Ectopic Pregnancy: A trainee's guide to making the right call.
1.
Stephanie N. Histed,MD1
Monica Deshmukh, MD2
Rinat Masamed, MD1
Cecilia M. Jude, MD2
Shaden Mohammad, MD2
Maitraya K. Patel, MD1,2
Ectopic Pregnancy: A Trainee’s
Guide to Making the Right Call
2.
Overview
Ectopic pregnancy refersto a pregnancy implanted outside the normal intrauterine
position.
Background
Overall prevalence of ectopic
pregnancy is approximately 2% in the
United States.
In women with first trimester vaginal
bleeding and/or pain, the prevalence
of ectopic pregnancy has been
reported to be up to 18%.
It is the most common cause of first
trimester maternal death.
Early detection can avoid the need for
surgery.
The radiology trainee is often at the
front line for initial evaluation and
affects diagnosis and treatment.
Topics covered
Clinical and laboratory features
Normal early pregnancy
Case studies by ectopic location
Treatment
3.
Learning Objectives
Key concepts
Transvaginal ultrasonography (US),
with findings interpreted in
conjunction with serum human
chorionic gonadotropin (hCG) values,
is the key test to diagnose ectopic
pregnancy.
Normal physiology and ectopic
pregnancies with their expected
radiologic findings are important for
the radiology trainee to understand.
Accurate diagnosis as early as
possible is essential to help initiate
treatment, which may include local or
systemic medications or surgery.
Learning objectives
Review the normal process of
fertilization, implantation, and
expected US findings for a normal
intrauterine pregnancy (IUP).
Describe the possible locations where
an ectopic pregnancy may be found.
Fallopian tubal, cervical, ovarian,
interstitial, cornual, cesarean
section scar, heterotopic, and
abdominal
Discuss treatment options for ectopic
pregnancy, including first-line therapy
and contraindications.
4.
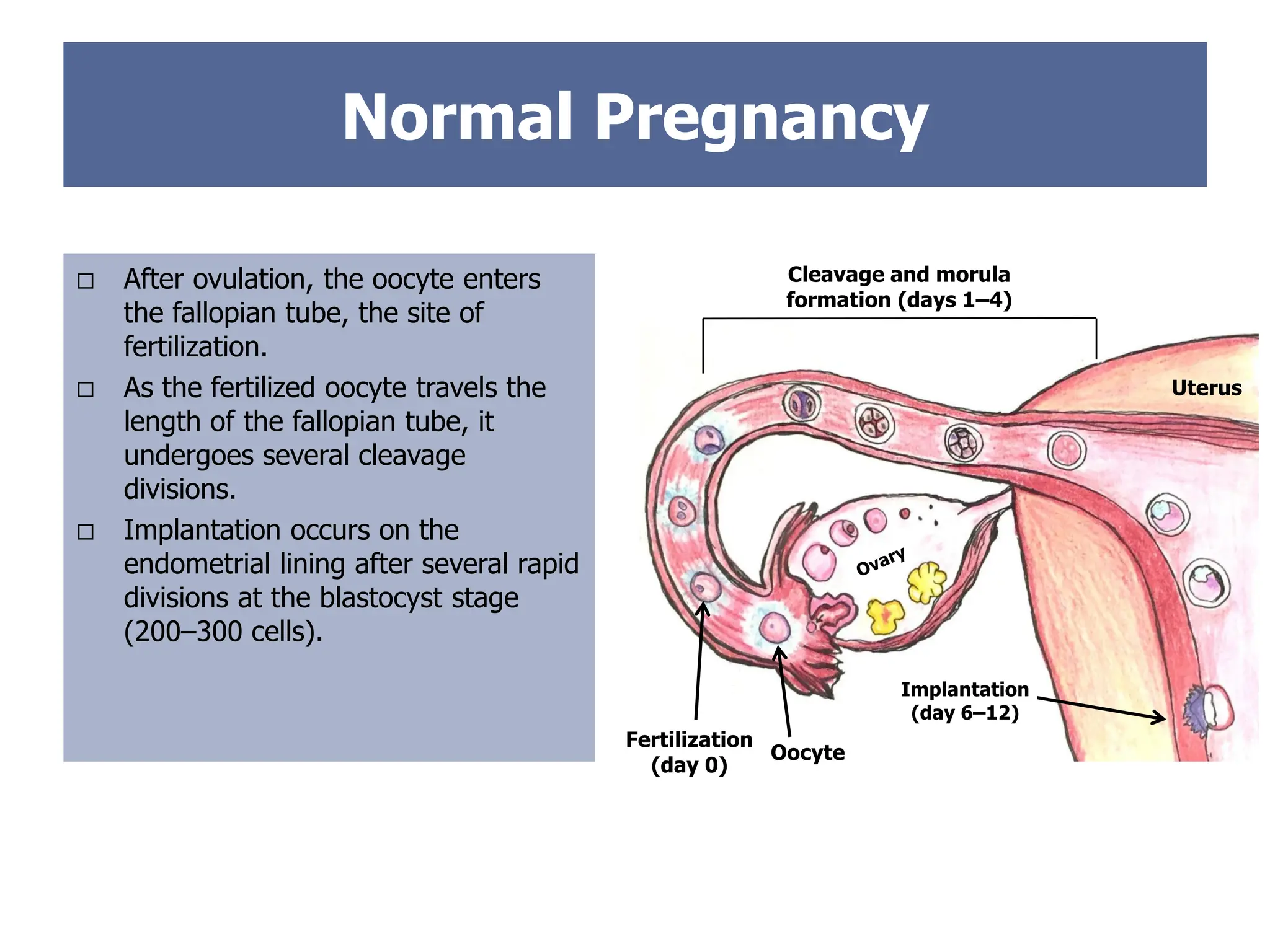
Normal Pregnancy
Afterovulation, the oocyte enters
the fallopian tube, the site of
fertilization.
As the fertilized oocyte travels the
length of the fallopian tube, it
undergoes several cleavage
divisions.
Implantation occurs on the
endometrial lining after several rapid
divisions at the blastocyst stage
(200–300 cells).
Fertilization
(day 0)
Uterus
Cleavage and morula
formation (days 1–4)
Implantation
(day 6–12)
Oocyte
5.
First Trimester TransvaginalUS
Findings
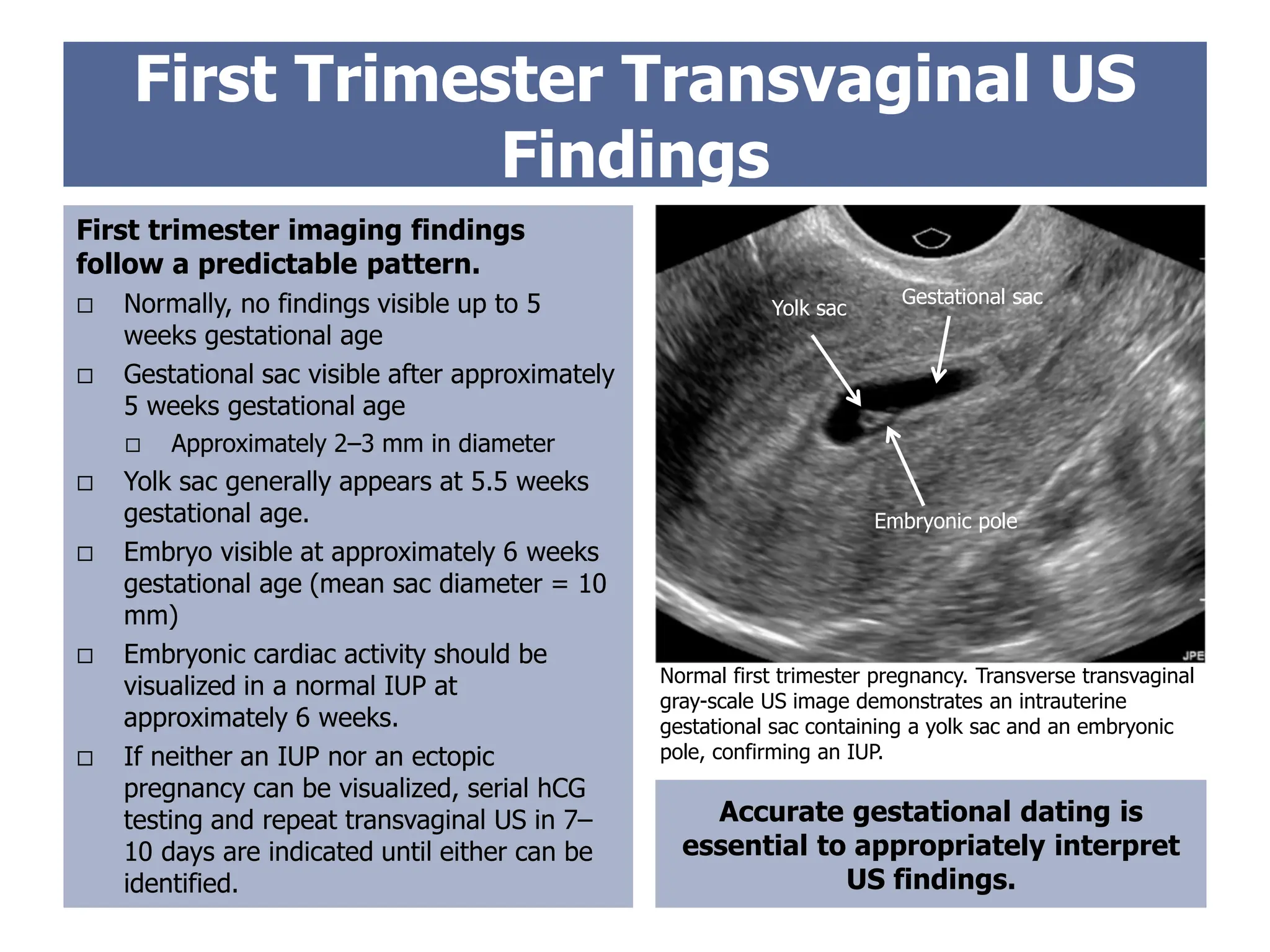
First trimester imaging findings
follow a predictable pattern.
Normally, no findings visible up to 5
weeks gestational age
Gestational sac visible after approximately
5 weeks gestational age
Approximately 2–3 mm in diameter
Yolk sac generally appears at 5.5 weeks
gestational age.
Embryo visible at approximately 6 weeks
gestational age (mean sac diameter = 10
mm)
Embryonic cardiac activity should be
visualized in a normal IUP at
approximately 6 weeks.
If neither an IUP nor an ectopic
pregnancy can be visualized, serial hCG
testing and repeat transvaginal US in 7–
10 days are indicated until either can be
identified.
Accurate gestational dating is
essential to appropriately interpret
US findings.
Gestational sac
Yolk sac
Embryonic pole
Normal first trimester pregnancy. Transverse transvaginal
gray-scale US image demonstrates an intrauterine
gestational sac containing a yolk sac and an embryonic
pole, confirming an IUP.
6.
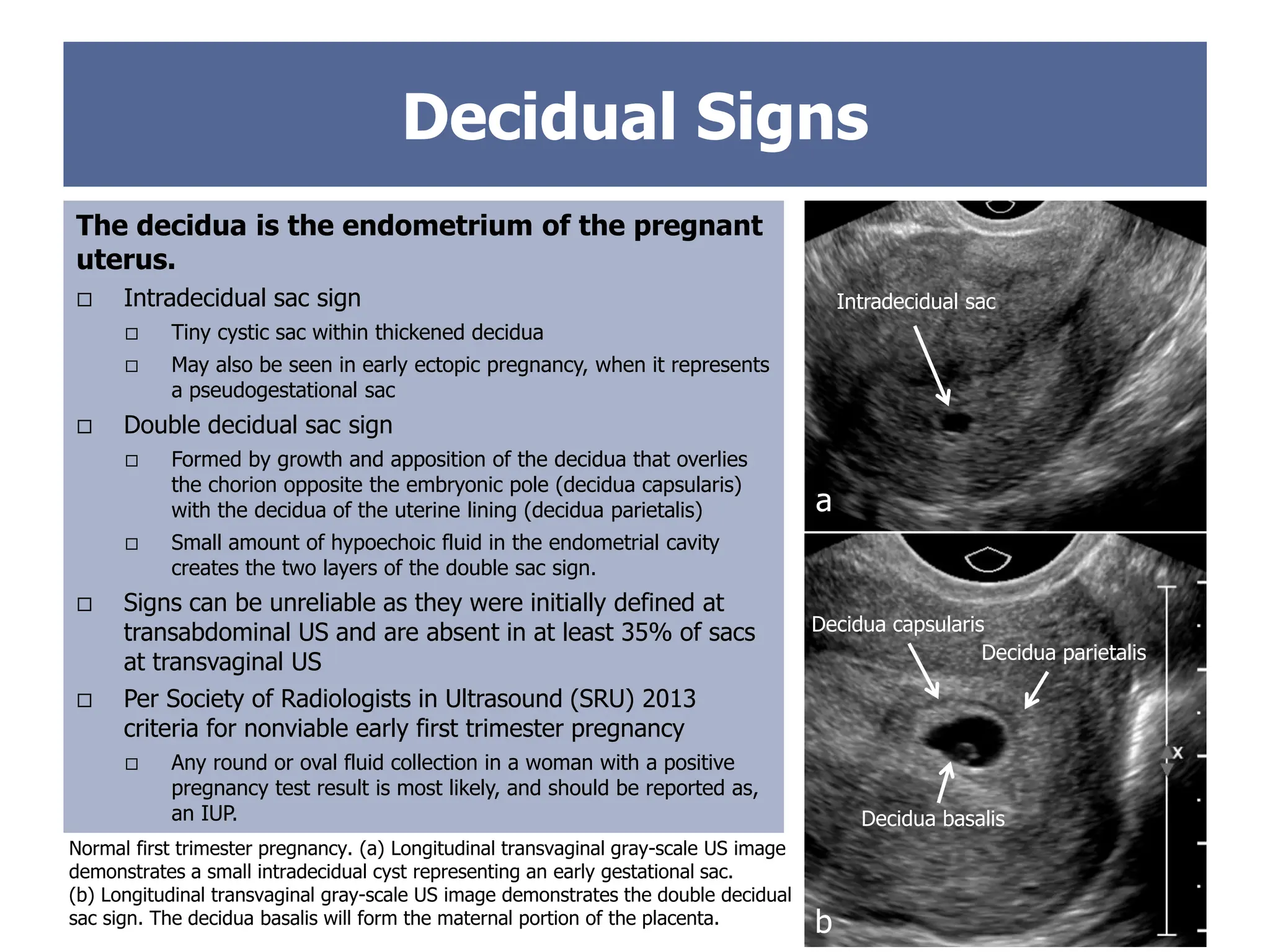
The decidua isthe endometrium of the pregnant
uterus.
Intradecidual sac sign
Tiny cystic sac within thickened decidua
May also be seen in early ectopic pregnancy, when it represents
a pseudogestational sac
Double decidual sac sign
Formed by growth and apposition of the decidua that overlies
the chorion opposite the embryonic pole (decidua capsularis)
with the decidua of the uterine lining (decidua parietalis)
Small amount of hypoechoic fluid in the endometrial cavity
creates the two layers of the double sac sign.
Signs can be unreliable as they were initially defined at
transabdominal US and are absent in at least 35% of sacs
at transvaginal US
Per Society of Radiologists in Ultrasound (SRU) 2013
criteria for nonviable early first trimester pregnancy
Any round or oval fluid collection in a woman with a positive
pregnancy test result is most likely, and should be reported as,
an IUP.
Normal first trimester pregnancy. (a) Longitudinal transvaginal gray-scale US image
demonstrates a small intradecidual cyst representing an early gestational sac.
(b) Longitudinal transvaginal gray-scale US image demonstrates the double decidual
sac sign. The decidua basalis will form the maternal portion of the placenta.
a
Intradecidual sac
Decidual Signs
b
Decidua basalis
Decidua capsularis
Decidua parietalis
7.
First Trimester Pregnancy:
Nonviability
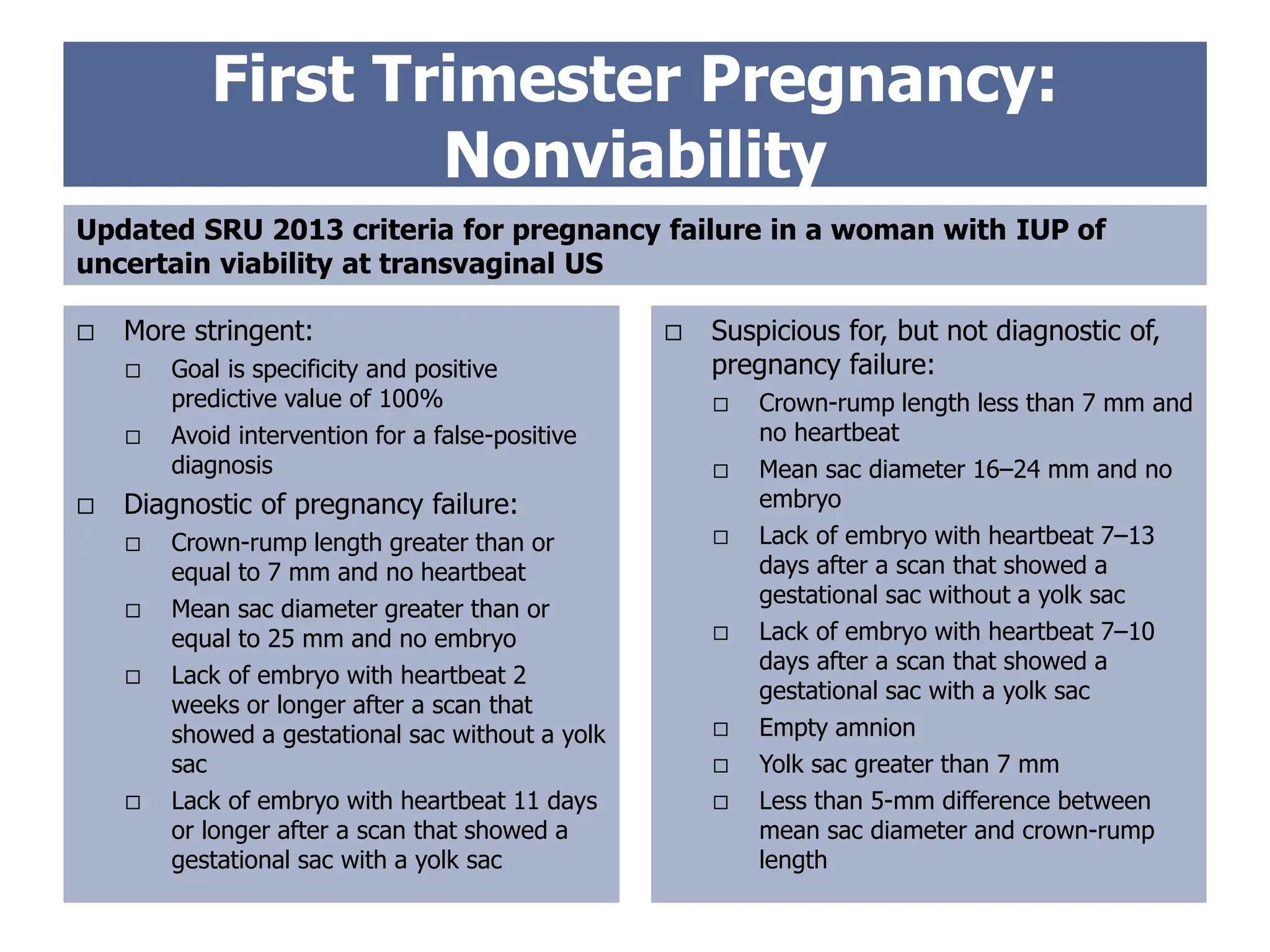
More stringent:
Goal is specificity and positive
predictive value of 100%
Avoid intervention for a false-positive
diagnosis
Diagnostic of pregnancy failure:
Crown-rump length greater than or
equal to 7 mm and no heartbeat
Mean sac diameter greater than or
equal to 25 mm and no embryo
Lack of embryo with heartbeat 2
weeks or longer after a scan that
showed a gestational sac without a yolk
sac
Lack of embryo with heartbeat 11 days
or longer after a scan that showed a
gestational sac with a yolk sac
Updated SRU 2013 criteria for pregnancy failure in a woman with IUP of
uncertain viability at transvaginal US
Suspicious for, but not diagnostic of,
pregnancy failure:
Crown-rump length less than 7 mm and
no heartbeat
Mean sac diameter 16–24 mm and no
embryo
Lack of embryo with heartbeat 7–13
days after a scan that showed a
gestational sac without a yolk sac
Lack of embryo with heartbeat 7–10
days after a scan that showed a
gestational sac with a yolk sac
Empty amnion
Yolk sac greater than 7 mm
Less than 5-mm difference between
mean sac diameter and crown-rump
length
8.
