Downloaded 411 times





















The document discusses various types of clinical trial designs including observational studies, uncontrolled experiments, non-randomized controlled trials, and randomized controlled trials. It provides examples of different randomized controlled trial designs such as parallel group trials, crossover trials, and cluster randomized trials. Factorial and Latin square designs are also summarized. The key advantages and disadvantages of randomized controlled trials are outlined.
An introduction to the presentation on clinical trial design by Dr. Urmila M. Aswar, focusing on pharmacology.
Classification of clinical trials: proof of concept, pilot, and pivotal studies, highlighting differences in sample sizes.
Discusses types of observational studies including cohort, case-control, cross-sectional, and case series.
Introduction to experimental trials, laying the groundwork for discussing controlled and uncontrolled designs.
Details types of experimental trials: uncontrolled, controlled, non-randomized, randomized, crossover, factorial, and Latin square.
Describes a design measuring dependent variables before and after treatment in a single test group.
Illustrates the methodology for calculating treatment effects based on before and after measurements in a trial.
Characteristics of non-randomized trials, focusing on early studies of new therapies and their challenges.
Discusses designs involving comparison between a treatment and control group without randomization.
Tests the effect of treatment by measuring outcomes in both the test group and control group.
Explains a design involving pre-treatment and post-treatment measurements in both test and control groups.
Introduction to Randomized Controlled Trials, regarded as the gold standard in clinical research.
Emphasizes the advantages of randomization including minimizing bias and improving validity of results.
Discusses necessary components of RCTs, including control groups, blinding, and the elimination of selection bias.
Lists the benefits of RCTs, including maximizing statistical power and minimizing various biases.
Highlights disadvantages of RCTs, such as recruitment difficulties, acceptability of randomization, and potential lack of generalizability.
Outlines the parallel-group trial design where participants are randomly assigned to groups for interventions.
Describes crossover design where participants receive treatments in random order over time.
Explains cluster trials involving pre-existing groups assigned to receive or not receive an intervention.
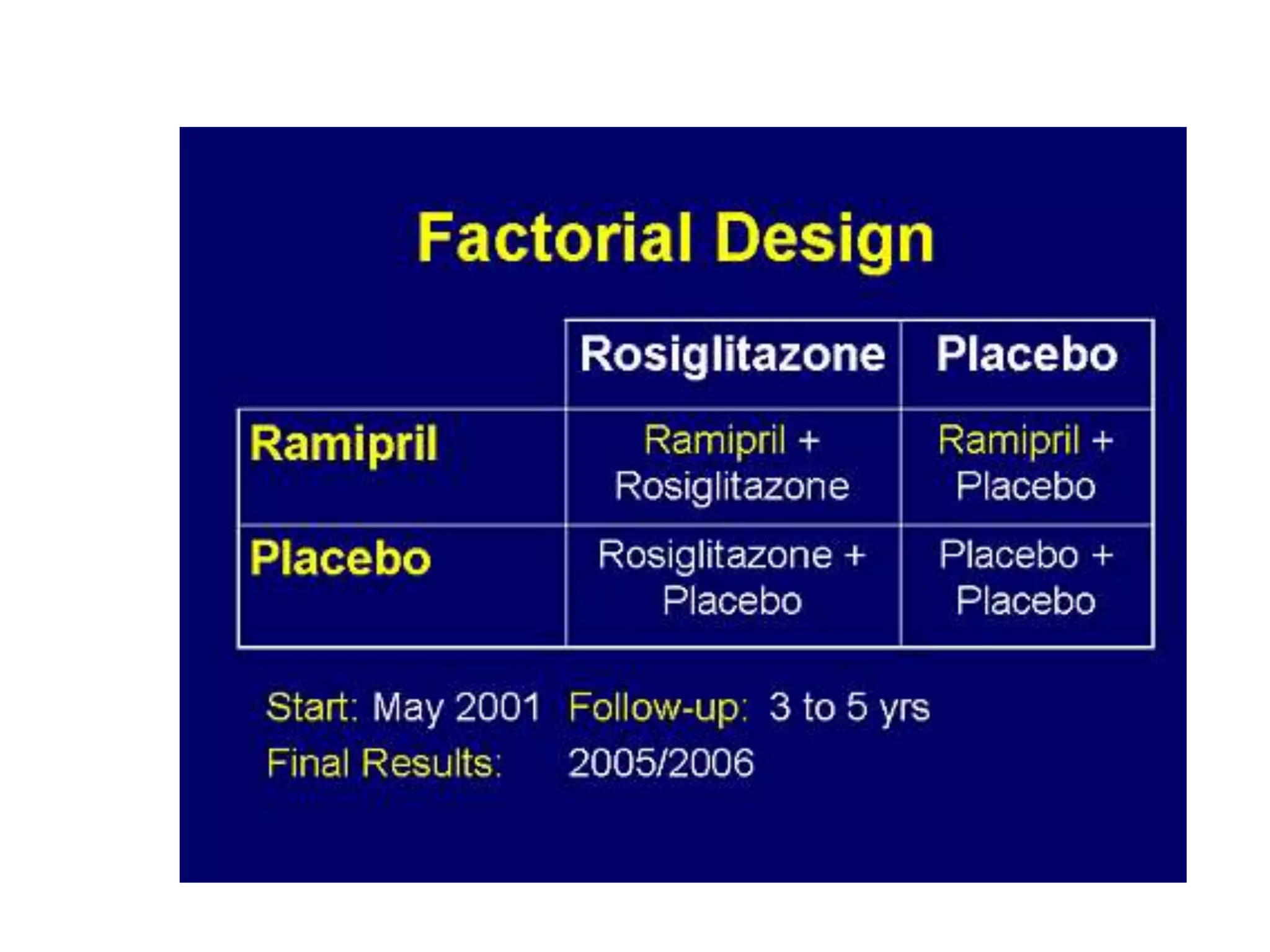
Details factorial design allowing combinations of treatments to study independent and interaction effects.
Discusses the Latin square design, explaining its structure in clinical trial designs.
Summarizes the key points discussed and introduces Zelen’s design where patients are randomized prior to consent.











































































































