Premium Call Girls Cottonpet Whatsapp 7001035870 Independent Escort Service
Congenital Diaphragmatic Hernia.pptx
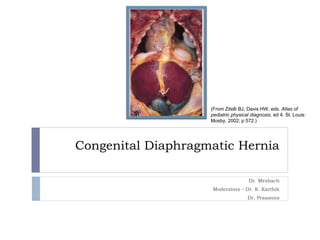
1. Congenital Diaphragmatic Hernia
Dr. Meshach
Moderators – Dr. K. Karthik
Dr. Prasanna
(From Zitelli BJ, Davis HW, eds. Atlas of
pediatric physical diagnosis, ed 4. St. Louis:
Mosby, 2002; p 572.)
3. Introduction
Congenital diaphragmatic hernia results when
intraabdominal organs extrude into the thoracic cavity
secondary to failure of development of the diaphragm
early in gestation
In utero, CDH evolves into a disorder of lung
development - pulmonary hypoplasia and abnormal
vasculature.
CDH may be an isolated lesion, but approximately 40% of
cases are associated with other anomalies, including 20%
with congenital heart disease
4. Embryology
Smith's Anesthesia for Infants and Children
9th Edition
Authors: Peter Davis Franklyn Cladis
P 587
https://obgynkey.com/gastroenterology-2/ Fig. 14.1
5. Pathophysiology
Midgut is commonly herniated but in some cases
stomach, descending colon, left kidney and left lobe
of liver can also be herniated
Pulmonary hypoplasia occurs that depends upon the
timing of herniation and degree of compression
during fetal development
The contralateral lung can also be affected
6. Pathophysiology
Fewer alveoli with
thickened walls
Smaller alveolar gas
exchange surface area
Decreased vasculature
Hyperplasia of medial
layer
Extension of smooth
muscle layer of alveoli
into the intra acinar
arterioles
Pulmonary
Hypertension
Pulmonary
Hypoplasia
Right Left
PDA
PFO
8. Prenatal Management
Diagnosis
USG - On routine ultrasound, the most common findings
include displacement of the heart and fluid-filled bowel in
the thorax, and, in some cases, herniation of the liver
Severity assessment
USG and MRI are relevant to predicting severity of the
CDH.
Severity depends on the Lung size and presence of liver
position
LHR – Lung to Head Ratio (Contralateral lung) and
presence or absence of liver in the thorax
Assessing vascularization – Contralateral vascularization
index
9. Prenatal Management
Tracheal Occlusion Procedure
Preventing lung fluid from exiting the lung, tracheal
occlusion results in stretching the lung to accelerate
growth.
The increased intrathoracic pressure tends to move
the viscera out of the thorax
11. Preoperative Management
Postnatal diagnosis
The classic triad of CDH consists of cyanosis, dyspnea,
and apparent dextrocardia.
scaphoid abdomen,
bulging chest,
decreased breath sounds,
distant or right-displaced heart sounds, and
bowel sounds in the chest.
CXR shows air filler viscera in chest with mediastinal shift
12. Preoperative Management
Postnatal Management
NG tube to decompress stomach
Positioning the neonate in semi recumbent position with
hernia side down
Do not mask ventilate
Secure the airway by intubation with ETT and ventilate
Monitor airway pressure
Permissive hypercapnia and hypoxaemia with least
aggressive ventilation to prevent barotrauma
13. Preoperative Management
antenatal diagnosis,
neonatal stabilization
delayed surgery and
avoidance of ventilator-induced lung injury
have significantly improved morbidity and
mortality for infants with severe CDH.
16. Intraoperative Management
IV access preferentially upperlimb. In some cases
CVP may be necessary
Goals of ventilation similar to preoperative period
Prevention of hypothermia
Management of pneumothorax or pulmonary
hypertension intraoperatively
Avoid N2O as it can diffuse into the viscera and
exaggerate lung compression
Low concentration inhalation anaesthetics
Good analgesics either regional or intravenous.
