Recommended

Recommended
More Related Content
What's hot
What's hot (18)
Similar to Esacaide 931
Similar to Esacaide 931 (20)
Recently uploaded
Recently uploaded (20)
Esacaide 931
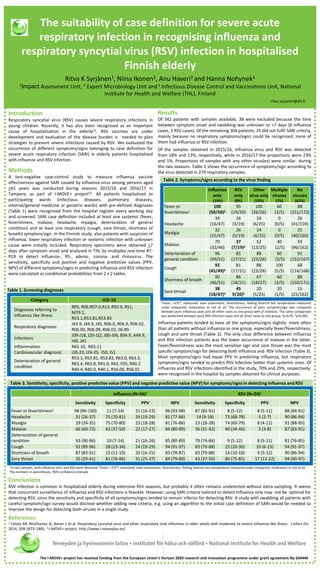
- 1. Results Of 342 patients with samples available, 38 were excluded because the time between symptom onset and swabbing was unknown or >7 days (6 influenza cases, 3 RSV cases). Of the remaining 304 patients, 25 did not fulfil SARI criteria, mainly because no respiratory symptoms/signs could be recognised; none of them had influenza or RSV infection. Of the samples obtained in 2015/16, influenza virus and RSV was detected from 18% and 13%, respectively, while in 2016/17 the proportions were 23% and 1%. Proportions of samples with any other virus(es) were similar during the two seasons. Table 2 shows the occurrence of symptoms/sign according to the virus detected in 279 respiratory samples. 1Fever, >37C⁰, measured, even anamnestic; feverishness, feeling feverish but temperature measured under antipyretic medication or not at all. The occurrence of each symptom/sign was compared between pure influenza cases and all other cases as one group with χ2 statistics. The same comparison was performed between pure RSV infection cases and all other cases as one group; 2p<0.05, 3p<0.005. Influenza patients tended to have all the symptoms/signs slightly more often than all patients without influenza as one group, especially fever/feverishness, cough and sore throat (Table 2). The only clear difference between influenza and RSV infection patients was the lower occurrence of malaise in the latter. Fever/feverishness was the most sensitive sign and sore throat was the most specific symptom/sign for detecting both influenza and RSV infection (Table 3). Most symptoms/signs had equal PPV in predicting influenza, but respiratory symptoms/signs tended to predict RSV infection better than systemic ones. Of influenza and RSV infections identified in the study, 70% and 25%, respectively, were recognised in the hospital by samples obtained for clinical purposes. The suitability of case definition for severe acute respiratory infection in recognising influenza and respiratory syncytial virus (RSV) infection in hospitalised Finnish elderly Ritva K Syrjänen1, Niina Ikonen2, Anu Haveri2 and Hanna Nohynek3 1Impact Assessment Unit, 2 Expert Microbiology Unit and3 Infectious Disease Control and Vaccinations Unit, National Institute for Health and Welfare (THL), Finland ritva.syrjanen@thl.fi Introduction Respiratory syncytial virus (RSV) causes severe respiratory infections in young children. Recently, it has also been recognised as an important cause of hospitalisation in the elderly(1). RSV vaccines are under development and evaluation of the disease burden is needed to plan strategies to prevent severe infections caused by RSV. We evaluated the occurrence of different symptoms/signs belonging to case definition for severe acute respiratory infection (SARI) in elderly patients hospitalised with influenza and RSV infection. Methods A test-negative case-control study to measure influenza vaccine effectiveness against SARI caused by influenza virus among persons aged >65 years was conducted during seasons 2015/16 and 2016/17 in Tampere, as part of I-MOVE+ project(2). All patients hospitalised to participating wards (infectious diseases, pulmonary diseases, internal/general medicine or geriatric wards) with pre-defined diagnoses (Table 1) were recognised from the hospital register every working day and screened. SARI case definition included at least one systemic (fever, feverishness, malaise, headache, myalgia, deterioration of general condition) and at least one respiratory (cough, sore throat, shortness of breath) symptom/sign. In the Finnish study, also patients with suspicion of influenza, lower respiratory infection or systemic infection with unknown cause were initially