Clinical Evaluation
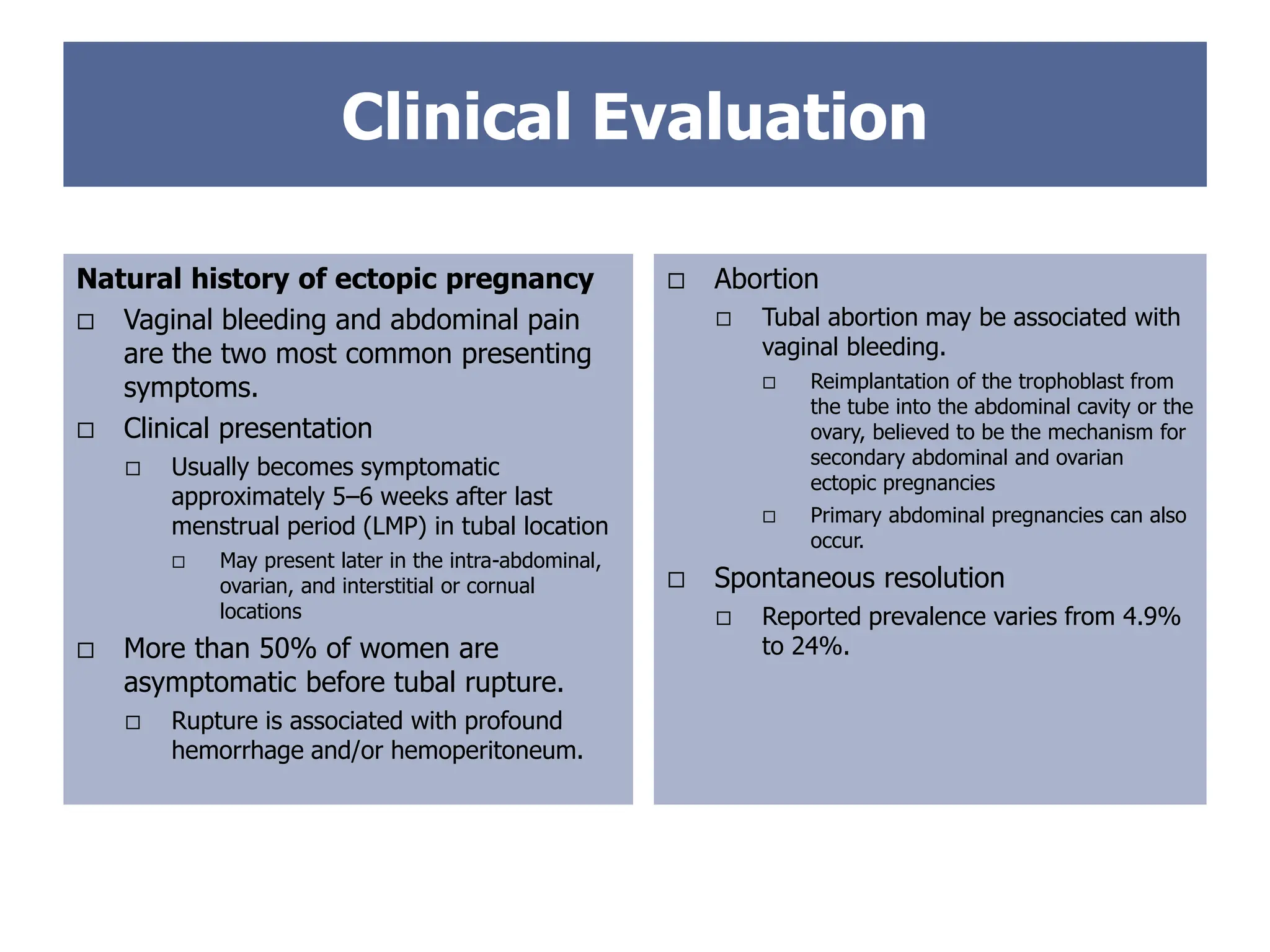
Abortion
Tubal abortion may be associated with
vaginal bleeding.
Reimplantation of the trophoblast from
the tube into the abdominal cavity or the
ovary, believed to be the mechanism for
secondary abdominal and ovarian
ectopic pregnancies
Primary abdominal pregnancies can also
occur.
Spontaneous resolution
Reported prevalence varies from 4.9%
to 24%.
Natural history of ectopic pregnancy
Vaginal bleeding and abdominal pain
are the two most common presenting
symptoms.
Clinical presentation
Usually becomes symptomatic
approximately 5–6 weeks after last
menstrual period (LMP) in tubal location
May present later in the intra-abdominal,
ovarian, and interstitial or cornual
locations
More than 50% of women are
asymptomatic before tubal rupture.
Rupture is associated with profound
hemorrhage and/or hemoperitoneum.
9.
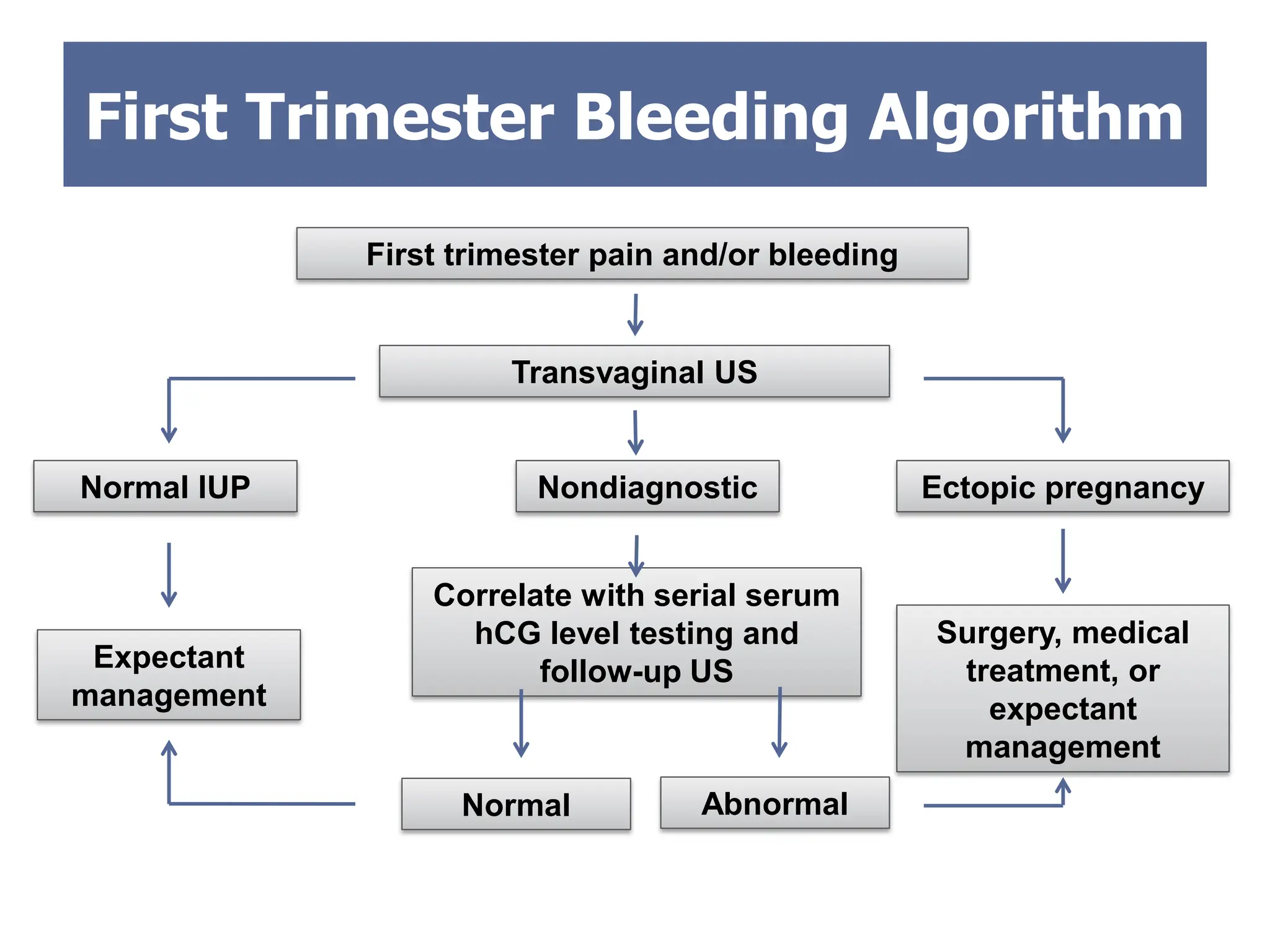
First Trimester BleedingAlgorithm
Transvaginal US
First trimester pain and/or bleeding
Correlate with serial serum
hCG level testing and
follow-up US
Ectopic pregnancy
Normal IUP
Expectant
management
Surgery, medical
treatment, or
expectant
management
Nondiagnostic
Abnormal
Normal
10.
Serum hCG Valuesin Pregnancy
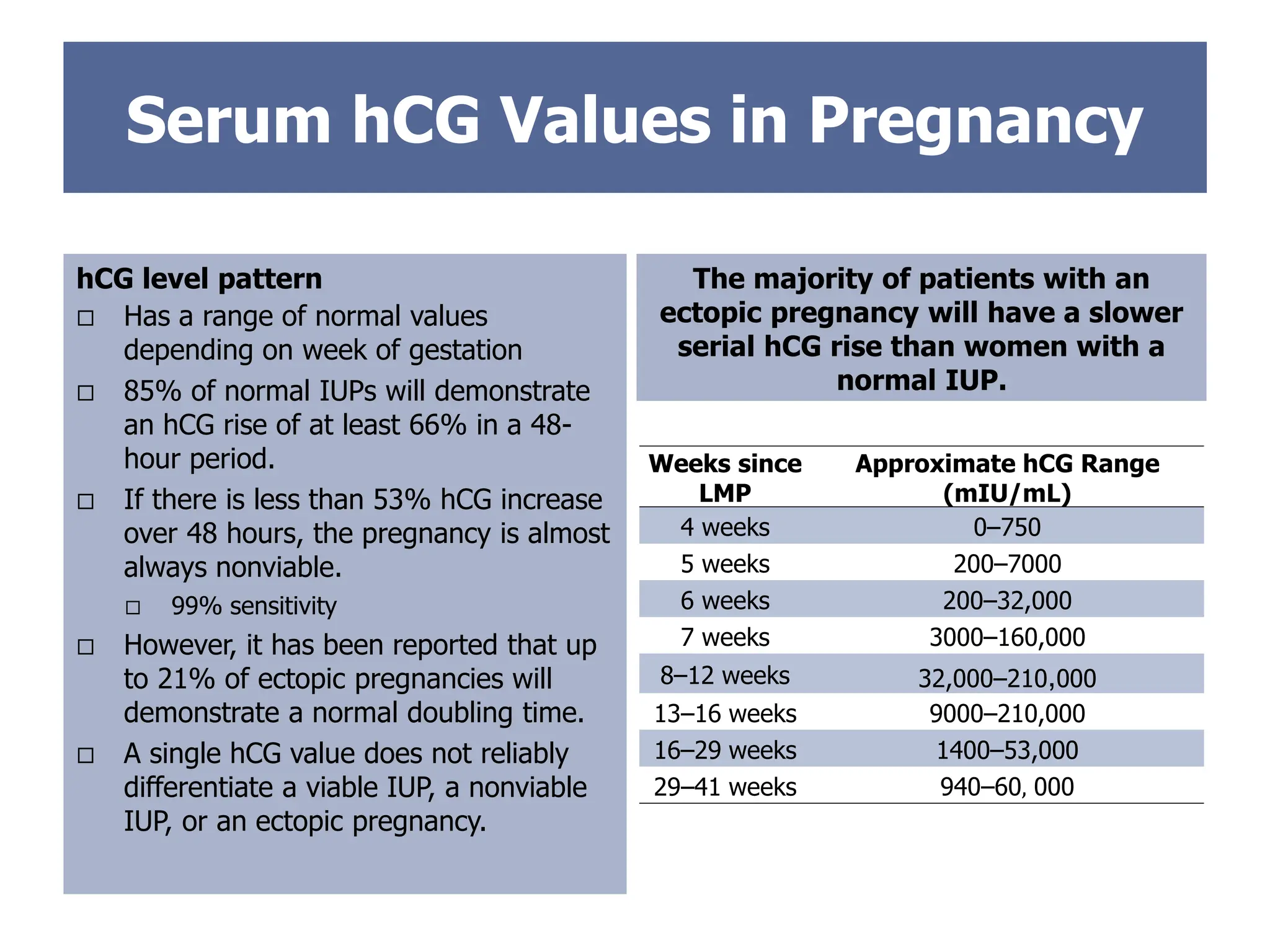
hCG level pattern
Has a range of normal values
depending on week of gestation
85% of normal IUPs will demonstrate
an hCG rise of at least 66% in a 48-
hour period.
If there is less than 53% hCG increase
over 48 hours, the pregnancy is almost
always nonviable.
99% sensitivity
However, it has been reported that up
to 21% of ectopic pregnancies will
demonstrate a normal doubling time.
A single hCG value does not reliably
differentiate a viable IUP, a nonviable
IUP, or an ectopic pregnancy.
The majority of patients with an
ectopic pregnancy will have a slower
serial hCG rise than women with a
normal IUP.
Weeks since
LMP
Approximate hCG Range
(mIU/mL)
4 weeks 0–750
5 weeks 200–7000
6 weeks 200–32,000
7 weeks 3000–160,000
8–12 weeks 32,000–210,000
13–16 weeks 9000–210,000
16–29 weeks 1400–53,000
29–41 weeks 940–60, 000
11.
Risk Factors forEctopic Pregnancy
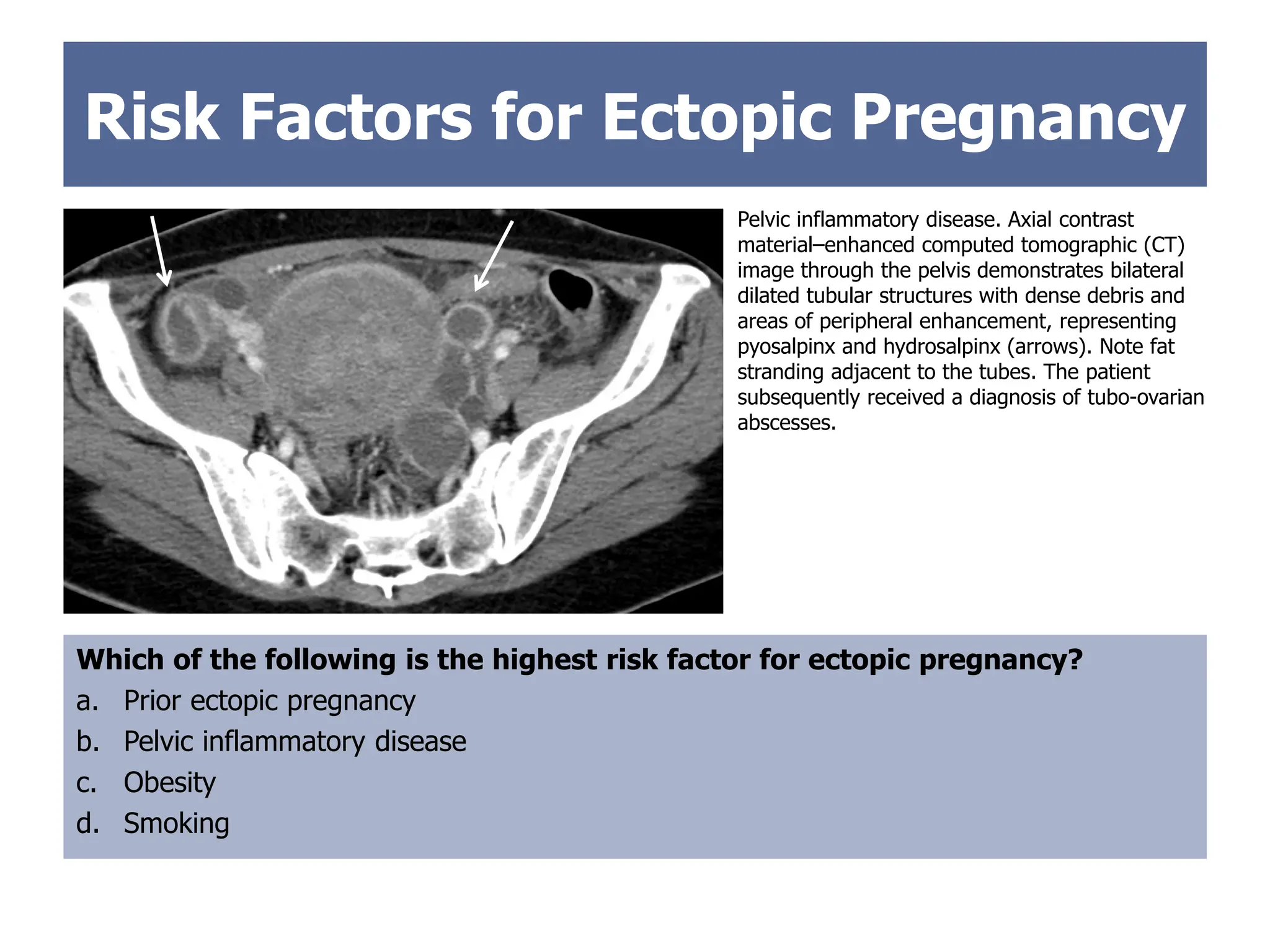
Which of the following is the highest risk factor for ectopic pregnancy?
a. Prior ectopic pregnancy
b. Pelvic inflammatory disease
c. Obesity
d. Smoking
Pelvic inflammatory disease. Axial contrast
material–enhanced computed tomographic (CT)
image through the pelvis demonstrates bilateral
dilated tubular structures with dense debris and
areas of peripheral enhancement, representing
pyosalpinx and hydrosalpinx (arrows). Note fat
stranding adjacent to the tubes. The patient
subsequently received a diagnosis of tubo-ovarian
abscesses.
12.
