Downloaded 20 times






















































![52
Drug-Free ASEAN 2015: Status and Recommendations
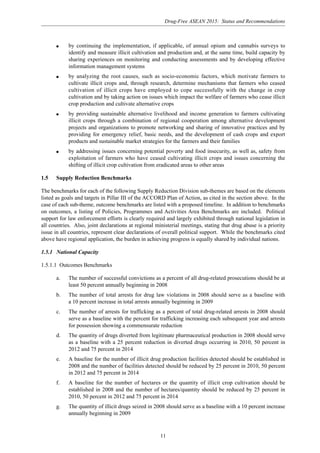
Prevention and Education Treatment and Rehabilitation Addressing HIV/AIDS
q A working group in place and set
of guiding principles adopted and
distributed for prevention activities.
Creation of materials to support the
guiding principles is underway
q Inventory and assessment of
NGOs active in drug control is
underway but there is no budgetary
support
q No trial treatment programmes in
prison have been initiated but plans are
under development
q Legal provisions permit
access to voluntary treatment
programmes but not to treatment
as an alternative to criminal
charges
q Some support for various
methodologies for HIV/AIDS
infection prevention – activities
in this area are mainly
implemented by NGOs
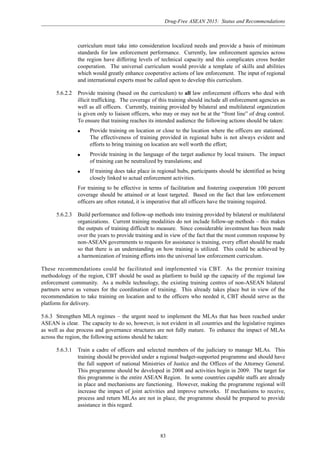
Demand Reduction projects and programmes by international organizations
Organization Project/Activity
Coverage and Budget and
Key Partner Duration
AusAID HIV/AIDS Asia Regional Programme (HAARP) National coverage to
be determined
Regional and
national
organizations and
NGOs
Total budget
US$51.6 m –
country specific
budget not yet
determined
2007-2015
US$15 million
2002-2007
Asia Regional HIV/AIDS Project (ARHP)
[closed]
School-Based Healthy Living and HIV/AIDS
Prevention Education Programme (SHAPE) –
focuses on a range of health and social issues
relevant to children and young people, including
HIV/AIDS, hygiene, alcohol and drugs. SHAPE
Plus – extension of project targeting
out-of-school youth
UNICEF 1998 – ongoing
USAID NA
3.1.7 Philippines
Summary of National Plan
Established under the Republic Act No. 6425, which is also known as the Dangerous Drugs Act of 1972,
the Dangerous Drugs Board (DDB) of the Philippines was set up to facilitate the pursuit of the goal of
a drug-free and prosperous Philippines by eradicating the supply and demand for dangerous drugs and
precursor chemicals. The multi-disciplinary DDB has 17 members, of which three are permanent, and is
lead by a Chairman (Secretary) appointed by the President of the Philippines from among the three
Permanent Members. For more information see Annex 1 G.
Included in the
national curriculum
in Myanmar,
reaching 1.9 million
children in 14,000
schools
Ministry of
Education
Kachin StateUSAID supports Médecins du Monde who target
IDUs; providing training for health personnel on
prevention and drug treatment issues; outreach to
families for HIV prevention and drug abuse
education; counseling support for IDUs](https://image.slidesharecdn.com/drugfreeasean2015-150430083453-conversion-gate01/85/Drug-free-asean-2015-61-320.jpg)