18. Postoperative Management
Postoperative ventilation is planned and FiO2 is
adjusted to maintain a PaO2>150
Slowly weaned off over 48 to 72 hours
Avoid honey moon phenomenon
19. Summary
Preoperative
Intubation and ventilation
with permissive hypercapnia
Avoid bag and mask
ventilation
Nasogastric tube for stomach
decompression
Broad spectrum antibiotics
Sedation/ anaesthesia
Intraoperative
Standard monitoring
Pulse oximeter
Arterial catheter
CVP catheter
Anaesthetic agents
High dose opoids
NDMR
Ventilation
Permissive hypercapnia and
peak pressure <25cmH2O
Temperature monitoring
Forced air warmer
Postoperative
Consider Regional
anaesthesia
Continue postoperative
ventilation
Condider
NO
ECMO
21. Case History
A 23 old women G3P1L1A1 came to hospital with 9
months of amenorrhoea
POG 38weeks
Antenatal period was uneventful
Foetus diagnosed to have diaphragmatic hernia
Mother didn’t have any comorbidities and admitted for
elective LSCS
22. Case History
USG at 34 weeks of gestation
Defect of 3x2 cm noted. Defect in left
diaphragm with herniation of stomach into thoracic
cavity causing shifting of mediastinum to right.
Possibly diaphragmatic hernia
USG at 38 weeks of gestation
Single loop of cord around neck. Defect
measuring 3x3 cm seen in left diaphragm with
herniation of stomach and adjacent mesentery into left
thoracic cavity. Mediastinum shifted to right.
Congenital diaphragmatic hernia with herniation of
stomach
23. Case History
Elective LSCS done on 8th June under low dose
spinal anaesthesia
Female baby of weight 2.745 kg was born.
Baby cried immediately
APGOR score of 7/10 immediately after birth and 7/10
after 5 mins.
General appearance – fair
Good cry
Colour – Cyanosed
Moving all four limbs
24. Case History
Vitals
HR – 130/min
RR – 70/min
Spo2 in RA 80%
Subcostal Recession +
Baby shifted to NICU
Distress subsided after providing O2 via hood
25. Case History
Baby kept NPO
X – ray chest and abdomen AP view taken
Nasal oxygen by hood 2l/min
NG tube insitu and continuous aspiration done
IVF 10% Dexrose 240 ml + Sodabicarbonate 8
ml + Kcl 2 ml for 24 hours
IV antibiotics given
IV Rantac 2 mg given
Warmer care, vitals monitoring and observation
done
26. Examination
On examination
Cry fair
Colour pink
Good activity
Moving all four limbs
CVS – S1 S2 heard no
murmurs
RS – Left side air entry
reduced
No added sounds
Vitals
BP – 63/40 mmHg
HR – 123/min
SpO2 – 93% in RA
RR – 60/min
28. Anaesthetic Goals
To prevent potential hypoxia and hypotension from
distension of the stomach and bowel and due to
primary pulmonary hypoplasia
To prevent pulmonary hypertension and RV failure
by preventing hypoxia, hypercarbia and acidosis.
To provide adequate analgesia to blunt the stress
response to minimize sudden increase in PVR with
resultant increase in right to left shunt
To maintain fluid and electrolyte balance
Ventilation strategies to prevent barotrauma
29. Intraoperative
GA was planned
Machine checked
Two 24G cannula
inserted in both upper
limbs
Monitors connected:
ECG, NIBP, Pulse
oxymeter, Precordial
Stethoscope
Jackson Rees circuit
connected to machine
and checked
31. Intraoperative
Induction and Intubation
Inj. Thiopentone 10 mg
IV given
Inj. Suxamethonium
5mg IV given
Trachea intubated with
size 3 Portex tube
without cuff using size
1 Macintosh blade and
fixed at 12 cm.
33. Intra operative
Vitals
BP - 63/42 mmHg to 70/52 mmHg
HR - 120/min to 150/min
SpO2 - 100%
Fluids
Isolyte P given at 15 ml/ hour
Drugs
Inj. Paracetamol 25 mg IV given
Blood Loss
Minimal
No Complications
35. Post operative
Baby extubated after adequate reversal with Inj.
Neostigmine 1mg IV and Inj. Atropine 0.1 mg IV.
Colour pink
Moving all four limbs
Vitals
BP - 72/43 mmHg
HR - 120/min
SpO2 - 100% with 2l of Oxygen
via hood
No Complications
36. Post Operative
Baby shifted to paediatric surgery ICU
HR – 128
RR – 64/min
SpO2 – 99% with Oxygen 2l via hood
Colour pink
No Chest indrawing
37. In Paediatric ICU
Baby intubated due to persistent respiratory distress
after 12 hours of extubation
Tachypnoea, subcostal and intercostal retractions
present
Baby shifted to NICU and kept on mechanical
ventilation SIMV mode
PIP 15cmH2O, RR 60/min, PEEP 3cmH2O, FiO2 -
1