Risk Factors forEctopic Pregnancy
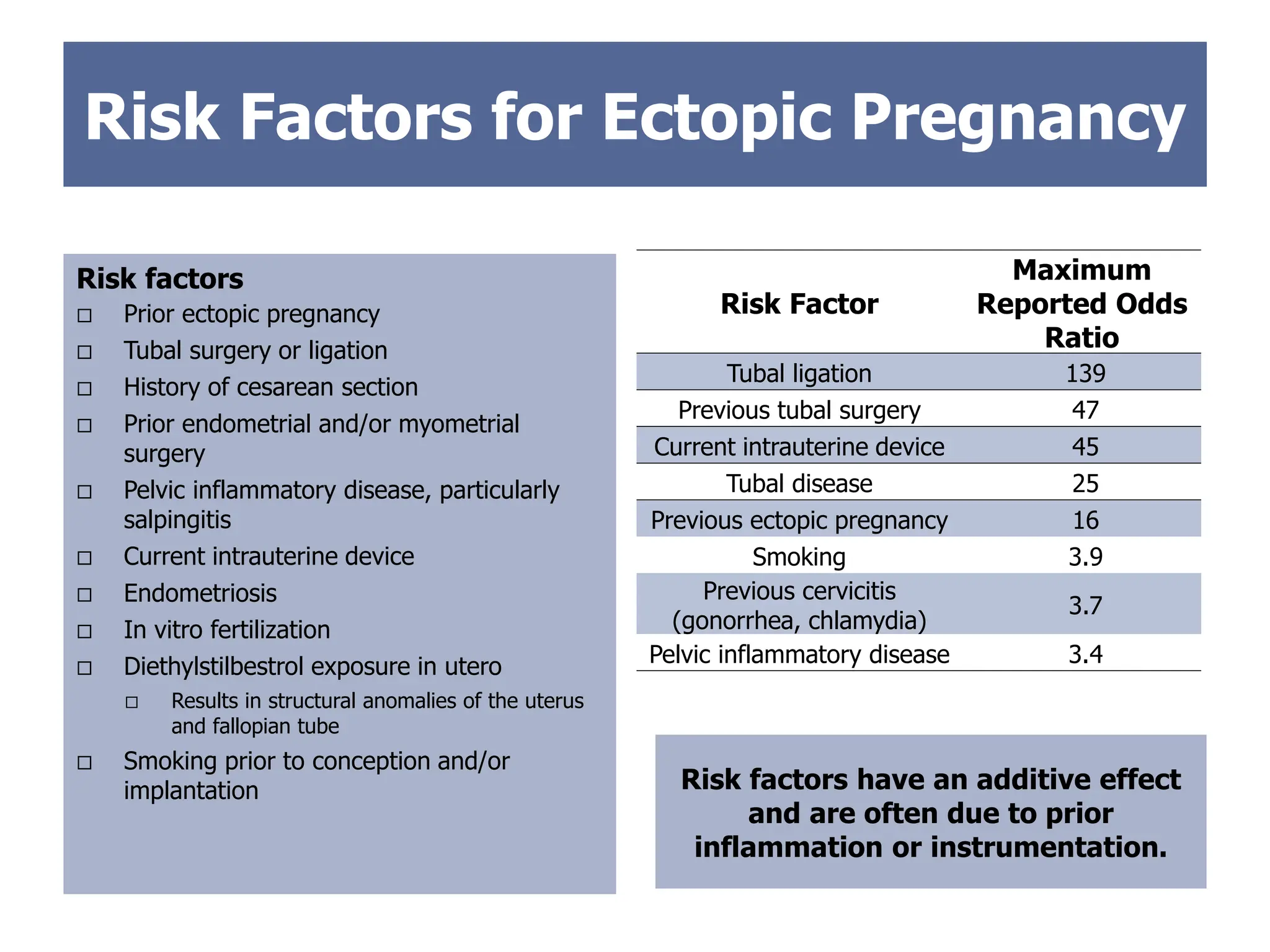
Risk factors
Prior ectopic pregnancy
Tubal surgery or ligation
History of cesarean section
Prior endometrial and/or myometrial
surgery
Pelvic inflammatory disease, particularly
salpingitis
Current intrauterine device
Endometriosis
In vitro fertilization
Diethylstilbestrol exposure in utero
Results in structural anomalies of the uterus
and fallopian tube
Smoking prior to conception and/or
implantation
Risk Factor
Maximum
Reported Odds
Ratio
Tubal ligation 139
Previous tubal surgery 47
Current intrauterine device 45
Tubal disease 25
Previous ectopic pregnancy 16
Smoking 3.9
Previous cervicitis
(gonorrhea, chlamydia)
3.7
Pelvic inflammatory disease 3.4
Risk factors have an additive effect
and are often due to prior
inflammation or instrumentation.
13.
Case 1
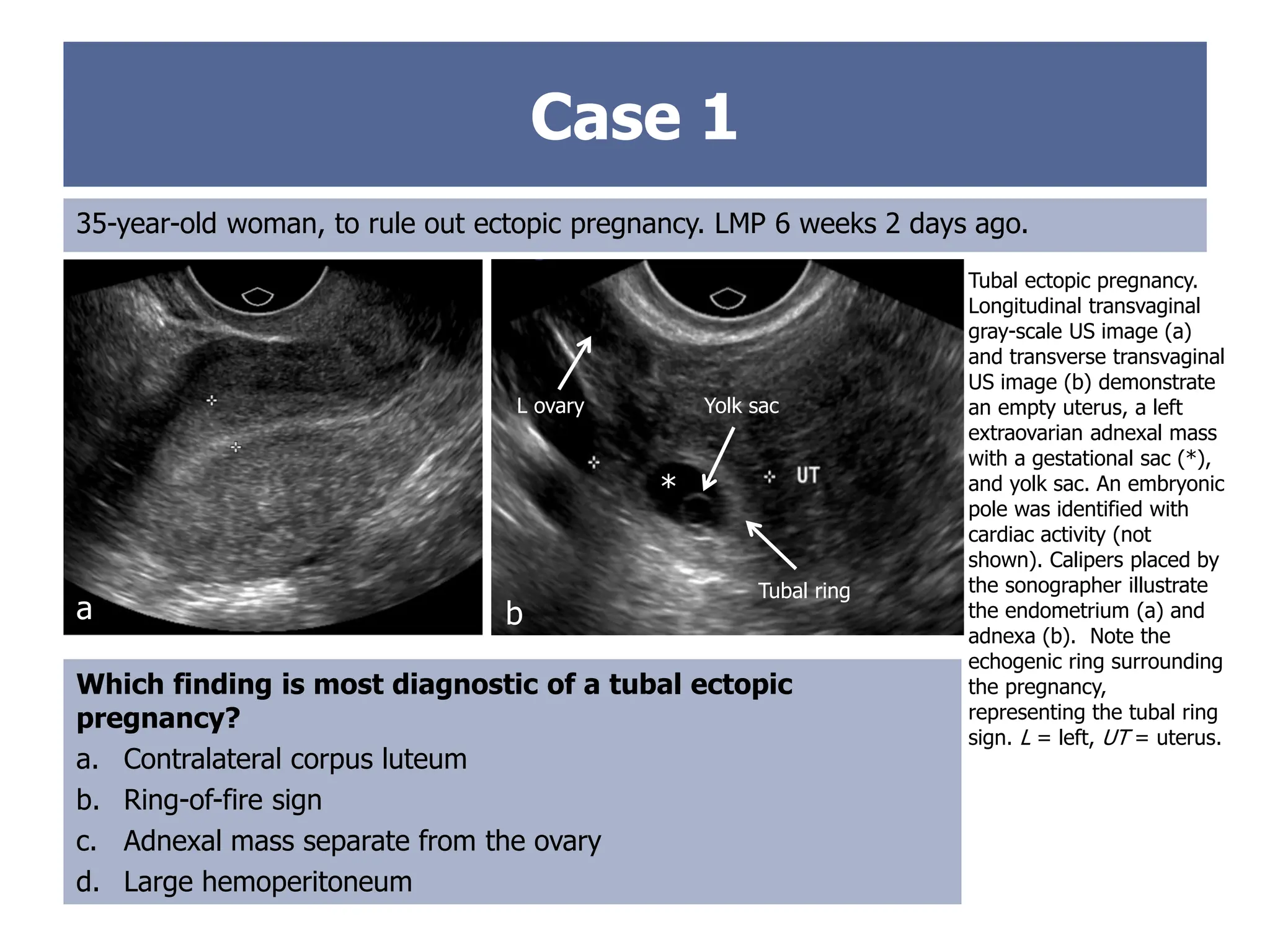
35-year-old woman,to rule out ectopic pregnancy. LMP 6 weeks 2 days ago.
Tubal ectopic pregnancy.
Longitudinal transvaginal
gray-scale US image (a)
and transverse transvaginal
US image (b) demonstrate
an empty uterus, a left
extraovarian adnexal mass
with a gestational sac (*),
and yolk sac. An embryonic
pole was identified with
cardiac activity (not
shown). Calipers placed by
the sonographer illustrate
the endometrium (a) and
adnexa (b). Note the
echogenic ring surrounding
the pregnancy,
representing the tubal ring
sign. L = left, UT = uterus.
Which finding is most diagnostic of a tubal ectopic
pregnancy?
a. Contralateral corpus luteum
b. Ring-of-fire sign
c. Adnexal mass separate from the ovary
d. Large hemoperitoneum
a b
*
L ovary Yolk sac
Tubal ring
14.
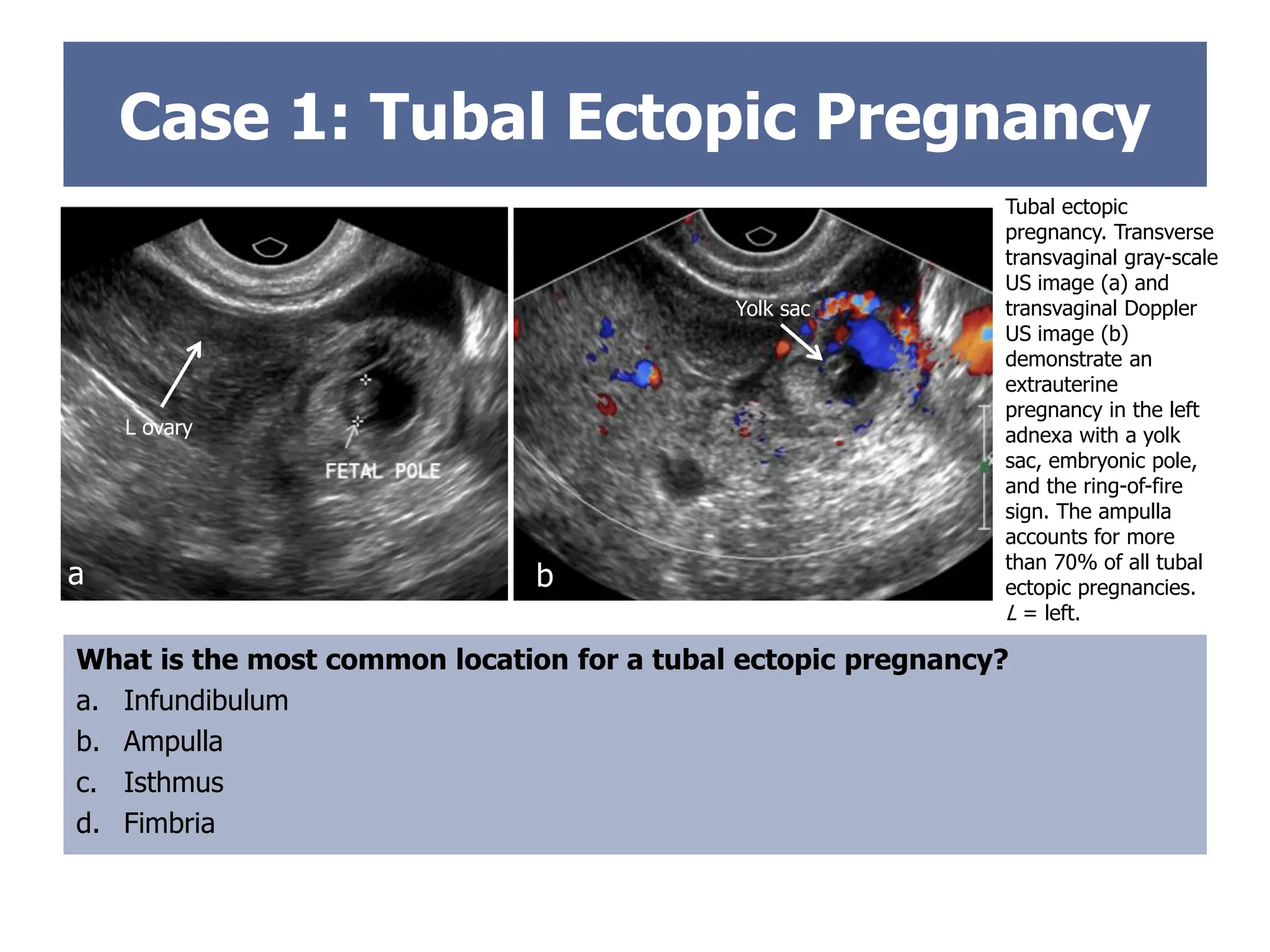
Case 1: TubalEctopic Pregnancy
Tubal ectopic
pregnancy. Transverse
transvaginal gray-scale
US image (a) and
transvaginal Doppler
US image (b)
demonstrate an
extrauterine
pregnancy in the left
adnexa with a yolk
sac, embryonic pole,
and the ring-of-fire
sign. The ampulla
accounts for more
than 70% of all tubal
ectopic pregnancies.
L = left.
What is the most common location for a tubal ectopic pregnancy?
a. Infundibulum
b. Ampulla
c. Isthmus
d. Fimbria
RING OF FIRE
b
a
L ovary
Yolk sac
15.
Case 1: TubalEctopic Pregnancy
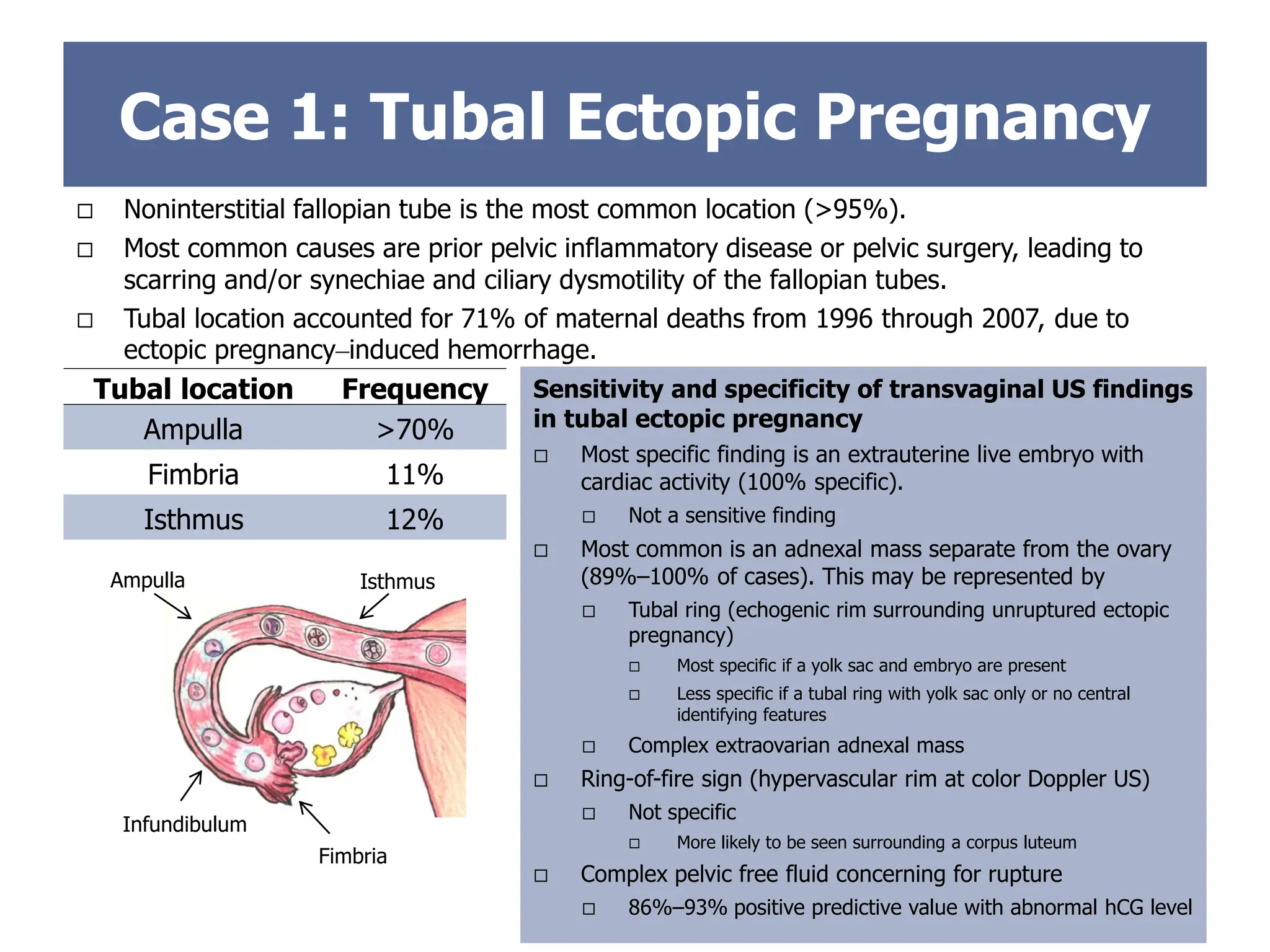
Noninterstitial fallopian tube is the most common location (>95%).
Most common causes are prior pelvic inflammatory disease or pelvic surgery, leading to
scarring and/or synechiae and ciliary dysmotility of the fallopian tubes.
Tubal location accounted for 71% of maternal deaths from 1996 through 2007, due to
ectopic pregnancy–induced hemorrhage.
Sensitivity and specificity of transvaginal US findings
in tubal ectopic pregnancy
Most specific finding is an extrauterine live embryo with
cardiac activity (100% specific).
Not a sensitive finding
Most common is an adnexal mass separate from the ovary
(89%–100% of cases). This may be represented by
Tubal ring (echogenic rim surrounding unruptured ectopic
pregnancy)
Most specific if a yolk sac and embryo are present
Less specific if a tubal ring with yolk sac only or no central
identifying features
Complex extraovarian adnexal mass
Ring-of-fire sign (hypervascular rim at color Doppler US)
Not specific
More likely to be seen surrounding a corpus luteum
Complex pelvic free fluid concerning for rupture
86%–93% positive predictive value with abnormal hCG level
Tubal location Frequency
Ampulla >70%
Fimbria 11%
Isthmus 12%
Fimbria
Ampulla Isthmus
Infundibulum
16.