included. Respiratory specimens were obtained <7 days after symptom onset and analysed in THL by multiplex real-time RT- PCR to detect influenza-, RS-, adeno-, corona- and rhinovirus. The sensitivity, specificity and positive and negative predictive values (PPV, NPV) of different symptoms/signs in predicting influenza and RSV infection were calculated as conditional probabilities from 2 x 2 tables. Table 1. Screening diagnoses References 1. Falsey AR, McElhaney JE, Beran J, et al. Respiratory syncytial virus and other respiratory viral infections in older adults with moderate to severe influenza-like illness. J Infect Dis 2014; 209:1873–1881. 2.I-MOVE+ project, http://www.i-moveplus.eu/ Table 2. Symptoms/signs according to the virus finding Table 3. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for symptoms/signs in detecting influenza and RSV Influenza only (19%) RSV only (8%) Other virus only (10%) Multiple viruses (2%) No viruses (62%) Fever or feverishness1 100 (50/50)2 95 (19/20) 100 (26/26) 60 (3/5) 88 (151/172) Headache 34 (16/47) 16 (3/19) 24 (6/25) 0 (0/5) 26 (41/159) Myalgia 32 (15/47) 26 (5/19) 24 (6/25) 0 (0/5) 25 (40/160) Malaise 70 (32/46) 37 (7/19)2 52 (13/25) 40 (2/5) 59 (96/162) Deterioration of general condition 96 (49/51) 81 (17/21) 88 (23/26) 60 (3/5) 91 (152/167) Cough 92 (45/49)3 81 (17/21) 88 (23/26) 100 (5/5) 68 (114/168) Shortness of breath 90 (46/51) 86 (18/21) 67 (18/27) 60 (3/5) 88 (150/171) Sore throat 38 (18/47)3 45 9/20)2 20 (5/25) 20 (1/5) 15 (25/162) Category ICD-10 Diagnoses referring to influenza like illness R05, R06,R07.0,R13, R50.9, R51, M79.1, R53.1,R53.81,R53.83 Respiratory diagnoses J43.9, J44.9, J45, R06.0, R06.9, R06.02, R06.00, R06.09, R06.03, 06.89 Infections J09-J18, J20-J22, J00-J06, B34.9, A49.9, J40, J41 Inflammation R65.10, R65.11 Cardiovascular diagnosis I20-23, I24-25, I50, I51 Deterioration of general condition R53.1, R53.81, R53.83, R63.0, R63.3, R63.4, R63.8, R41.0, R42, F05, R40.2 R40.4, R40.0, R40.1, R56.00, R56.01 Influenza (N=56)1 RSV (N=24)1 Sensitivity Specificity PPV NPV Sensitivity Specificity PPV NPV Fever or feverishness2 98 (96-100) 11 (7-14) 21 (16-23) 96 (93-98) 87 (83-91) 8 (5-12) 8 (5-11) 88 (84-91) Headache 31 (26-37) 75 (70-81) 24 (19-29) 81 (77-86) 14 (9-18) 73 (68-78) 5 (2-7) 90 (86-94) Myalgia 29 (24-35) 75 (70-80) 23 (18-28) 81 (76-86) 23 (18-28) 74 (69-79) 8 (4-11) 91 (88-95) Malaise 66 (60-72) 43 (37-50) 22 (17-27) 84 (80-89) 36 (31-42) 40 (34-46) 5 (3-8) 87 (83-91) Deterioration of general condition 93 (90-96) 10 (7-14) 21 (16-26) 85 (80-89) 79 (74-84) 9 (5-12) 8 (5-11) 81 (76-85) Cough 92 (89-96) 28 (23-34) 24 (19-29) 94 (91-97) 83 (79-88) 25 (20-30) 10 (6-13) 94 (91-97) Shortness of breath 87 (83-91) 15 (11-19) 20 (16-25) 83 (78-87) 83 (79-88) 14 (10-18) 9 (5-12) 90 (86-94) Sore throat 35 (29-41) 81 (76-86) 31 (25-37) 84 (79-88) 43 (37-50) 80 (75-85) 17 (13-22) 94 (90-97) 1In two samples, both influenza virus and RSV were detected. 2Fever, >37C⁰, measured, even anamnestic; feverishness, feeling feverish but temperature measured under antipyretic medication or not at all. The numbers in parentheses, 95% confidence intervals The I-MOVE+ project has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 634446 Conclusions RSV infection is common in hospitalised elderly during extensive RSV seasons, but probably it often remains undetected without extra sampling. It seems that concurrent surveillance of influenza and RSV infections is feasible. However, using SARI criteria tailored to detect influenza only may not be optimal for detecting RSV, since the sensitivity and specificity of all symptoms/signs tended to remain inferior for detecting RSV. A study with swabbing all patients with careful symptom/sign survey would disclose whether adding new criteria, e.g. using an algorithm to the initial case definition of SARI would be needed to improve the design for detecting both viruses in a single study.