular, and vacuolar cytoplasmic alterations, the last attesting to lipid accumulation
- 91. Oligodendroglioma. The bright signal abnormalities seen in this nonenhanced CT study of a large right cerebral oligodendroglioma represent foci of intratumoral calcification. While evidenced by only a minority of oligodendroglial neoplasms, linear or plate-like calcifications of this sort are most suggestive of the diagnosis
- 92. Granulosa cell tumor with an entirely cystic gross appearance
- 95. Renal cell carcinoma of papillary type. Note the neutrophilic infiltratio Other gross appearances of renal cell carcinoma
- 97. Subependymal giant cell astrocytma (MASA INTRAVENTRICULAR). 2-3 D.. features of tuberous sclerosis..TRIADA(EPILEPSIA, REARDO MENTAL, ADENOMA SEBASEO.
- 98. Choroid plexus papilloma. Note the characteristically bosselated surface of this surgically resected example. Deprived of its blood supply, the tumor tissue loses its normally hyperemic appearance and may assume a tan or golden hue
- 99. Medulloblastoma. The classic medulloblastoma is a highly cellular neoplasm composed of diminutive, undifferentiated-looking elements possessed of little definable cytoplasm and prone to nuclear moldin
- 100. Meningioma. The broad dural base depicted here is characteristi
- 102. Ependymoma. The cytoplasmic processes of ependymal tumor cells condense about blood vessels to form pseudorosettes GLIOMA MAS FRECUENTE DEL CORDON ESPINAL. EN NIÑOS FOSA POSTERIOR (0-16) 30-40. QX Y RX
- 103. >20 A.Ependymoma MIXOPAILAR. Characteristic of this entity is the huddling of small tumor cells in an expansive fibrillar meshwork. Microcystic changes commonly round out the histologic pictur, CONO MEDULAR Y COLA DE CABALLO. INCONTINENCIA URINARIA-FECAL
- 104. CORDOMA (SACROCOCCIGEO) CELS FISALIFERAS
- 108. Juvenile granulosa cell tumor. (B) the tumor cells are seen lack the coffee- bean nuclei seen in the adult type
- 109. Juvenile granulosa cell tumor. The follicle-like spaces seen on low-power examination (A) are a common feature of this neoplasm
- 112. Sx ewing.FEMUR-PELVIS 5-20A4 Gross appearance of Ewing’s sarcoma. It has a typical ill-defined quality, with extensive involvement of medulla and cortex associated with elevation of periosteum
- 113. Ewing’s sarcoma of fibula. Growth is ill defined and accompanied by a prominent periosteal reaction
- 114. Low- and high-power appearance of myxoid liposarcoma
- 116. Rosai–Dorfman disease. Low-power view showing massive distension of the sinuses by the histiocytic infiltrate
- 117. Rosai–Dorfman disease. • A, Oil red O stain showing abundant neutral lipid in the cytoplasm of the histiocytes • Strong immunoreactivity of the sinus histiocytes for S-100 protein in Rosai Dorfman disease
- 120. A and B, Lymph node involvement by Langerhans’ cell histiocytosis. A, The infiltrate has a predominantly sinusal distributionB, High-power view showing mononuclear and multinucleated Langerhans’ cells. There are also numerous eosinophils.
- 121. Immunoreactivity of the cells of Langerhans’ cell histiocytosis for langerin
- 123. Mantle cell lymphoma surrounding a small residual germinal cente
- 124. Immunoreactivity for cyclin D1 in mantle zone lymphom
- 126. Gross appearance of lymph nodes involved by non-Hodgkin’s lymphoma of diffuse large B-cell type. The nodes are enlarged and show a homogeneous tan cut surface
- 127. Medium and high-power views of diffuse large B-cell lymphoma of large cleaved typ
- 129. Medium and high-power views of diffuse large B-cell lymphoma of immunoblastic typ
- 132. Sclerosing adenosis. MAMA B , Medium-power view. Note the spindle shape of the proliferating cells in the center of the lobule and the fibrillary quality of the cytoplasm, indicative of myoepithelial nature
- 133. Benign “perineurial invasion” in a breast lesion that had elsewhere the typical features of sclerosing adenosi
- 134. Prototypical invasive ductal carcinom
- 136. Two views of low-grade phylloides tumor, showing cleft-like spaces and concentration of tumor cells beneath the epithelium
- 137. Phylloides tumor with adipose tissue differentiation of the neoplastic stromal component
- 139. malignant mixed müllerian tumor of ovary. The neoplasms are large, variegated, solid and cystic, with hemorrhagic and necrotic areas
- 140. , Malignant mixed müllerian tumor of ovary. The tumor shown in A is of the so-called “homologous type,” whereas the others exhibit heterologous foci in the form of bone and cartilage (B) or skeletal muscle (C
- 155. Hiperplasia higado