Right ovary
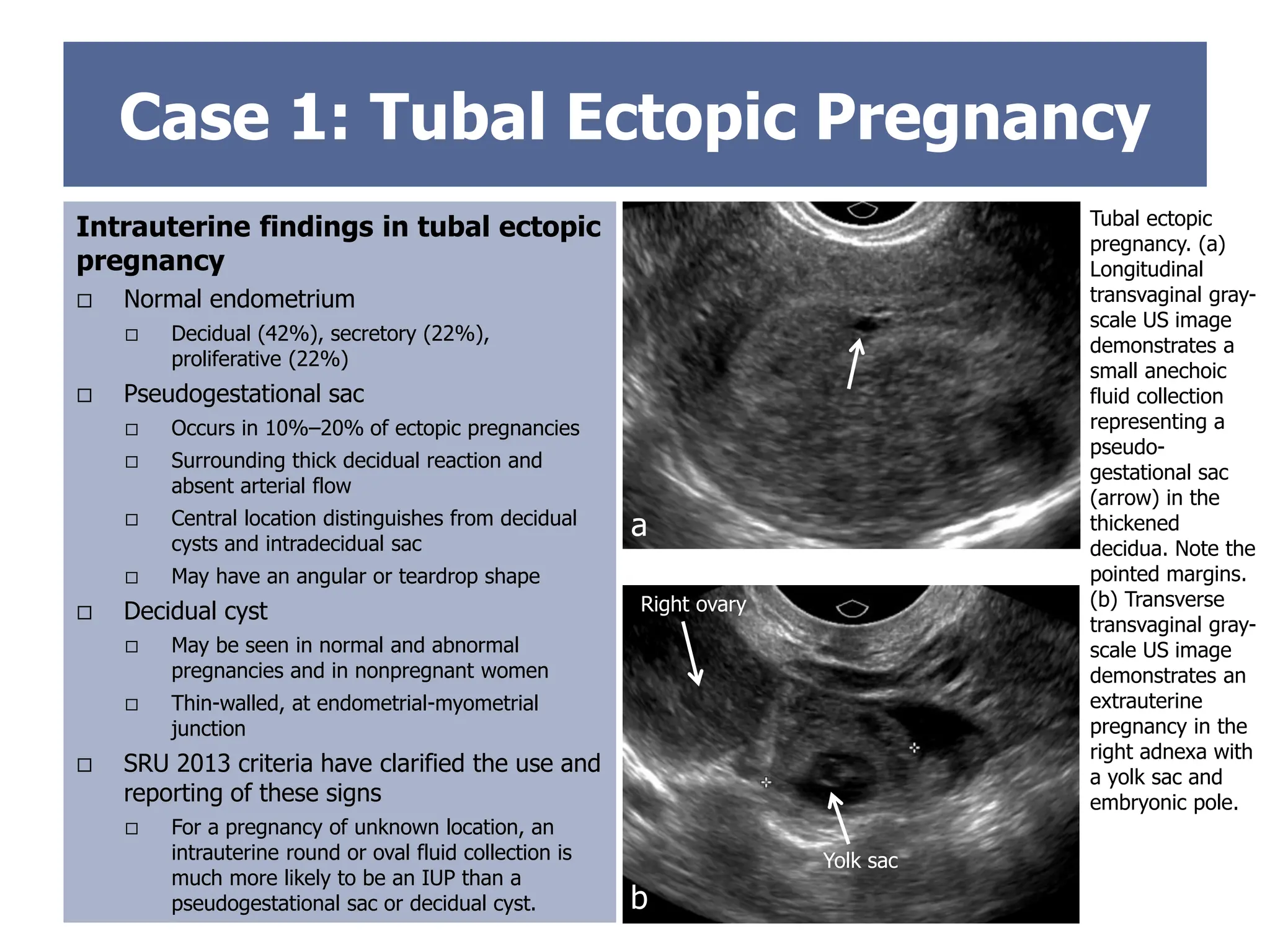
Case 1:Tubal Ectopic Pregnancy
Intrauterine findings in tubal ectopic
pregnancy
Normal endometrium
Decidual (42%), secretory (22%),
proliferative (22%)
Pseudogestational sac
Occurs in 10%–20% of ectopic pregnancies
Surrounding thick decidual reaction and
absent arterial flow
Central location distinguishes from decidual
cysts and intradecidual sac
May have an angular or teardrop shape
Decidual cyst
May be seen in normal and abnormal
pregnancies and in nonpregnant women
Thin-walled, at endometrial-myometrial
junction
SRU 2013 criteria have clarified the use and
reporting of these signs
For a pregnancy of unknown location, an
intrauterine round or oval fluid collection is
much more likely to be an IUP than a
pseudogestational sac or decidual cyst.
Tubal ectopic
pregnancy. (a)
Longitudinal
transvaginal gray-
scale US image
demonstrates a
small anechoic
fluid collection
representing a
pseudo-
gestational sac
(arrow) in the
thickened
decidua. Note the
pointed margins.
(b) Transverse
transvaginal gray-
scale US image
demonstrates an
extrauterine
pregnancy in the
right adnexa with
a yolk sac and
embryonic pole.
a
b
Yolk sac
17.
Case 2
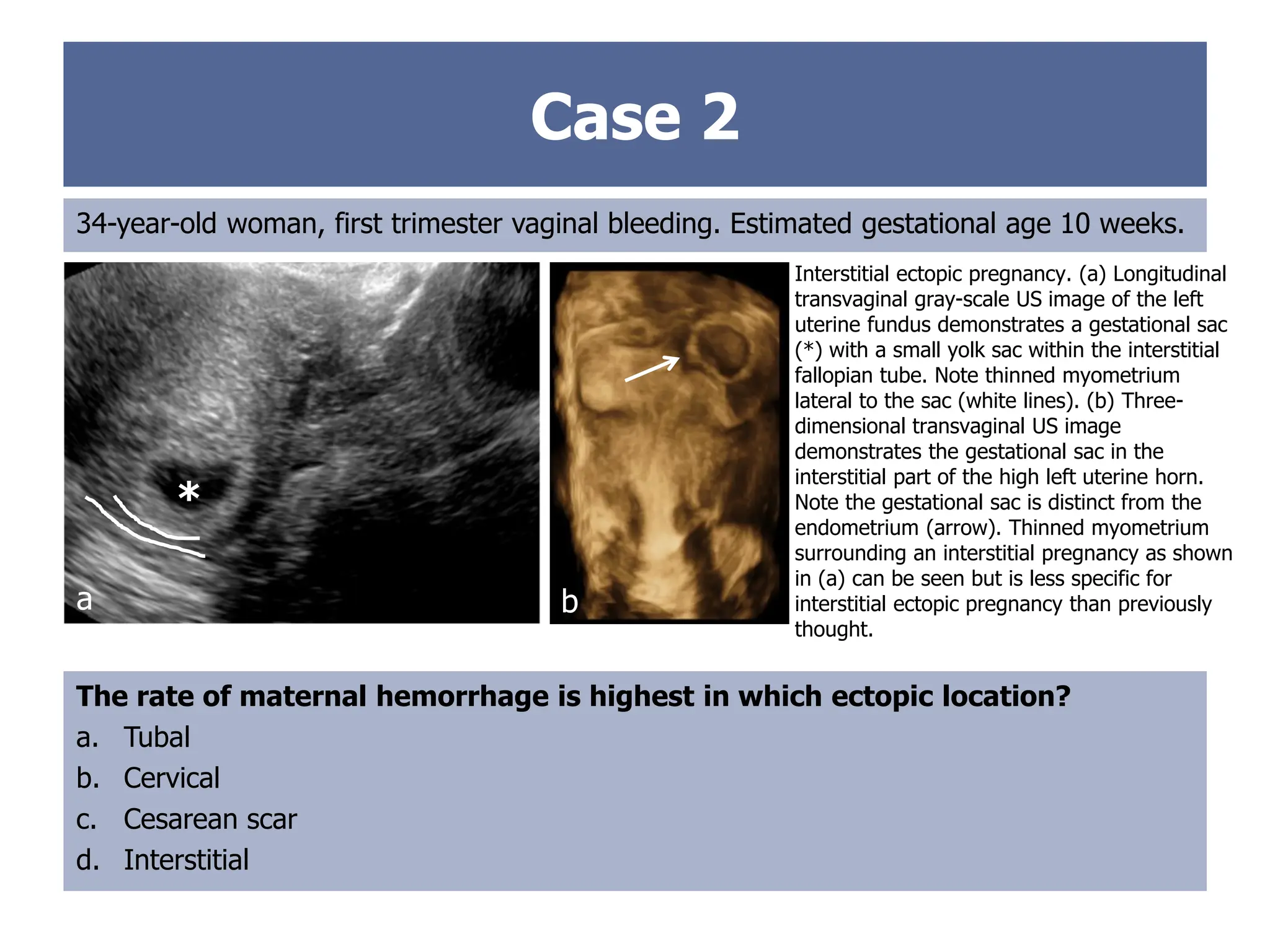
34-year-old woman,first trimester vaginal bleeding. Estimated gestational age 10 weeks.
The rate of maternal hemorrhage is highest in which ectopic location?
a. Tubal
b. Cervical
c. Cesarean scar
d. Interstitial
Interstitial ectopic pregnancy. (a) Longitudinal
transvaginal gray-scale US image of the left
uterine fundus demonstrates a gestational sac
(*) with a small yolk sac within the interstitial
fallopian tube. Note thinned myometrium
lateral to the sac (white lines). (b) Three-
dimensional transvaginal US image
demonstrates the gestational sac in the
interstitial part of the high left uterine horn.
Note the gestational sac is distinct from the
endometrium (arrow). Thinned myometrium
surrounding an interstitial pregnancy as shown
in (a) can be seen but is less specific for
interstitial ectopic pregnancy than previously
thought.
*
a b
18.
Case 2: InterstitialEctopic
Pregnancy
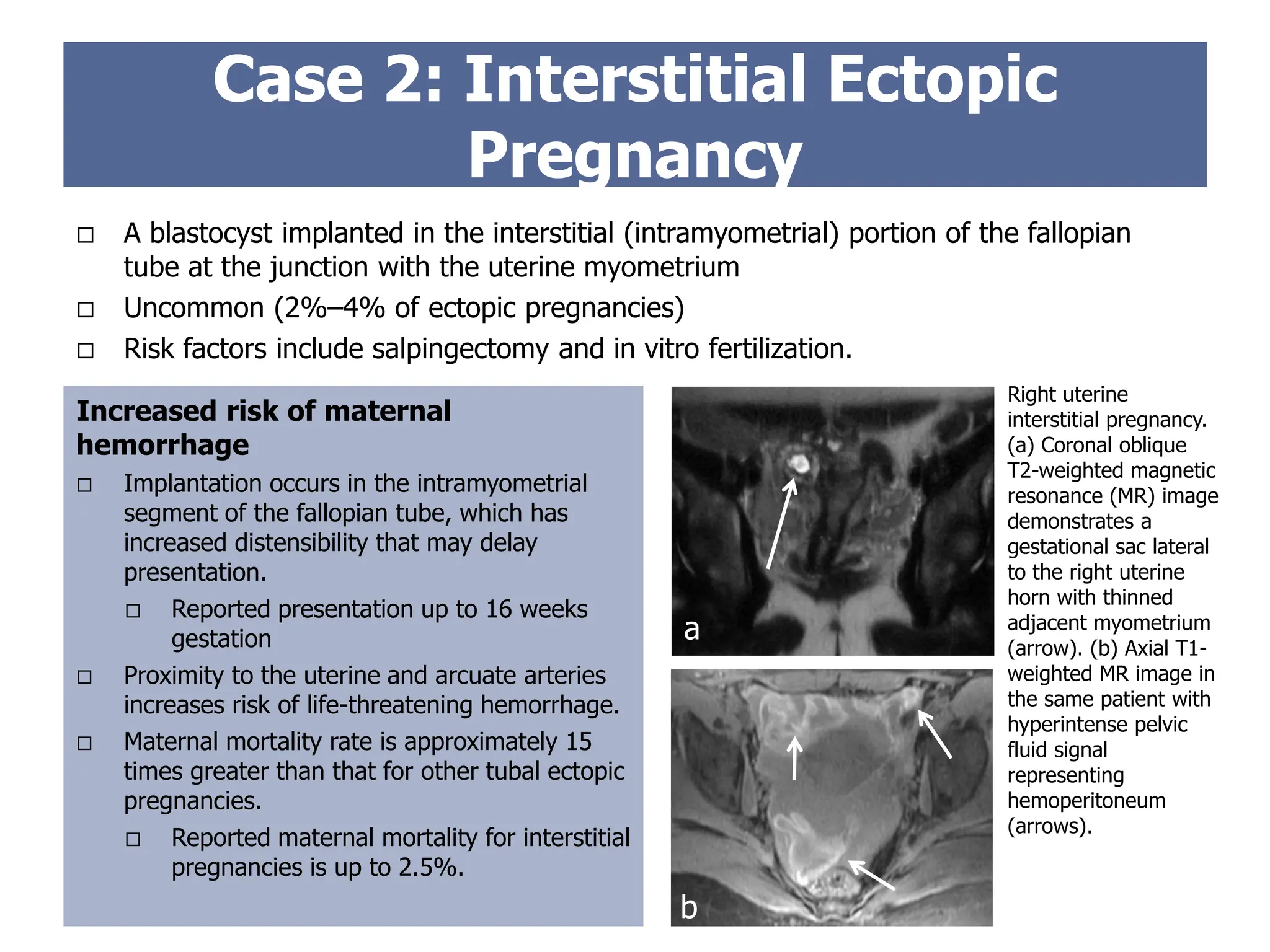
Increased risk of maternal
hemorrhage
Implantation occurs in the intramyometrial
segment of the fallopian tube, which has
increased distensibility that may delay
presentation.
Reported presentation up to 16 weeks
gestation
Proximity to the uterine and arcuate arteries
increases risk of life-threatening hemorrhage.
Maternal mortality rate is approximately 15
times greater than that for other tubal ectopic
pregnancies.
Reported maternal mortality for interstitial
pregnancies is up to 2.5%.
A blastocyst implanted in the interstitial (intramyometrial) portion of the fallopian
tube at the junction with the uterine myometrium
Uncommon (2%–4% of ectopic pregnancies)
Risk factors include salpingectomy and in vitro fertilization.
Right uterine
interstitial pregnancy.
(a) Coronal oblique
T2-weighted magnetic
resonance (MR) image
demonstrates a
gestational sac lateral
to the right uterine
horn with thinned
adjacent myometrium
(arrow). (b) Axial T1-
weighted MR image in
the same patient with
hyperintense pelvic
fluid signal
representing
hemoperitoneum
(arrows).
a
b
19.
Case 2: InterstitialEctopic Pregnancy
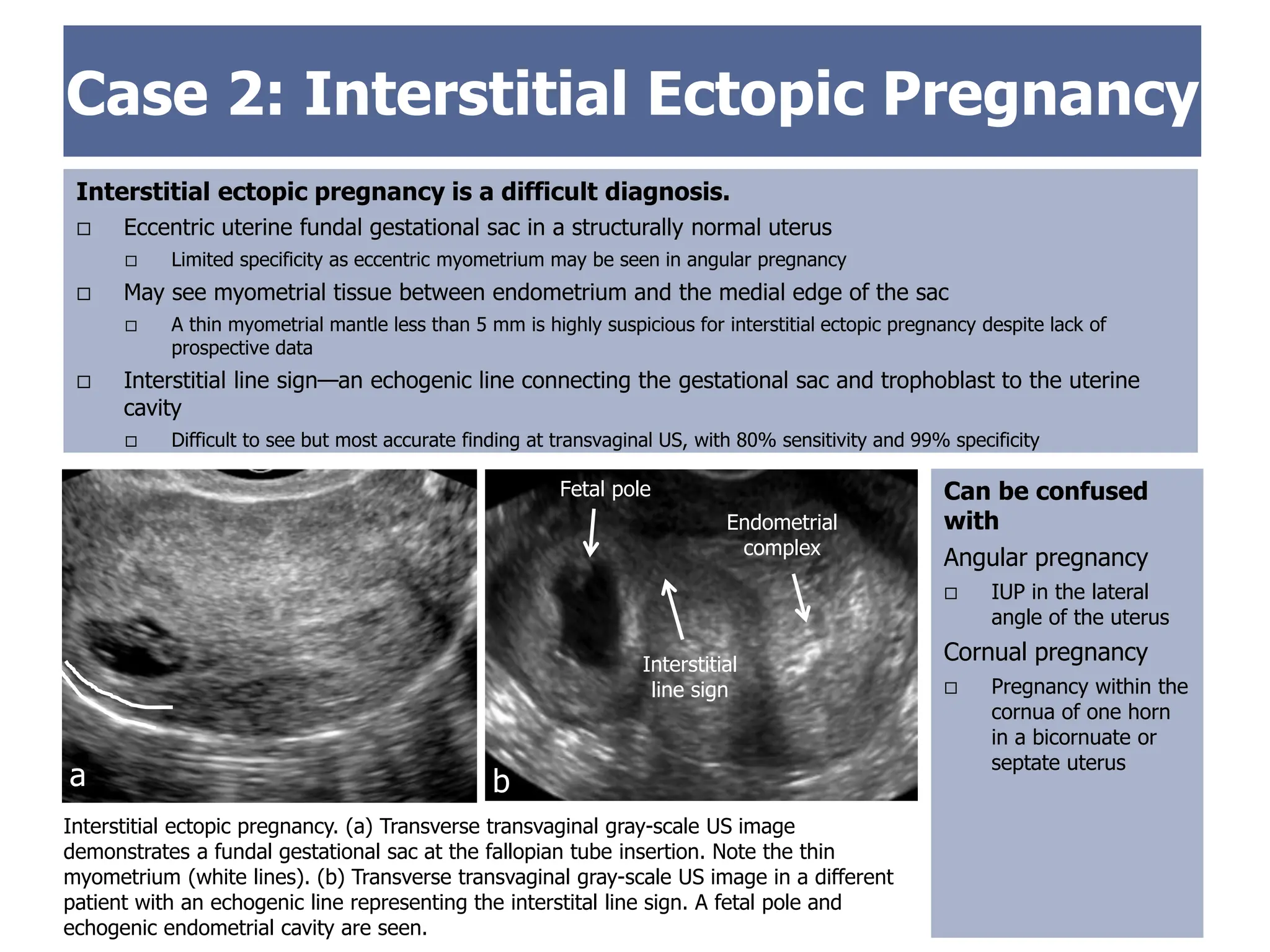
Interstitial ectopic pregnancy is a difficult diagnosis.
Eccentric uterine fundal gestational sac in a structurally normal uterus
Limited specificity as eccentric myometrium may be seen in angular pregnancy
May see myometrial tissue between endometrium and the medial edge of the sac
A thin myometrial mantle less than 5 mm is highly suspicious for interstitial ectopic pregnancy despite lack of
prospective data
Interstitial line sign—an echogenic line connecting the gestational sac and trophoblast to the uterine
cavity
Difficult to see but most accurate finding at transvaginal US, with 80% sensitivity and 99% specificity
Interstitial ectopic pregnancy. (a) Transverse transvaginal gray-scale US image
demonstrates a fundal gestational sac at the fallopian tube insertion. Note the thin
myometrium (white lines). (b) Transverse transvaginal gray-scale US image in a different
patient with an echogenic line representing the interstital line sign. A fetal pole and
echogenic endometrial cavity are seen.
Endometrial
complex
Interstitial
line sign
a b
Fetal pole Can be confused
with
Angular pregnancy
IUP in the lateral
angle of the uterus
Cornual pregnancy
Pregnancy within the
cornua of one horn
in a bicornuate or
septate uterus
20.
Case 3
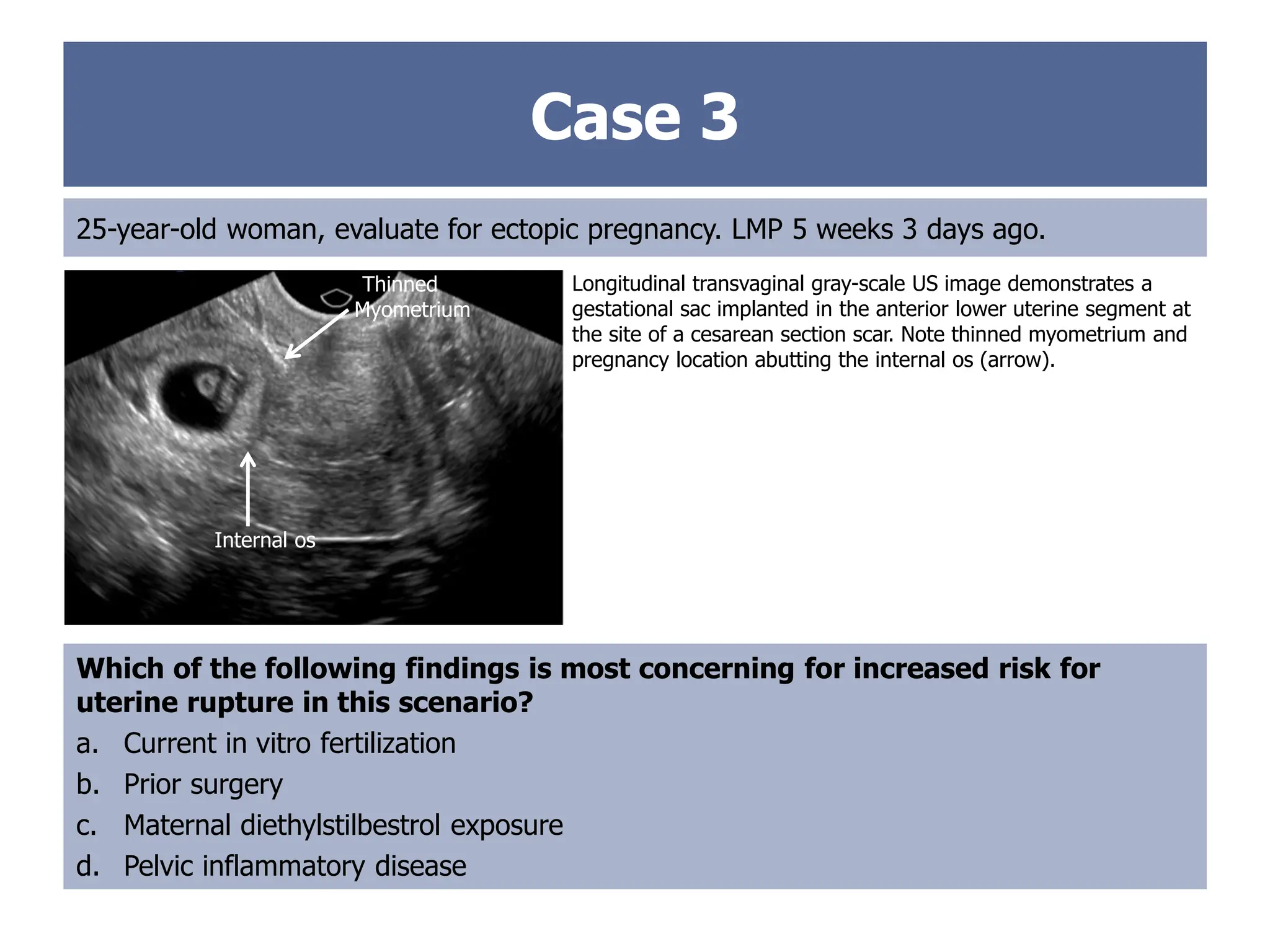
25-year-old woman,evaluate for ectopic pregnancy. LMP 5 weeks 3 days ago.
