Downloaded 257 times





![GRADE HAND & FEET EYES
0 No loss of sensation
No visible deformity or damage
(Muscle power normal)
No eye problem due to
leprosy;
No evidence of visual loss
1 LOSS OF SENSATION is there
No visible deformity or damage
Eye problem due to leprosy
present, but vision not severly
affected as a result of these
(can count fingers at 6m)
2 VISIBLE DAMAGE
[loss of sensation and muscle power
weak/paralysed]
(wounds, ulcer, deformity due to
muscle weakness, loss of tissue such as
foot drop, claw hand, loss or partial
resorption of fingers/toes)
Severe vsual impairment
Vision – cannot count fingers
at 6m
Also includes lagophthalmos,
iridocyclitis and corneal
opacities.
WHO GRADING OF DISABILITIES
IN LEPROSY](https://image.slidesharecdn.com/leprosycomplications-130818162428-phpapp02/75/Complications-of-leprosy-7-2048.jpg)








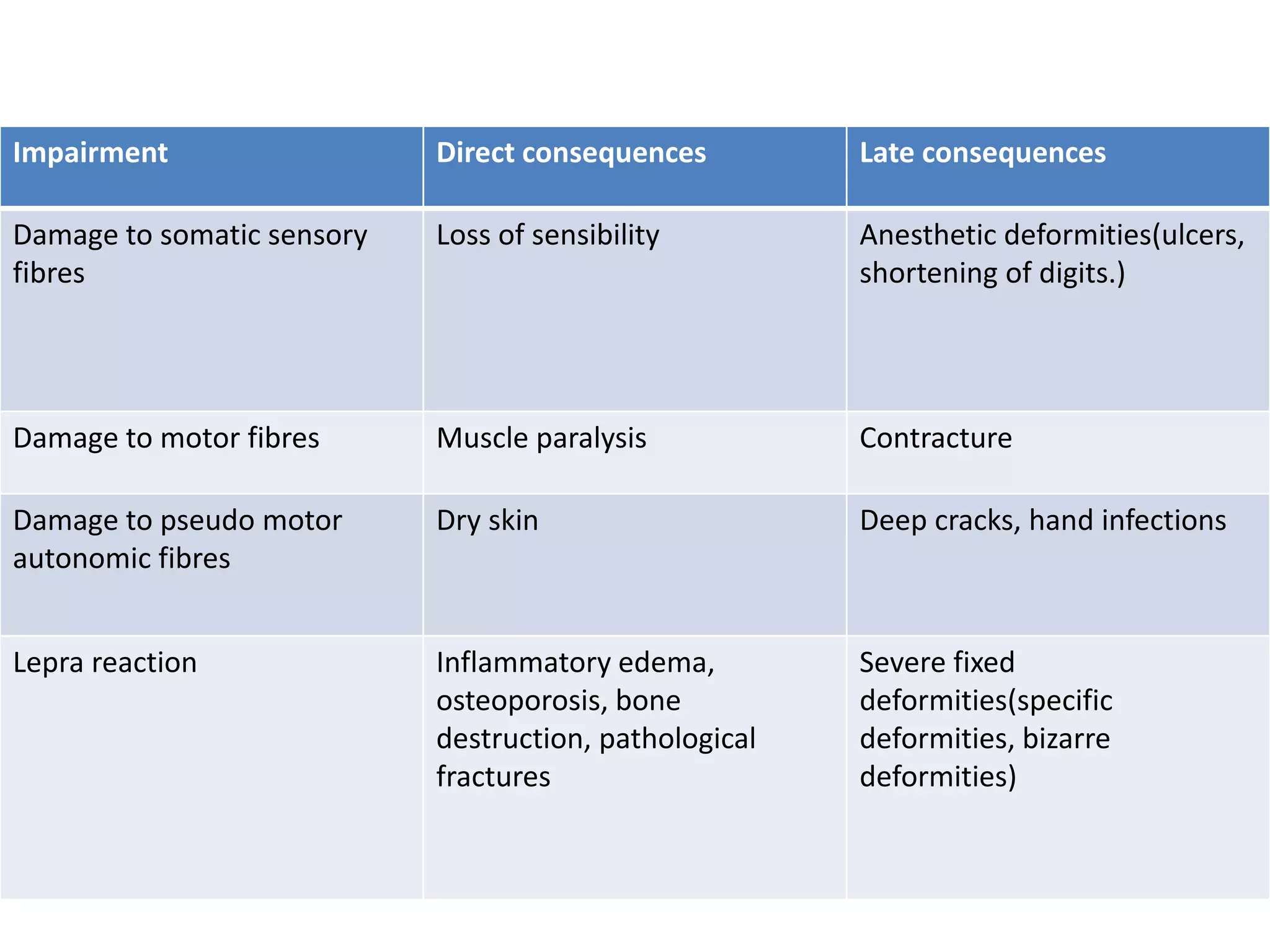