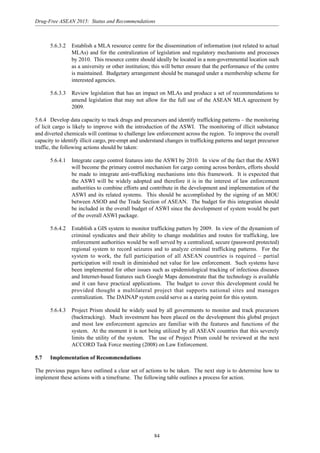
![60
Drug-Free ASEAN 2015: Status and Recommendations
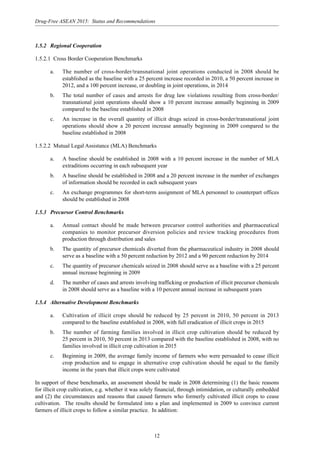
Prevention and Education Treatment and Rehabilitation Addressing HIV/AIDS
q Plan for ATS policies waiting for
analysis with ATS prevention focus
is on large cities
q Benchmarks are being developed
in the context of the national action
plan
q NGOs (mass organizations)
working group has been established
and an inventory and assessment of
NGO activities pending
authority – at present focus is on
drug prevention
q Review under consideration for
the provision of treatment in
custodial settings. Training
materials being developed – what
exists has be created by NGOs
Demand Reduction projects and programmes by international organizations
Organization Project/Activity
Coverage and Budget and
Key Partner Duration
AusAID HIV/AIDS Asia Regional Programme (HAARP) National coverage
to be determined
Regional
organizations and
NGOs
Total budget
US$51.6 m –
country specific
budget not yet
determined
2007-2015
US$15 million
2002-2007
Myanmar, Viet Nam
and two regions of
China
NA
Asia Regional HIV/AIDS Project (ARHP)
[closed] Implemented in Viet Nam by UNDP
Family Health
International
Under different programmes fund UNDP and
UNODC drug demand reduction projects, as well
as HIV/AIDS prevention activities by CARE
Australia and the Australian Red Cross and
several projects through the STD/HIV/AIDS
Centre (SHAPC)
Harm reduction activities, including drop in
centre, counseling and pilot methadone project.
Outreach activities for drug abusers and their
families. 1998-2004 part of IMPACT, 2004-2008
funded through PEPFAR
NA
Five provinces
Ho Chi Minh city,
Can Tho, An Giang,
Hai Phong, and
Quang Ninh,
planned expansion
of 2 provinces by
end 2007.
Viet Nam
Administration for
HIV/AIDS
Prevention and
Control, Provincial
health centres and
District preventative
medicine centres
1998-2008](https://image.slidesharecdn.com/drugfreeasean2015-150430083453-conversion-gate01/85/Drug-free-asean-2015-69-320.jpg)
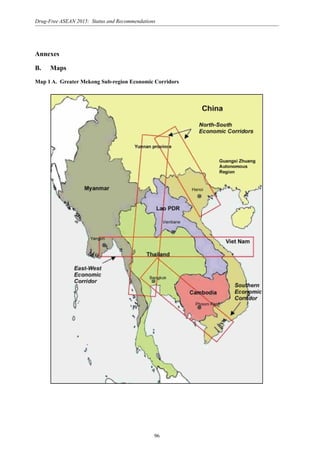
![Drug-Free ASEAN 2015: Status and Recommendations
61
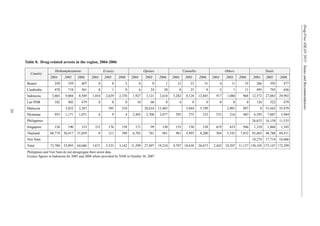
Organization Project/Activity
Coverage and Budget and
Key Partner Duration
UNDP Community-based Awareness Raising and
Behavioural Change for Vietnamese Youth
Project [closed] – build capacity for the Viet Nam
Youth Union (VYU) to implement HIV/AIDS
education and awareness activities, targeting
young people practicing high risk behaviour
Five Provinces; Ha
Tinh, Son La, Can
Tho, Hau Giang and
Tay Ninh.
Ministry of Labour,
Invalids and Social
Affairs (MOLISA),
Department of
Social Evil
Prevention
US$860,000
2001-2004
Reducing drug use and delinquency among youth
in the Greater Mekong Sub-region (Phase III):
Health systems development and policy reform
project
Total budget
US$450,000 –
country specific
budget not
ascertained
2007-2009
2006-2010
UNESCAP
Ministry of
Education
Drug information component in the Healthy
living and life skills project implemented by
Ministry of Education with support from
UNICEF in schools as extra curricular activity for
ages 10-14
See regional section
President’s Emergency Plan for AIDS Relief
(PEPFAR)
Viet Nam became a PEPFAR focus country in
June 2004
Proposed project – Building comprehensive harm
reduction services for IDUs in Cambodia, the Lao
PDR and Viet Nam: Towards universal access to
HIV/AIDS prevention, treatment and care – build
regional capacity in the health sector for the
prevention and reduction of HIV related harm
among IDUs. See regional section
UNICEF
Ministry of Health/
FHI
FY 2004-2006,
US$79 m FY 2007,
US$65.8 m 2003 –
ongoing
USAID
WHO/SIDA National coverage
to be determined
Ministry of Health
Total budget
US$2.3 m – country
specific budget not
ascertained
Planned 2007-2008](https://image.slidesharecdn.com/drugfreeasean2015-150430083453-conversion-gate01/85/Drug-free-asean-2015-70-320.jpg)













































This document provides a summary of the report "Drug-Free ASEAN 2015: Status and Recommendations". The report assesses the feasibility of achieving a drug-free ASEAN by 2015. It addresses whether the commitment is achievable, if the region is on track, and what can be done to accelerate progress. The report establishes benchmarks for supply and demand reduction efforts. It reviews the regional drug situation in 2000 and 2006 based on available data. Response gaps are identified and recommendations are proposed to strengthen national capacity, regional cooperation, precursor control, and demand reduction initiatives. Emerging challenges to achieving a drug-free ASEAN by 2015 due to factors like porous borders and increased trade and transport are also discussed.




























