Which of the following findings is most concerning for increased risk for
uterine rupture in this scenario?
a. Current in vitro fertilization
b. Prior surgery
c. Maternal diethylstilbestrol exposure
d. Pelvic inflammatory disease
Longitudinal transvaginal gray-scale US image demonstrates a
gestational sac implanted in the anterior lower uterine segment at
the site of a cesarean section scar. Note thinned myometrium and
pregnancy location abutting the internal os (arrow).
Internal os
Thinned
Myometrium
21.
Case 3
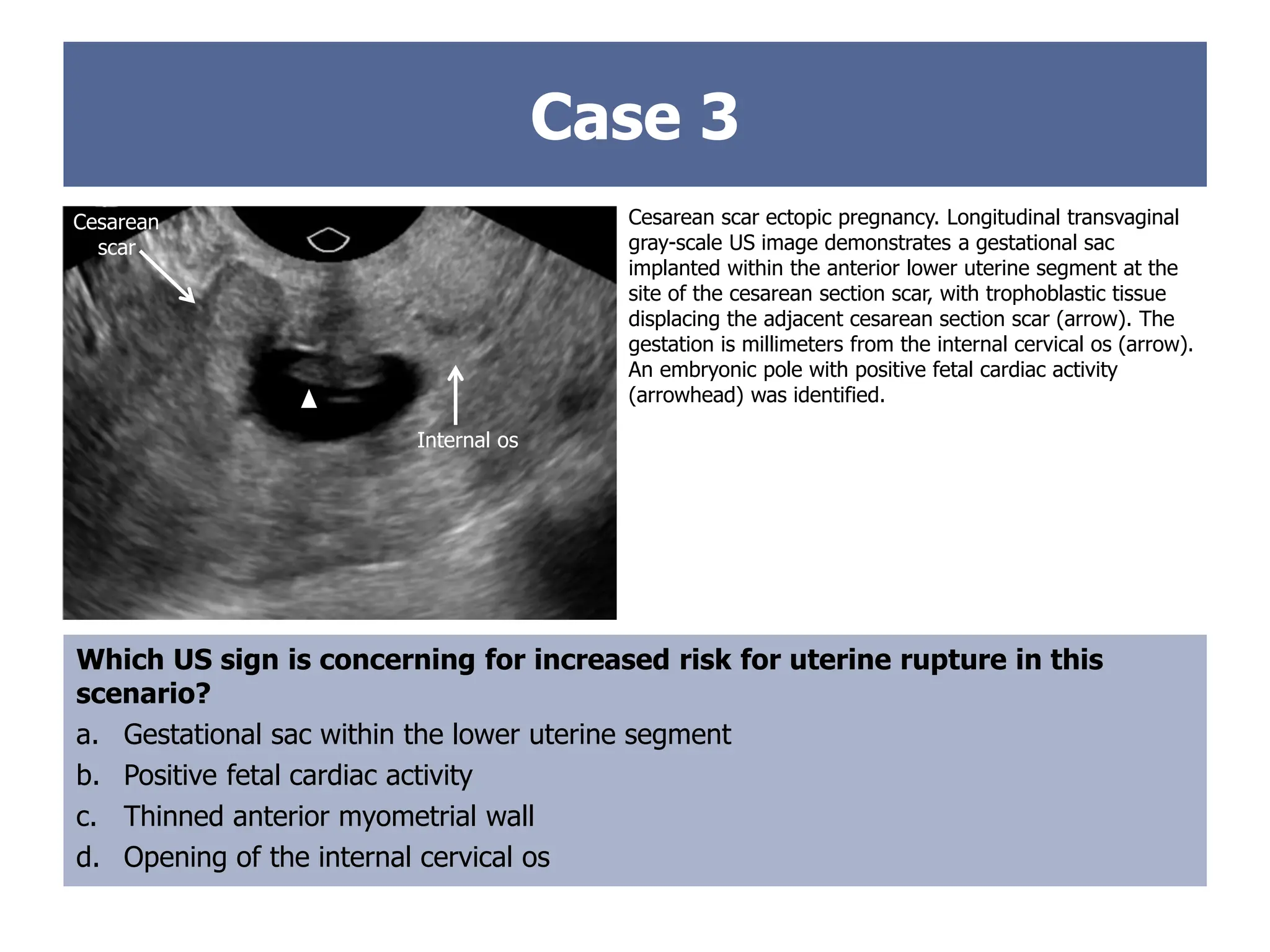
Cesarean scarectopic pregnancy. Longitudinal transvaginal
gray-scale US image demonstrates a gestational sac
implanted within the anterior lower uterine segment at the
site of the cesarean section scar, with trophoblastic tissue
displacing the adjacent cesarean section scar (arrow). The
gestation is millimeters from the internal cervical os (arrow).
An embryonic pole with positive fetal cardiac activity
(arrowhead) was identified.
Which US sign is concerning for increased risk for uterine rupture in this
scenario?
a. Gestational sac within the lower uterine segment
b. Positive fetal cardiac activity
c. Thinned anterior myometrial wall
d. Opening of the internal cervical os
Internal Os
Cesarean
scar
Internal os
22.
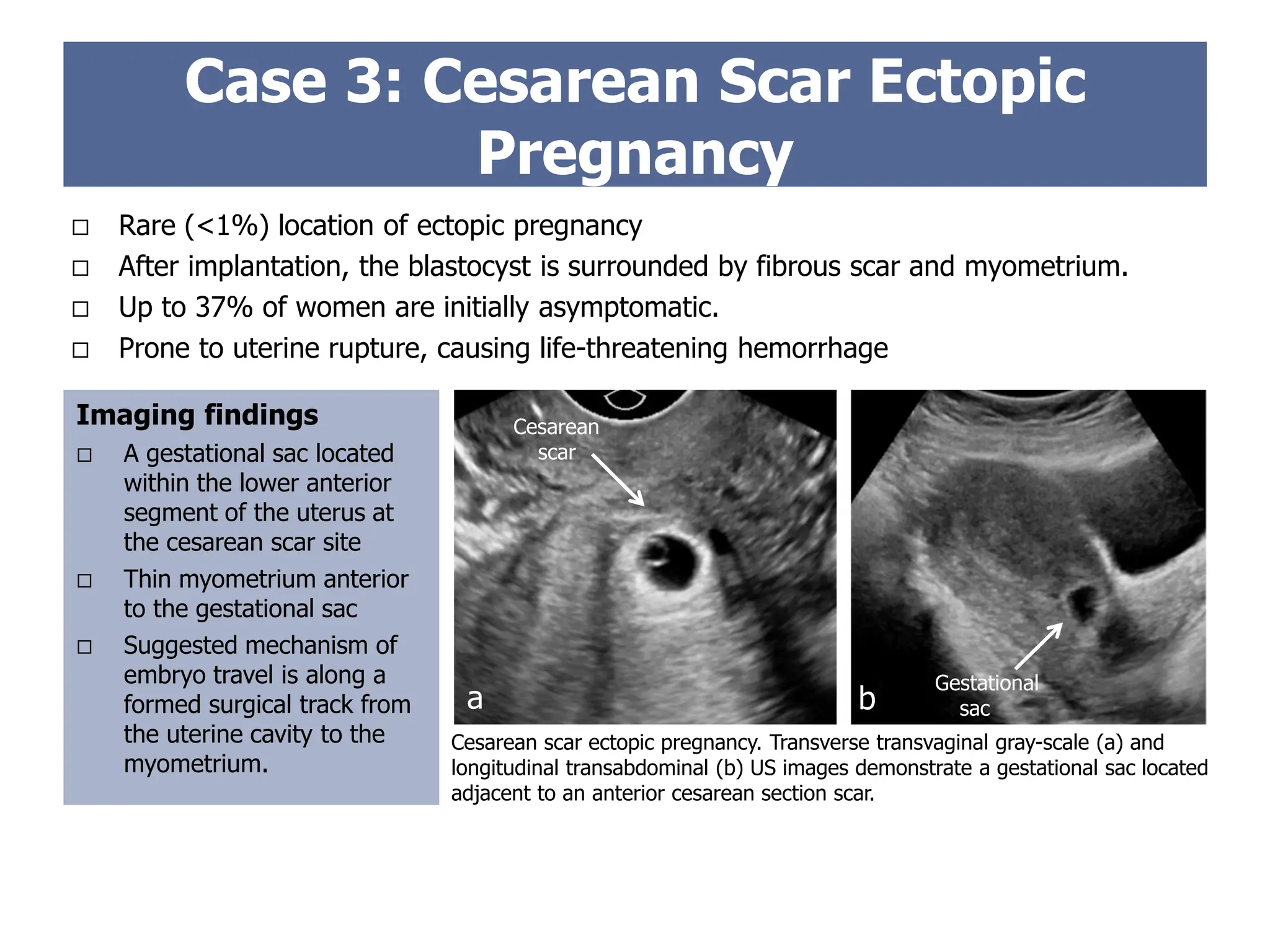
Rare (<1%)location of ectopic pregnancy
After implantation, the blastocyst is surrounded by fibrous scar and myometrium.
Up to 37% of women are initially asymptomatic.
Prone to uterine rupture, causing life-threatening hemorrhage
Imaging findings
A gestational sac located
within the lower anterior
segment of the uterus at
the cesarean scar site
Thin myometrium anterior
to the gestational sac
Suggested mechanism of
embryo travel is along a
formed surgical track from
the uterine cavity to the
myometrium.
Case 3: Cesarean Scar Ectopic
Pregnancy
Cesarean scar ectopic pregnancy. Transverse transvaginal gray-scale (a) and
longitudinal transabdominal (b) US images demonstrate a gestational sac located
adjacent to an anterior cesarean section scar.
Cesarean
scar
Gestational
sac
a b
23.
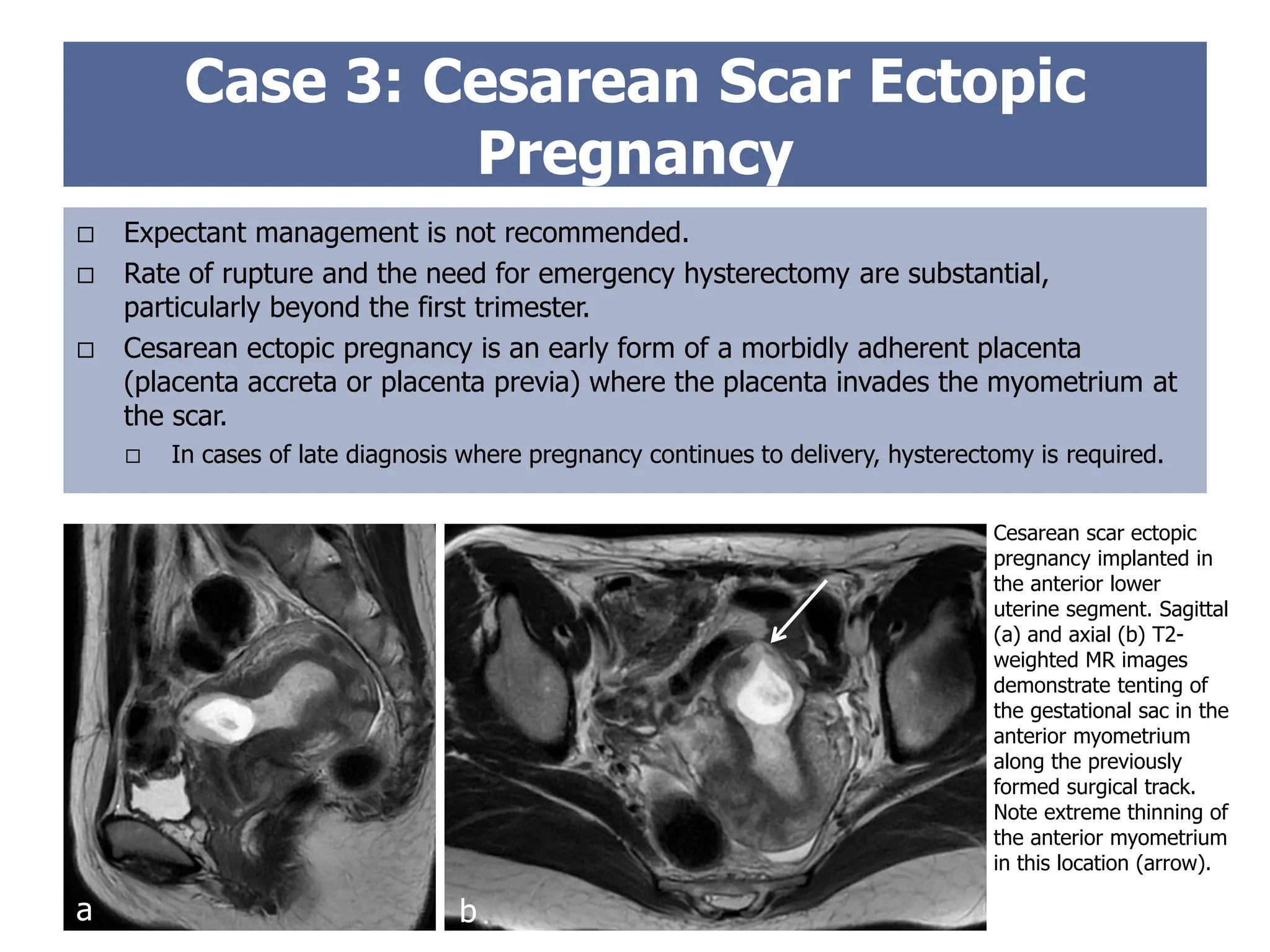
Expectant managementis not recommended.
Rate of rupture and the need for emergency hysterectomy are substantial,
particularly beyond the first trimester.
Cesarean ectopic pregnancy is an early form of a morbidly adherent placenta
(placenta accreta or placenta previa) where the placenta invades the myometrium at
the scar.
In cases of late diagnosis where pregnancy continues to delivery, hysterectomy is required.
Case 3: Cesarean Scar Ectopic
Pregnancy
Cesarean scar ectopic
pregnancy implanted in
the anterior lower
uterine segment. Sagittal
(a) and axial (b) T2-
weighted MR images
demonstrate tenting of
the gestational sac in the
anterior myometrium
along the previously
formed surgical track.
Note extreme thinning of
the anterior myometrium
in this location (arrow).
a b
24.
Case 4
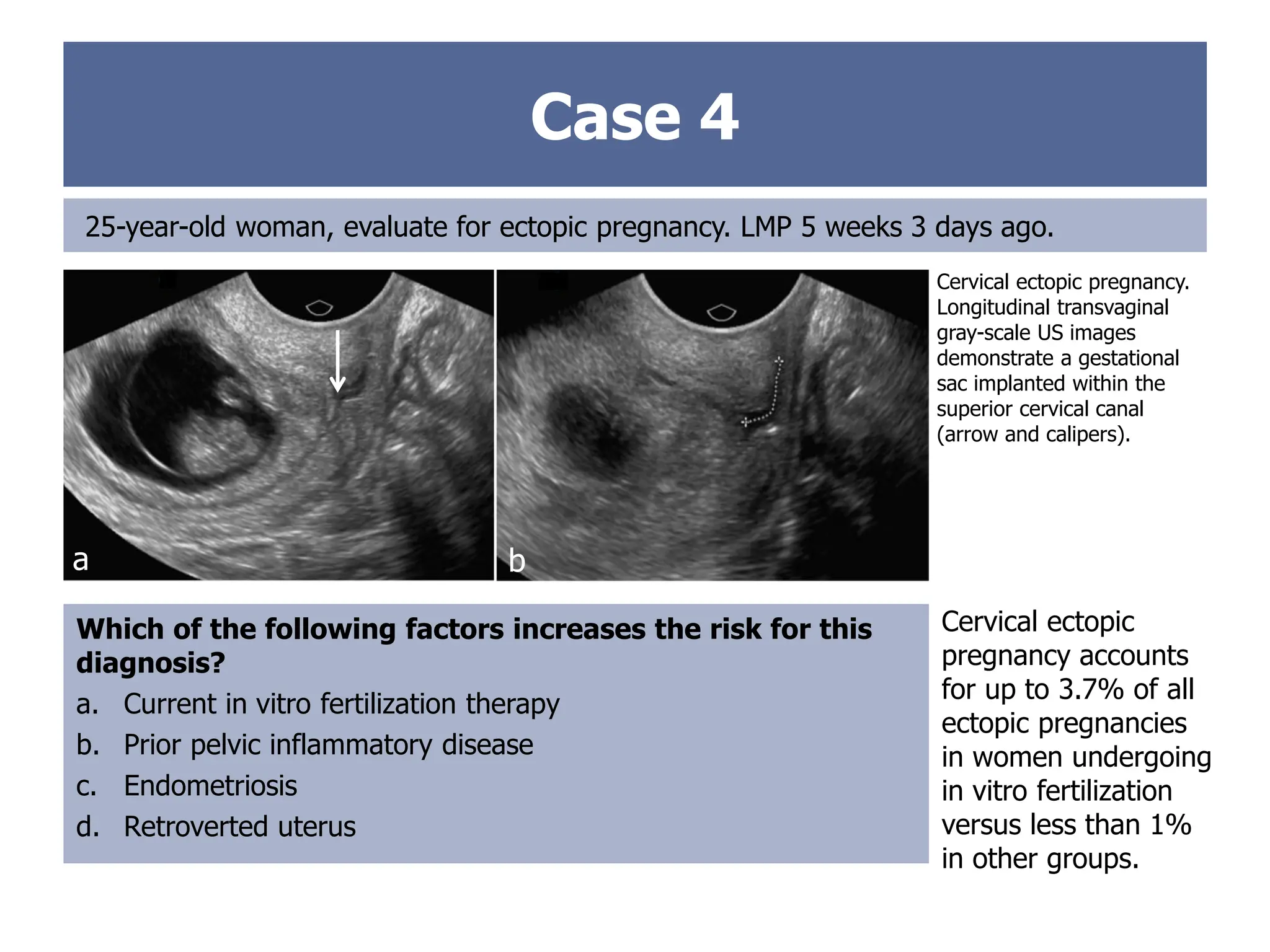
25-year-old woman,evaluate for ectopic pregnancy. LMP 5 weeks 3 days ago.