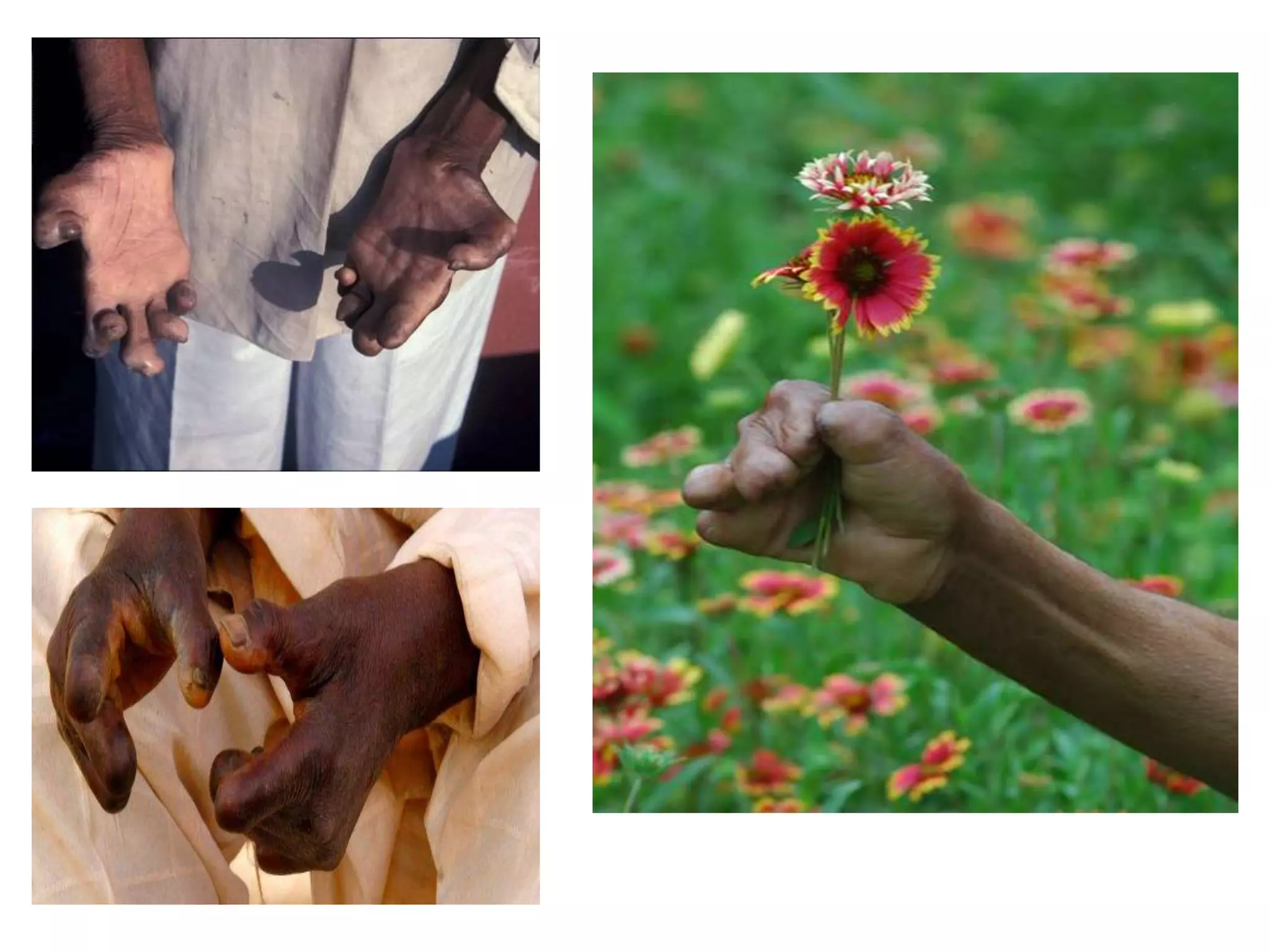
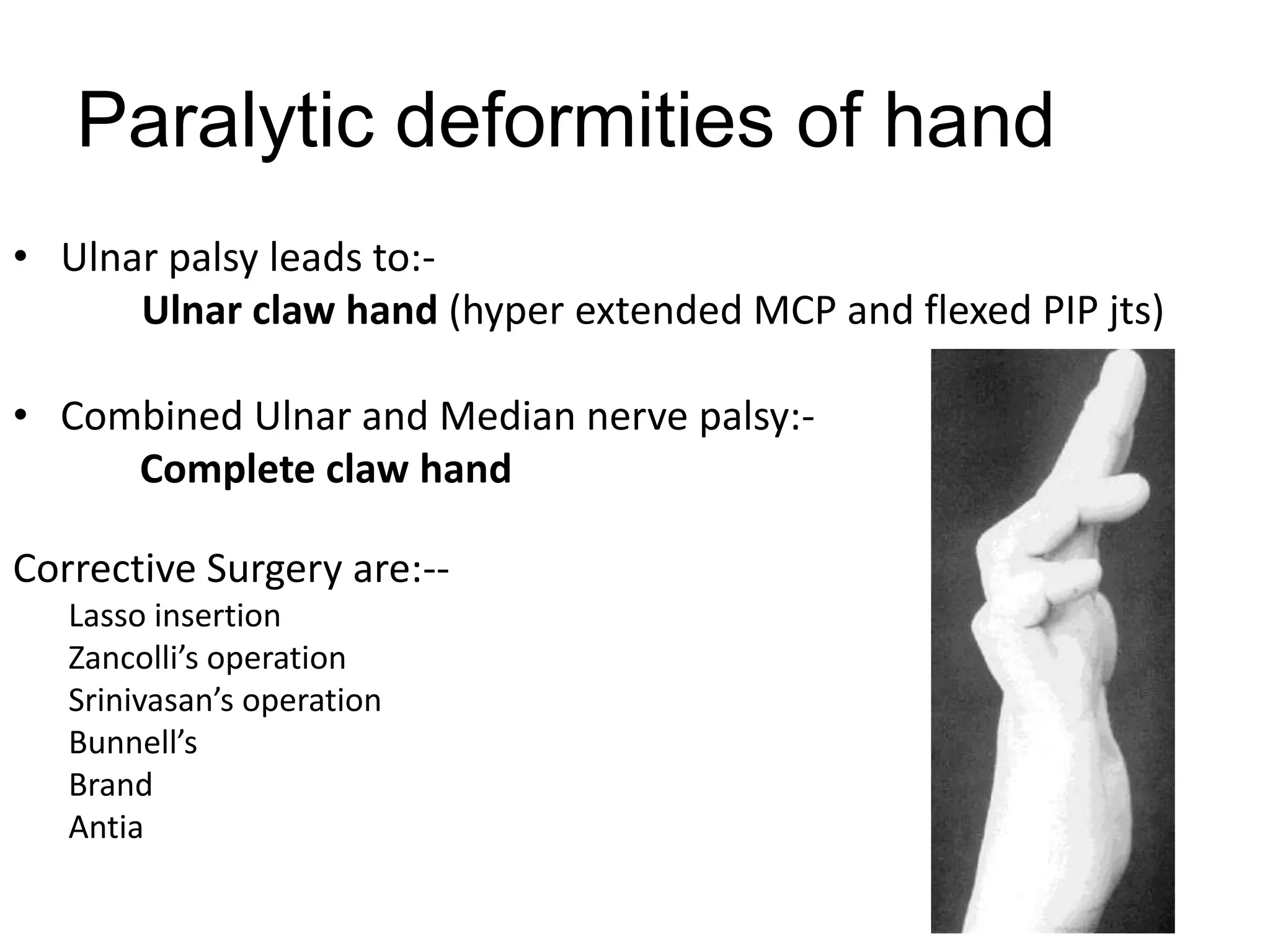
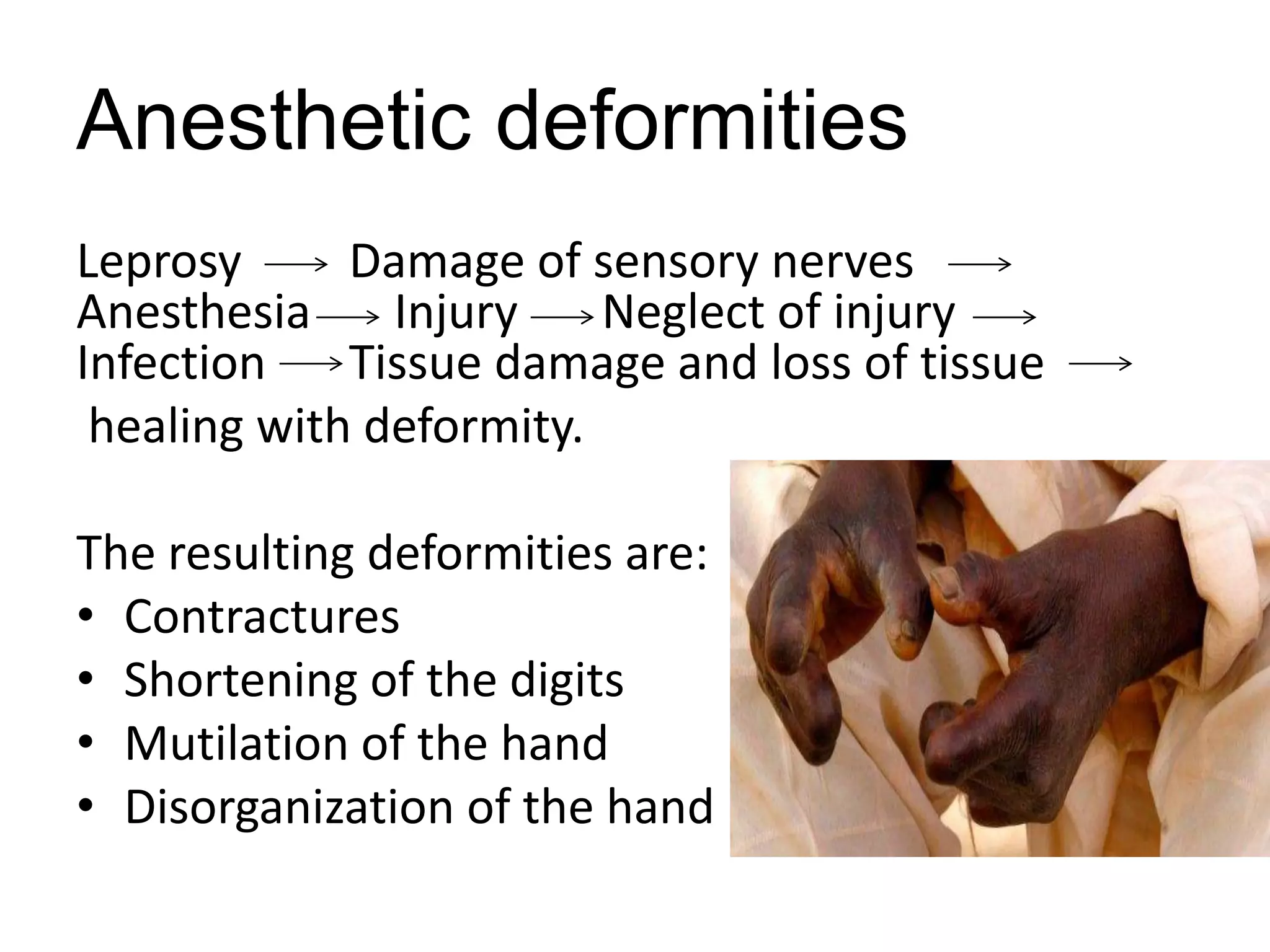













This document discusses various complications that can arise from leprosy, including: 1. Leprosy reactions which cause inflammation and damage nerves 2. Adverse effects from long-term use of anti-leprosy drugs 3. Disabilities and deformities caused by nerve damage leading to loss of sensation and muscle paralysis 4. Psycho-social problems from the stigma and rejection associated with leprosy It provides details on evaluating and grading disabilities, managing nerve damage, and treating specific issues like ulcers, clawing, eye problems, and social stigma. Surgical interventions and lifestyle adaptations are also described to prevent further impairment and support rehabilitation.










































