Cervical ectopic pregnancy.
Longitudinal transvaginal
gray-scale US images
demonstrate a gestational
sac implanted within the
superior cervical canal
(arrow and calipers).
Which of the following factors increases the risk for this
diagnosis?
a. Current in vitro fertilization therapy
b. Prior pelvic inflammatory disease
c. Endometriosis
d. Retroverted uterus
Cervical ectopic
pregnancy accounts
for up to 3.7% of all
ectopic pregnancies
in women undergoing
in vitro fertilization
versus less than 1%
in other groups.
a b
25.
Case 4
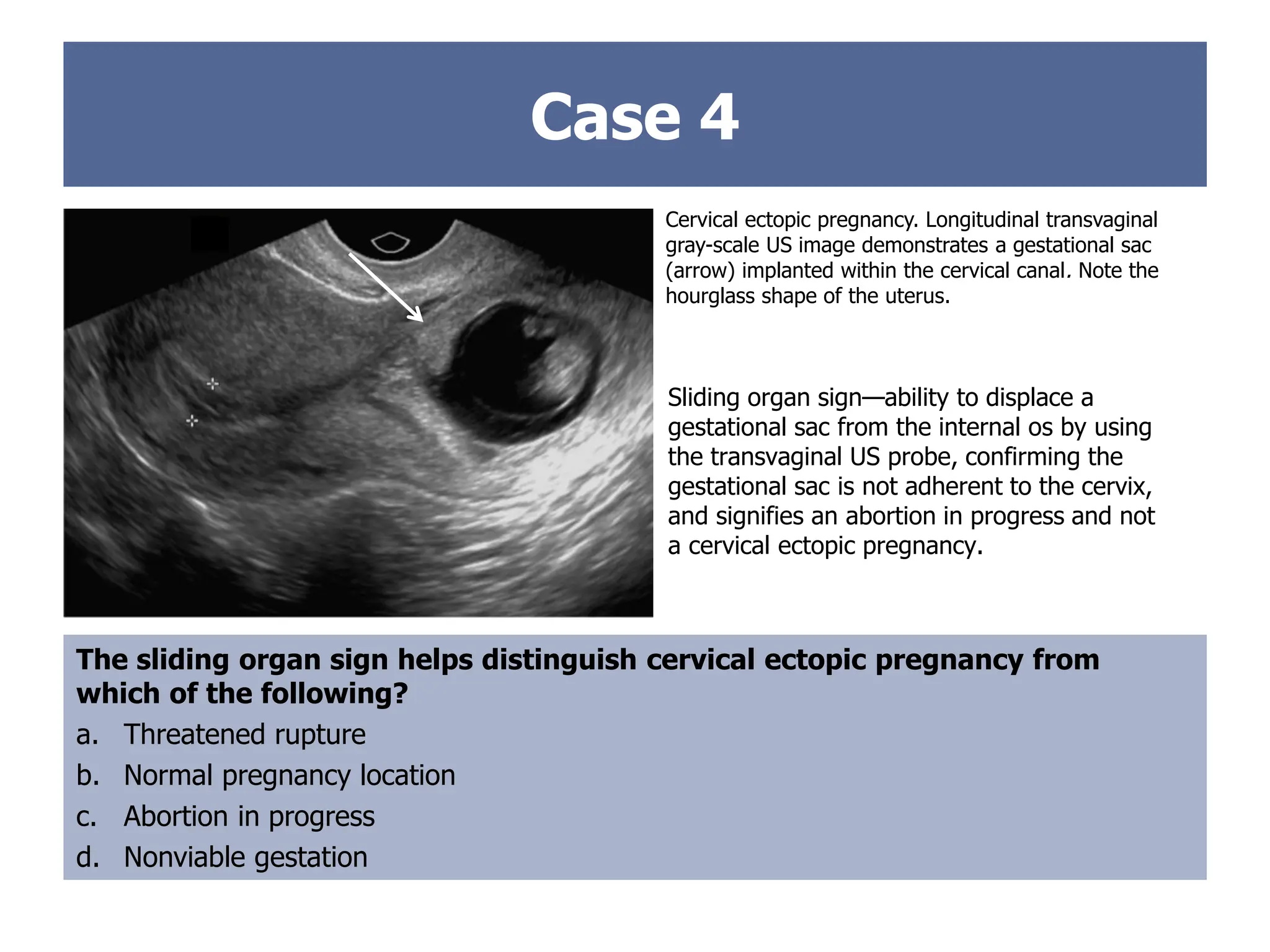
Cervical ectopicpregnancy. Longitudinal transvaginal
gray-scale US image demonstrates a gestational sac
(arrow) implanted within the cervical canal. Note the
hourglass shape of the uterus.
The sliding organ sign helps distinguish cervical ectopic pregnancy from
which of the following?
a. Threatened rupture
b. Normal pregnancy location
c. Abortion in progress
d. Nonviable gestation
Sliding organ sign—ability to displace a
gestational sac from the internal os by using
the transvaginal US probe, confirming the
gestational sac is not adherent to the cervix,
and signifies an abortion in progress and not
a cervical ectopic pregnancy.
26.
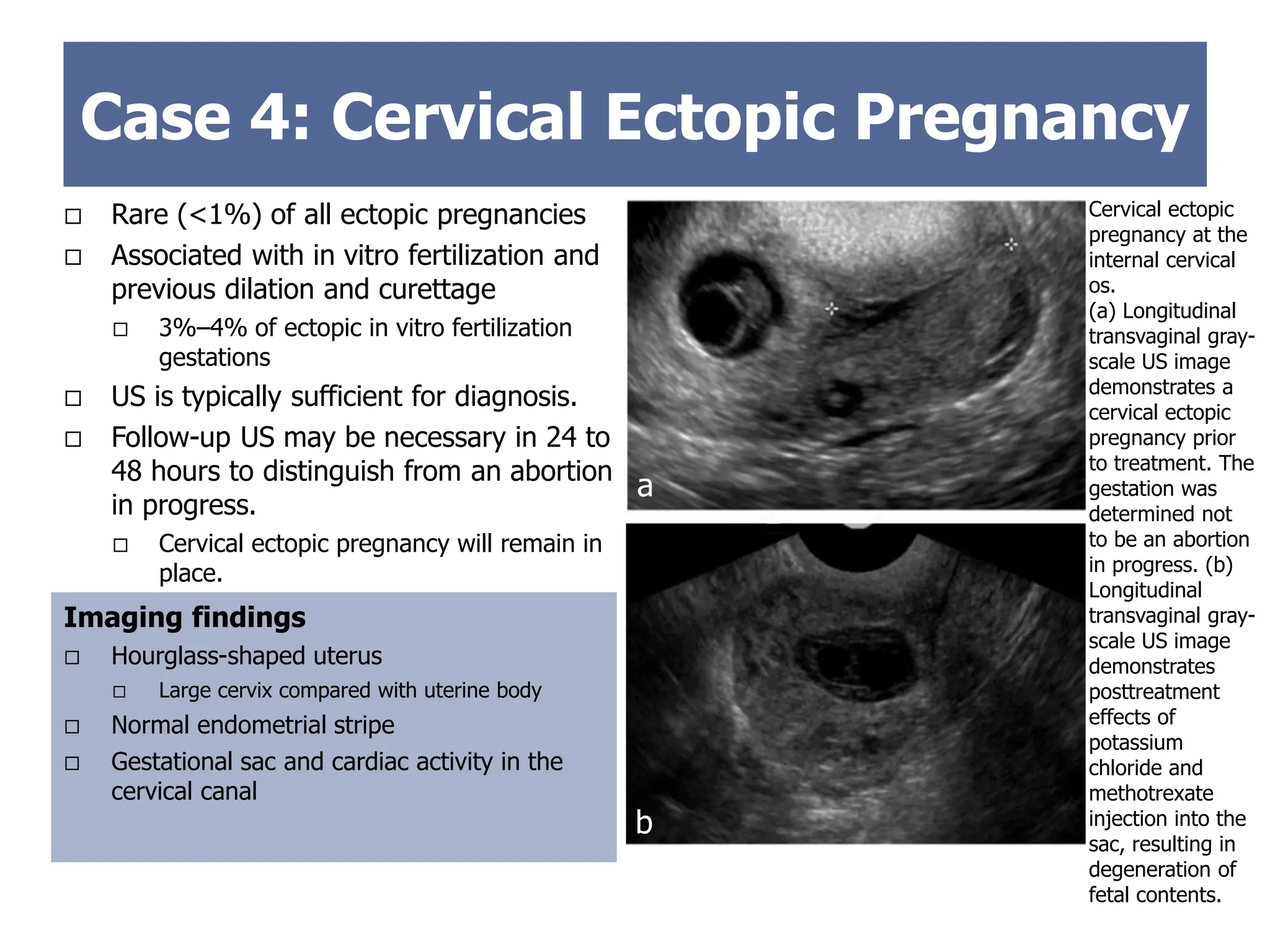
Rare (<1%)of all ectopic pregnancies
Associated with in vitro fertilization and
previous dilation and curettage
3%–4% of ectopic in vitro fertilization
gestations
US is typically sufficient for diagnosis.
Follow-up US may be necessary in 24 to
48 hours to distinguish from an abortion
in progress.
Cervical ectopic pregnancy will remain in
place.
Imaging findings
Hourglass-shaped uterus
Large cervix compared with uterine body
Normal endometrial stripe
Gestational sac and cardiac activity in the
cervical canal
Case 4: Cervical Ectopic Pregnancy
Cervical ectopic
pregnancy at the
internal cervical
os.
(a) Longitudinal
transvaginal gray-
scale US image
demonstrates a
cervical ectopic
pregnancy prior
to treatment. The
gestation was
determined not
to be an abortion
in progress. (b)
Longitudinal
transvaginal gray-
scale US image
demonstrates
posttreatment
effects of
potassium
chloride and
methotrexate
injection into the
sac, resulting in
degeneration of
fetal contents.
A
B
a
b
27.
Case 5
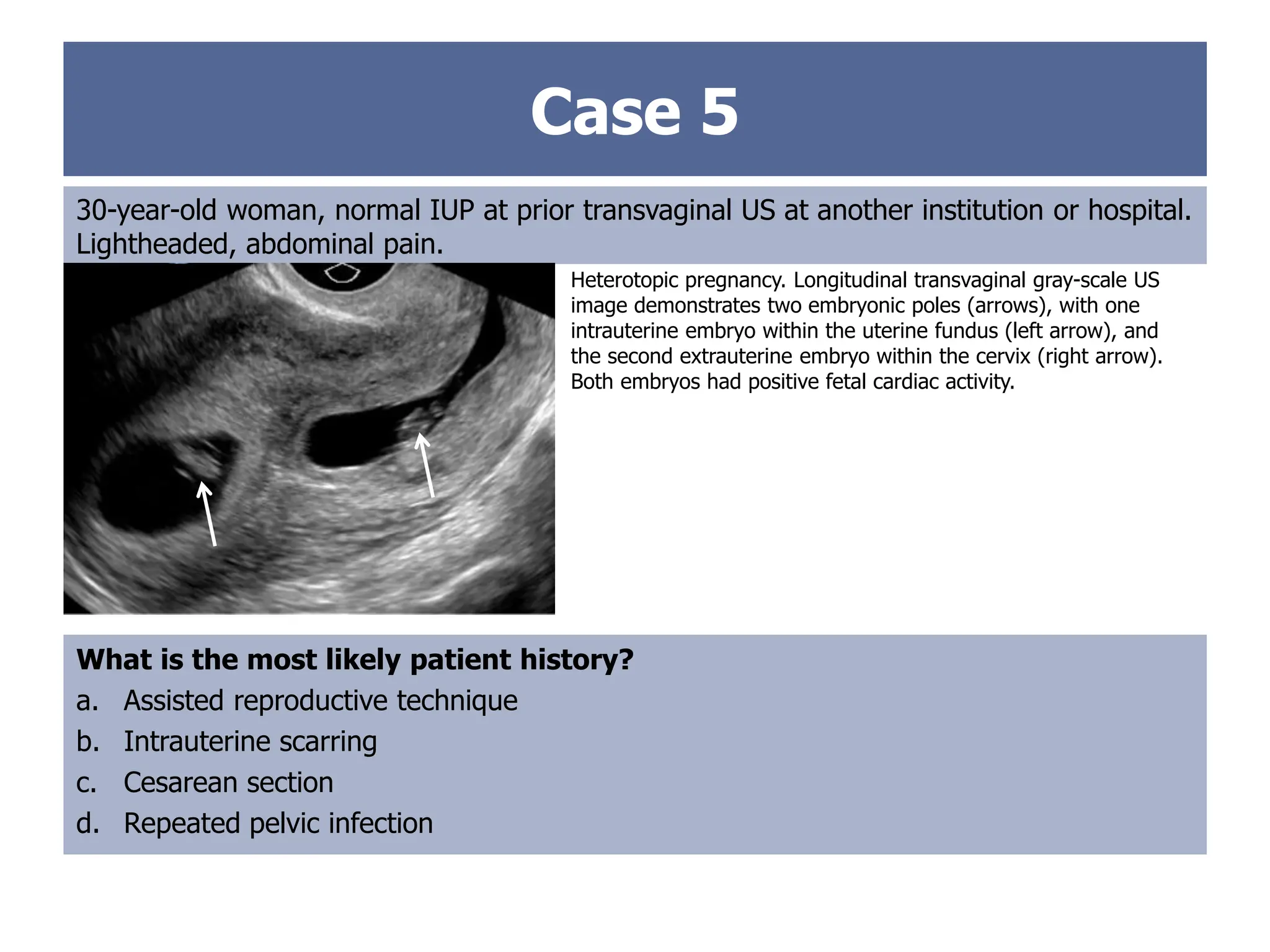
30-year-old woman,normal IUP at prior transvaginal US at another institution or hospital.
Lightheaded, abdominal pain.
Heterotopic pregnancy. Longitudinal transvaginal gray-scale US
image demonstrates two embryonic poles (arrows), with one
intrauterine embryo within the uterine fundus (left arrow), and
the second extrauterine embryo within the cervix (right arrow).
Both embryos had positive fetal cardiac activity.
What is the most likely patient history?
a. Assisted reproductive technique
b. Intrauterine scarring
c. Cesarean section
d. Repeated pelvic infection
28.
Rare (incidencereported from 1 in 2100 to
1 in 30,000 spontaneous pregnancies)
Increasing frequency due to assisted
reproductive techniques
According to National Assisted Reproductive
Technology Surveillance System data from
2000 to 2011, incidence was 485 of 553,557
pregnancies with assisted reproductive
techniques (1 in 1141).
Should be considered in patients with pelvic
and/or abdominal pain and prior assisted
reproduction
Specifically refers to concurrent intrauterine
and extrauterine pregnancy locations.
Extrauterine pregnancy rupture can result
in life-threatening maternal hemorrhage.
Diagnosis of an IUP at US should not
preclude a thorough evaluation for a
possible ectopic pregnancy.
Case 5: Heterotopic Ectopic
Pregnancy
The intrauterine gestation can be
allowed to progress normally.
Ruptured heterotopic pregnancy, in
addition to a ruptured corpus luteum,
should be considered when there is
hemorrhagic free fluid and a normal
IUP at US.
Treatments for the extrauterine
gestation include
Laparoscopic removal
Dilation and curettage
Imaging-guided ablation
29.
Ovarian and AbdominalEctopic
Pregnancy
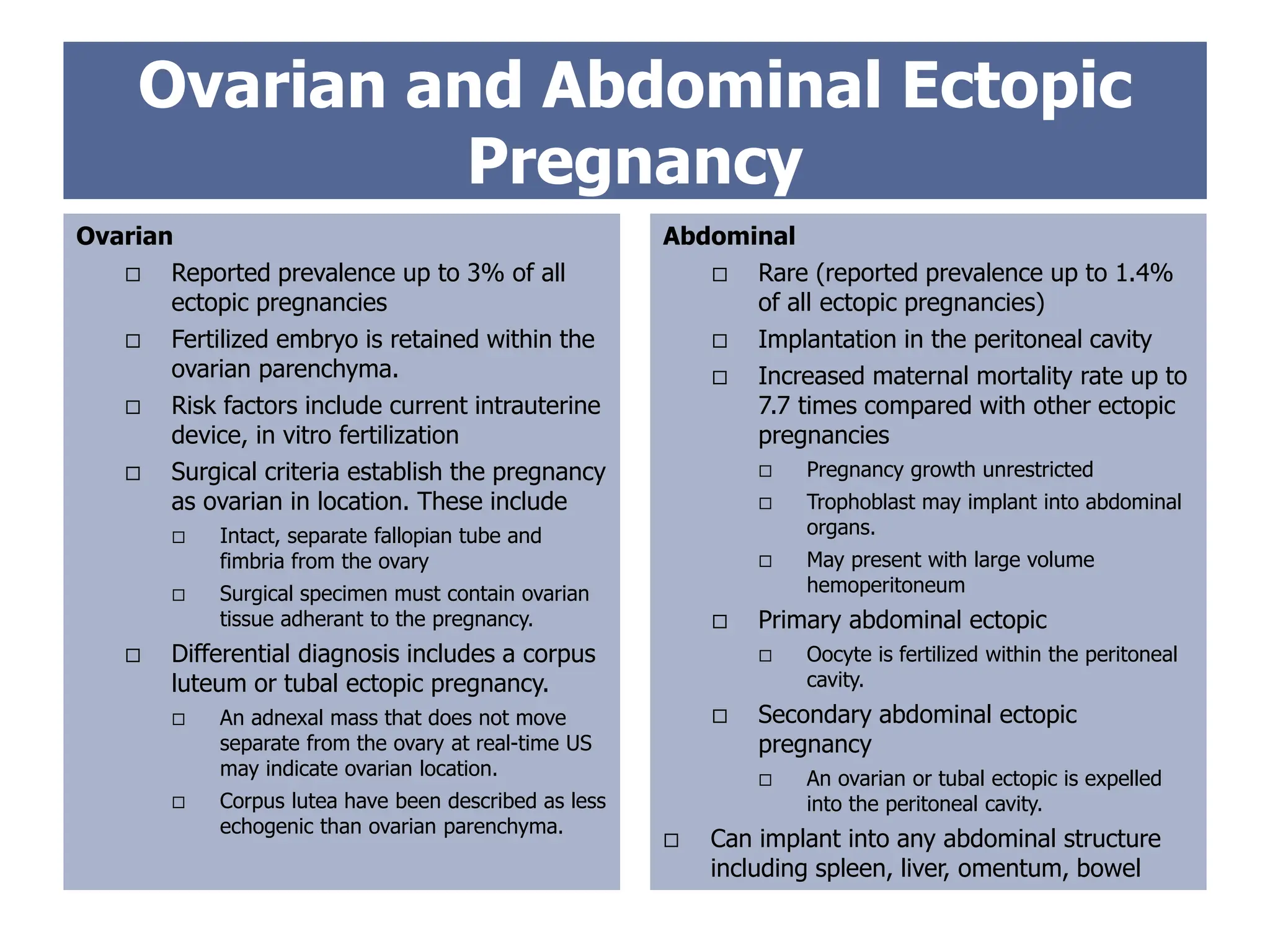
Ovarian
Reported prevalence up to 3% of all
ectopic pregnancies
Fertilized embryo is retained within the
ovarian parenchyma.
Risk factors include current intrauterine
device, in vitro fertilization
Surgical criteria establish the pregnancy
as ovarian in location. These include
Intact, separate fallopian tube and
fimbria from the ovary
Surgical specimen must contain ovarian
tissue adherant to the pregnancy.
Differential diagnosis includes a corpus
luteum or tubal ectopic pregnancy.
An adnexal mass that does not move
separate from the ovary at real-time US
may indicate ovarian location.
Corpus lutea have been described as less
echogenic than ovarian parenchyma.
Abdominal
Rare (reported prevalence up to 1.4%
of all ectopic pregnancies)
Implantation in the peritoneal cavity
Increased maternal mortality rate up to
7.7 times compared with other ectopic
pregnancies
Pregnancy growth unrestricted
Trophoblast may implant into abdominal
organs.
May present with large volume
hemoperitoneum
Primary abdominal ectopic
Oocyte is fertilized within the peritoneal
cavity.
Secondary abdominal ectopic
pregnancy
An ovarian or tubal ectopic is expelled
into the peritoneal cavity.
Can implant into any abdominal structure
including spleen, liver, omentum, bowel
30.
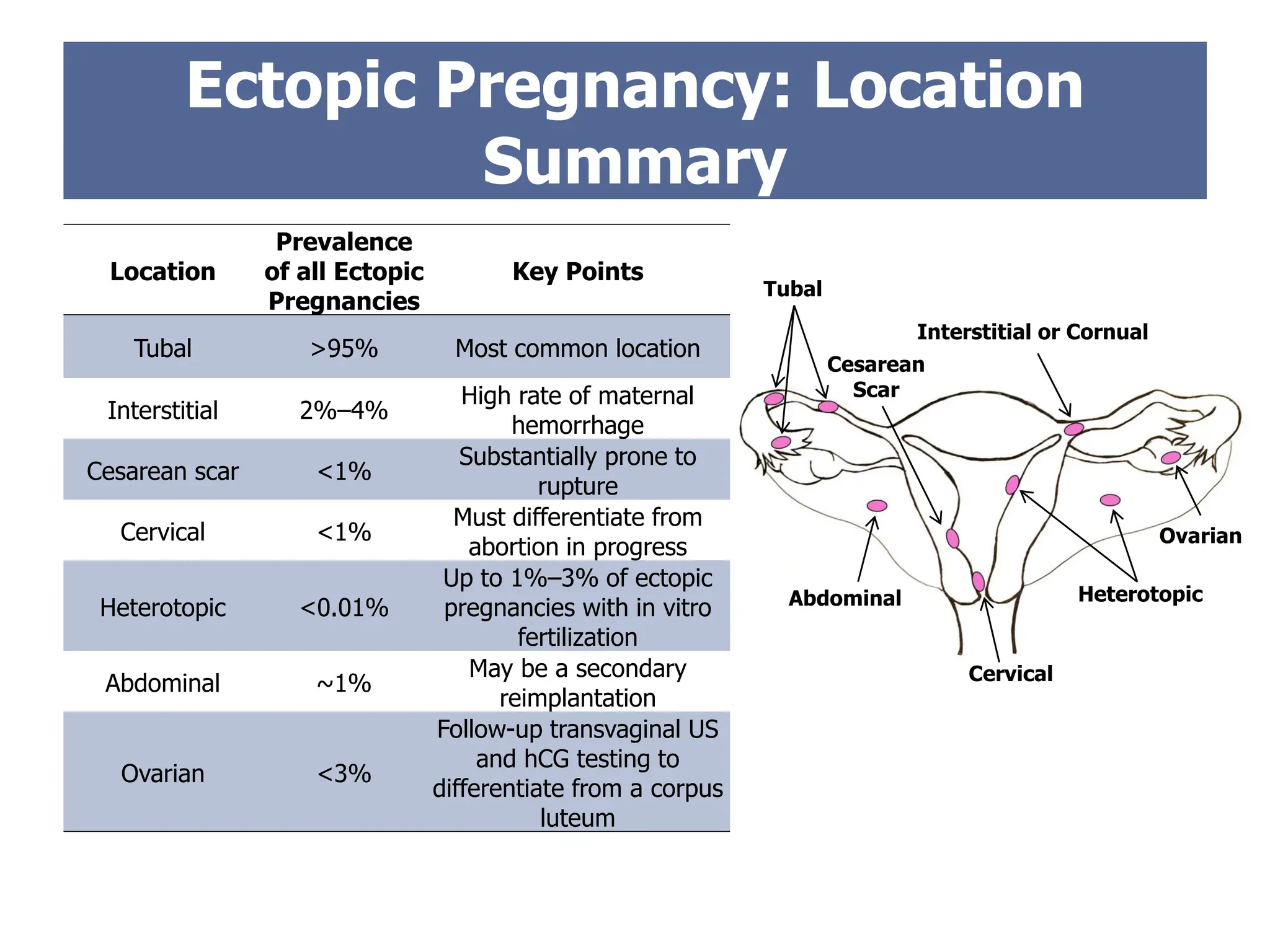
Tubal
Cervical
Abdominal
Ovarian
Cesarean
Scar
Heterotopic
Interstitial or Cornual
EctopicPregnancy: Location
Summary
Location
Prevalence
of all Ectopic
Pregnancies
Key Points
Tubal >95% Most common location
Interstitial 2%–4%
High rate of maternal
hemorrhage
Cesarean scar <1%
Substantially prone to
rupture
Cervical <1%
Must differentiate from
abortion in progress
Heterotopic <0.01%
Up to 1%–3% of ectopic
pregnancies with in vitro
fertilization
Abdominal ~1%
May be a secondary
reimplantation
Ovarian <3%
Follow-up transvaginal US
and hCG testing to
differentiate from a corpus
luteum
31.
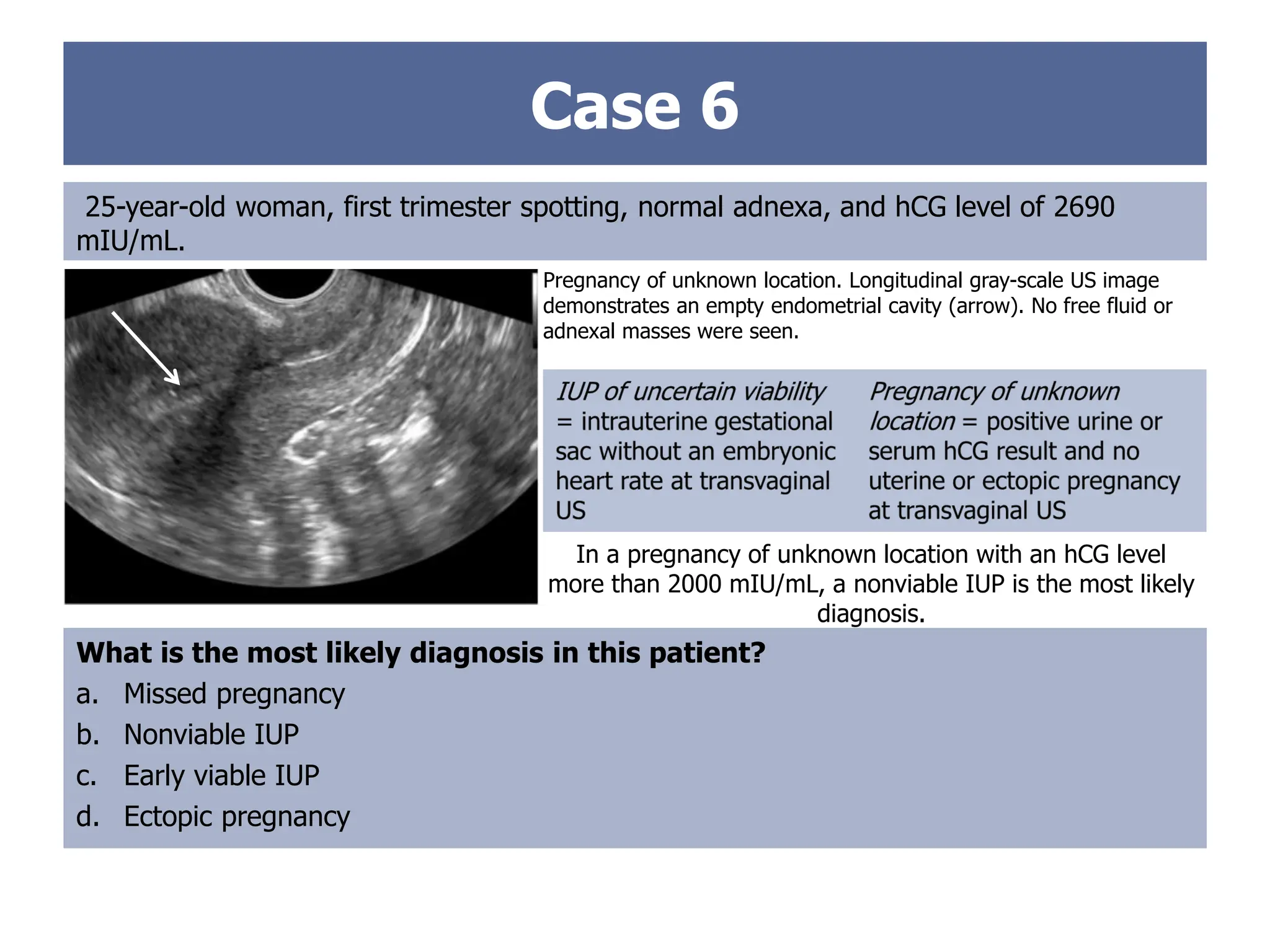
Case 6
25-year-old woman,first trimester spotting, normal adnexa, and hCG level of 2690
mIU/mL.
Pregnancy of unknown location. Longitudinal gray-scale US image
demonstrates an empty endometrial cavity (arrow). No free fluid or
adnexal masses were seen.
What is the most likely diagnosis in this patient?
a. Missed pregnancy
b. Nonviable IUP
c. Early viable IUP
d. Ectopic pregnancy
In a pregnancy of unknown location with an hCG level
more than 2000 mIU/mL, a nonviable IUP is the most likely
diagnosis.
32.
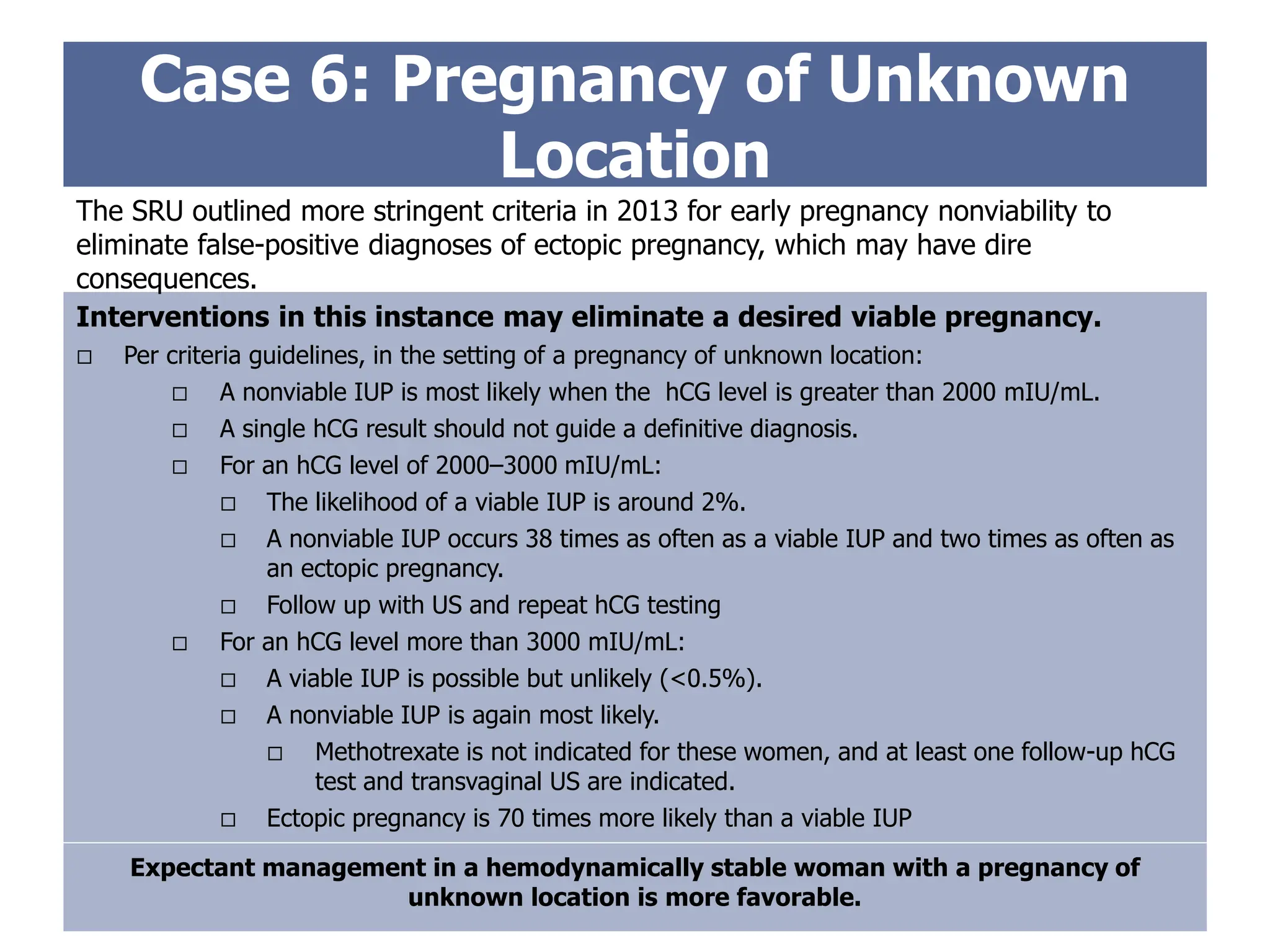
Case 6: Pregnancyof Unknown
Location
Interventions in this instance may eliminate a desired viable pregnancy.
Per criteria guidelines, in the setting of a pregnancy of unknown location:
A nonviable IUP is most likely when the hCG level is greater than 2000 mIU/mL.
A single hCG result should not guide a definitive diagnosis.
For an hCG level of 2000–3000 mIU/mL:
The likelihood of a viable IUP is around 2%.
A nonviable IUP occurs 38 times as often as a viable IUP and two times as often as
an ectopic pregnancy.
Follow up with US and repeat hCG testing
For an hCG level more than 3000 mIU/mL:
A viable IUP is possible but unlikely (<0.5%).
A nonviable IUP is again most likely.
Methotrexate is not indicated for these women, and at least one follow-up hCG
test and transvaginal US are indicated.
Ectopic pregnancy is 70 times more likely than a viable IUP
The SRU outlined more stringent criteria in 2013 for early pregnancy nonviability to
eliminate false-positive diagnoses of ectopic pregnancy, which may have dire
consequences.
Expectant management in a hemodynamically stable woman with a pregnancy of
unknown location is more favorable.
33.
Case 6: Pregnancyof Unknown
Location
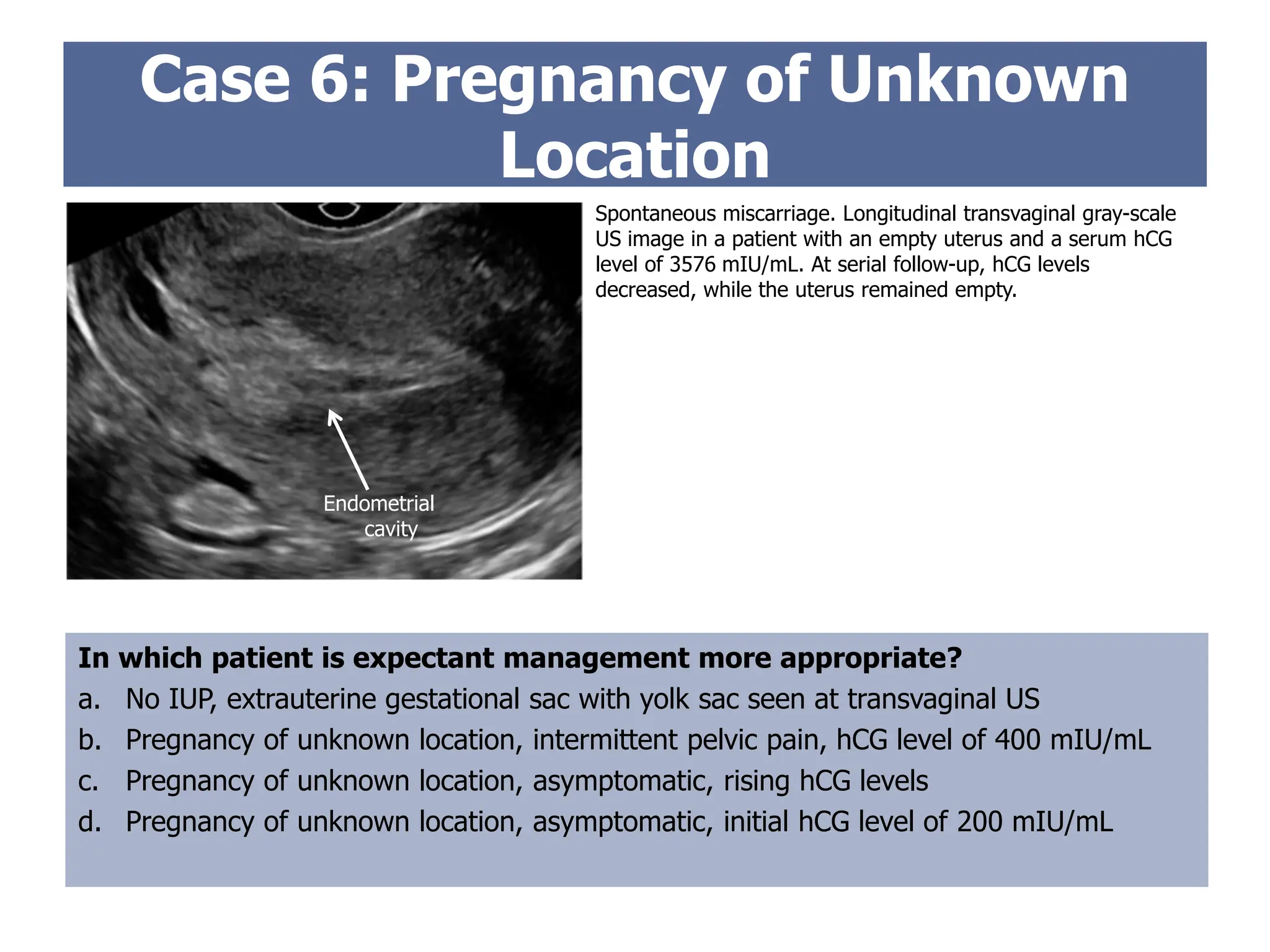
In which patient is expectant management more appropriate?
a. No IUP, extrauterine gestational sac with yolk sac seen at transvaginal US
b. Pregnancy of unknown location, intermittent pelvic pain, hCG level of 400 mIU/mL
c. Pregnancy of unknown location, asymptomatic, rising hCG levels
d. Pregnancy of unknown location, asymptomatic, initial hCG level of 200 mIU/mL
Spontaneous miscarriage. Longitudinal transvaginal gray-scale
US image in a patient with an empty uterus and a serum hCG
level of 3576 mIU/mL. At serial follow-up, hCG levels
decreased, while the uterus remained empty.
Endometrial
cavity
34.
Ectopic Pregnancy: Expectant
Management
Selectpatients with a pregnancy of unknown location in whom the risk for tubal rupture
is low can successfully be managed expectantly without medical or surgical intervention.
Expectant management
Careful patient selection
Typically
Asymptomatic
Evidence of pregnancy resolution
Per 2008 American Congress of Obstetricians and Gynecologists guidelines, generally manifested by
decreasing hCG levels
Accept the risks of tubal rupture and hemorrhage
Best candidates have tubal gestations with low hCG values.
If hCG level is less than 200 mIU/mL, spontaneous resolution is reportedly as high as 88%.
With increased pain, hemorrhage, or increasing or stable hCG levels,
expectant management should be avoided.
Extensive counseling, serial hCG testing every 48 hours, and transvaginal US
are required.
35.
Options include
Surgery(open or laparoscopic)
Medical therapy with methotrexate (folic acid antagonist)
Expectant management
A 2007 Cochrane review and 2008 meta-analysis found no difference in success rate or tubal
patency or subsequent fertility rates comparing methotrexate with laparoscopic salpingostomy.
Ectopic Pregnancy: Treatment
Surgical options
Salpingectomy
Salpingostomy
Preferred over
salpingectomy for a
patient who desires future
fertility
Laparotomy can generally be
avoided.
Reserved for acute
manifestations, including
hemodynamic instability
or poor visualization at
the time of laparoscopy
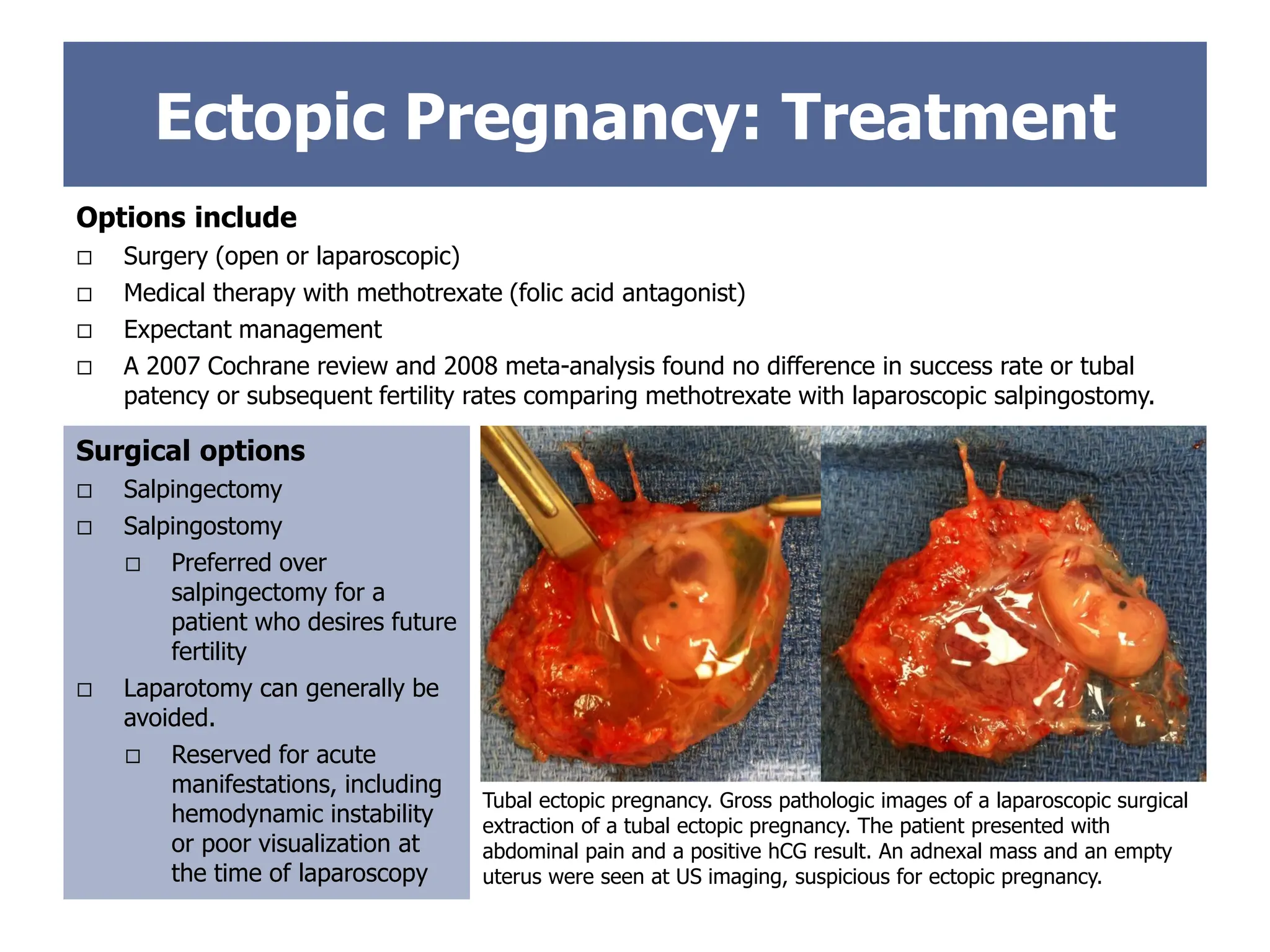
Tubal ectopic pregnancy. Gross pathologic images of a laparoscopic surgical
extraction of a tubal ectopic pregnancy. The patient presented with
abdominal pain and a positive hCG result. An adnexal mass and an empty
uterus were seen at US imaging, suspicious for ectopic pregnancy.
36.
Endometrial
Cavity
Endometrial
Cavity
Cervical
Ectopic
Ectopic Pregnancy: Treatment
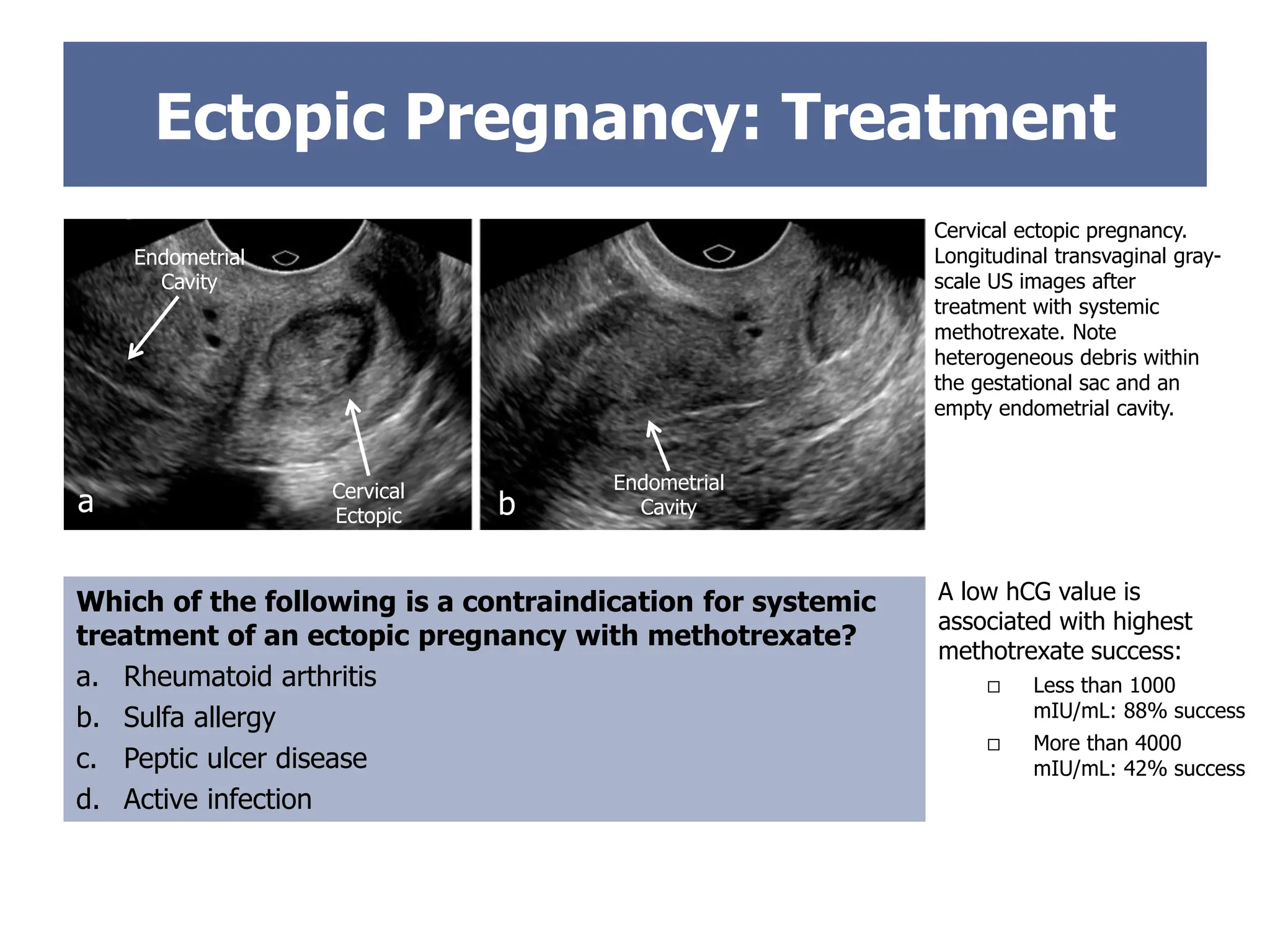
Whichof the following is a contraindication for systemic
treatment of an ectopic pregnancy with methotrexate?
a. Rheumatoid arthritis
b. Sulfa allergy
c. Peptic ulcer disease
d. Active infection
Cervical ectopic pregnancy.
Longitudinal transvaginal gray-
scale US images after
treatment with systemic
methotrexate. Note
heterogeneous debris within
the gestational sac and an
empty endometrial cavity.
a b
A low hCG value is
associated with highest
methotrexate success:
Less than 1000
mIU/mL: 88% success
More than 4000
mIU/mL: 42% success
37.
Ectopic Pregnancy: Systemic
Methotrexate
Benefits
Cost effective
Less invasive
Avoid risks of surgery and anesthesia
Side effects
Nausea and abdominal pain
Fatigue
Hepatotoxicity
Pulmonary fibrosis and renal failure
(rare)
Laboratory tests repeated after 1
week to assess renal and hepatic
function
Relative contraindications
Positive embryonic cardiac activity
Gestational sac more than 3.5 cm
Absolute contraindications
Active pulmonary disease
Peptic ulcer disease
Renal impairment (glomerular
filtration rate less than 50
mL/min/1.73 m2)
Hematologic dyscrasia
Immunosuppression
Alcoholism or liver failure
Breastfeeding
Methotrexate is a dihydrofolate reductase inhibitor that inhibits DNA synthesis.
Overall success rates of systemic methotrexate for ectopic pregnancy are reported to
range from 71.2% to 94.2%.
Candidates for systemic methotrexate should be hemodynamically stable, have an
unruptured mass, and be able to appropriately follow up.
May be given as a single dose, two doses, or a fixed multidose intramuscular regimen
Systemic methotrexate is an option after surgical management failure.
38.
Ectopic Pregnancy: Local
Treatment
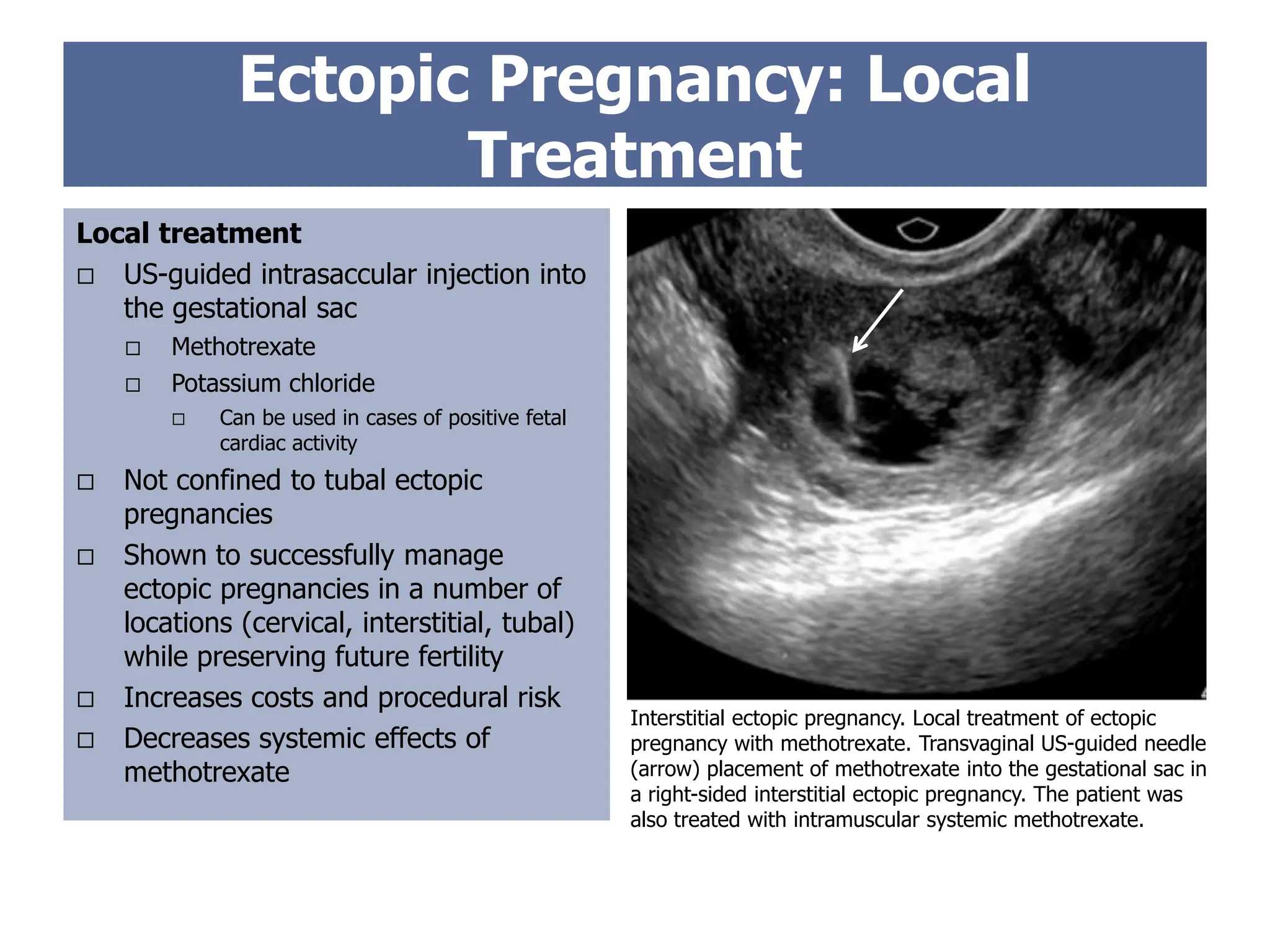
Interstitialectopic pregnancy. Local treatment of ectopic
pregnancy with methotrexate. Transvaginal US-guided needle
(arrow) placement of methotrexate into the gestational sac in
a right-sided interstitial ectopic pregnancy. The patient was
also treated with intramuscular systemic methotrexate.
Local treatment
US-guided intrasaccular injection into
the gestational sac
Methotrexate
Potassium chloride
Can be used in cases of positive fetal
cardiac activity
Not confined to tubal ectopic
pregnancies
Shown to successfully manage
ectopic pregnancies in a number of
locations (cervical, interstitial, tubal)
while preserving future fertility
Increases costs and procedural risk
Decreases systemic effects of
methotrexate
39.
Rule-out ectopicpregnancy is a common indication for pelvic US in the
emergency department.
Risks of incorrect diagnoses are high, as ectopic pregnancy can result in
maternal exsanguination and death.
Radiology trainees are on the front line to provide early diagnosis for these
patients and guide them toward rapid treatment.
Summary
Understanding the spectrum and pattern of findings seen in ectopic
pregnancy can help the radiologist and radiology trainee determine a
definitive diagnosis and guide early patient management.
40.
1. Ackerman TE,Levi CS, Dashefsky SM, Holt SC, Lindsay DJ. Interstitial line: sonographic finding in interstitial (cornual) ectopic pregnancy. Radiology 1993;189(1):83-87.
2. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 94. Medical management of ectopic pregnancy. Obstet Gynecol 2008;111(6):1479-1485.
3. Ankum WM, Mol BW, van der Veen F, Bossuyt PM. Risk factors for ectopic pregnancy: a meta-analysis. Fertil Steril 1996;65:1093-1099.
4. Ash A, Smith A, Maxwell D. Caesarean scar pregnancy. BJOG 2007;114(3):253-263.
5. Atri M, Chow CM, Kintzen G, Gillett P, Aldis AA, Thibodeau M, Reinhold C, Bret PM. Expectant treatment of ectopic pregnancies: clinical and sonographic predictors. AJR Am J
Roentgenol 2001;176(1):123-127.
6. Atrash HK, Friede A, Hogue CJ. Abdominal pregnancy in the United States: frequency and maternal mortality. Obstet Gynecol 1987;69(3 Pt 1):333–337.
7. Barash JH, Buchanan EM, Hillson C. Diagnosis and management of ectopic pregnancy. Am Fam Physician 2014;90(1):34-40.
8. Bouyer J, Coste J, Shojaei T, et al. Risk factors for ectopic pregnancy: a comprehensive analysis based on a large case-control, population-based study in France. Am J
Epidemiol 2003;157(3):185-194.
9. Centers for Disease Control and Prevention. Ectopic pregnancy: United States, 1990-1992. MMWR Morb Mortal Wkly Rep 1995;44(3):46–48.
10. Comstock C, Huston K, Lee W. The ultrasonographic appearance of ovarian ectopic pregnancies. Obstet Gynecol 2005;105(1):42-45.
11. Chukus A, Tirada N, Restrepo R, Reddy NI. Uncommon implantation sites of ectopic pregnancy: thinking beyond the complex adnexal mass. RadioGraphics 2015;35(3):946-
959.
12. Dibble EH, Lourenco AP. Imaging unusual pregnancy implantations: rare ectopic pregnancies and more. AJR Am J Roentgenol 2016;30:1-13.
13. Doubilet PM, Benson CB, Bourne T, Blaivas M; Society of Radiologists in Ultrasound Multispecialty Panel on Early First Trimester Diagnosis of Miscarriage and Exclusion of a
Viable Intrauterine Pregnancy, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med 2013;369(15):1443-1451.
14. Doubilet PM, Benson CB. Double sac sign and intradecidual sign in early pregnancy: interobserver reliability and frequency of occurrence. J Ultrasound Med 2013;32(7):1207-
1214.
15. Doubilet PM. Ultrasound evaluation of the first trimester. Radiol Clin North Am 2014;52(6):1191-1199.
16. Hajenius PJ, Mol F, Mol BW, Bossuyt PM, Ankum WM, van der Veen F. Interventions for tubal ectopic pregnancy. Cochrane Database Syst Rev 2007;(1):CD000324.
17. Kirk E, Bottomley C, Bourne T. Diagnosing ectopic pregnancy and current concepts in the management of pregnancy of unknown location. Hum Reprod Update
2014;20(2):250-261.
18. Lau S, Tulandi T. Conservative medical and surgical management of interstitial ectopic pregnancy. Fertil Steril 1999;72(2):207-215.
19. Levine D. Ectopic pregnancy. Radiology 2007;245(2):385-397.
20. Lewiss RE, Shaukat NM, Saul T. The endomyometrial thickness measurement for abnormal implantation evaluation by pelvic sonography. J Ultrasound Med 2014;33(7):1143-
1146.
21. Lin EP, Bhatt S, Dogra VS. Diagnostic clues to ectopic pregnancy. RadioGraphics 2008;28(6):1661-1671.
22. Marion LL, Meeks GR. Ectopic pregnancy: history, incidence, epidemiology, and risk factors. Clin Obstet Gynecol 2012;55(2):376-386.
23. Mol F, Mol BW, Ankum WM, van der Veen F, Hajenius PJ. Current evidence on surgery, systemic methotrexate and expectant management in the treatment of tubal ectopic
pregnancy: a systematic review and meta-analysis. Hum Reprod Update 2008;14(4):309-319.
24. Murray H, Baakdah H, Bardell T, Tulandi T. Diagnosis and treatment of ectopic pregnancy. CMAJ 2005;173(8):905-912.
25. Parker RA 3rd, Yano M, Tai AW, Friedman M, Narra VR, Menias CO. MR imaging findings of ectopic pregnancy: a pictorial review. RadioGraphics 2012;32(5):1445-1460.
26. Perkins KM, Boulet SL, Kissin DM, Jamieson DJ;National ART Surveillance (NASS) Group. Risk of ectopic pregnancy associated with assisted reproductive technology in the
United States, 2001-2011. Obstet Gynecol 2015;125(1):70-78.
Suggested Readings