Chest X-Ray and CT Images of Novel Coronavirus
•Download as PPTX, PDF•
1 like•141 views

The images are courtesy of Elsevier's STATdx at https://www.statdx.com/. Chest radiographs and Axial CECT of patients presenting with COVID-19.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Chest X-Ray and CT Images of Novel Coronavirus
Similar to Chest X-Ray and CT Images of Novel Coronavirus (20)
Recently uploaded
Recently uploaded (20)
Chest X-Ray and CT Images of Novel Coronavirus
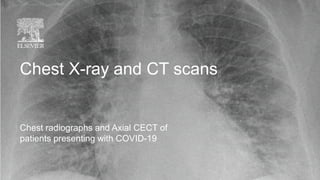
- 1. Chest X-ray and CT scans Chest radiographs and Axial CECT of patients presenting with COVID-19
- 2. April 9, 2020 We’d like to thank Drs. Santiago Martínez- Jiménez, MD, Melissa Rosado de Christenson, MD, FACR, and Sherief Garrana, MD for providing the images found in this document.
- 3. AP chest radiograph in a 57-year-old patient with COVID-19 infection shows diffuse bilateral mid and lower lung zone predominant peripheral opacities, which correspond to areas of acute lung injury and organizing pneumonia.
- 4. AP chest radiograph in a 65-year-old patient with COVID-19 infection shows patchy bilateral mid and lower lung zone opacities with a peripheral distribution, a common radiographic pattern in affected patients.
- 5. AP chest radiograph of a 40-year-old man with progressive dyspnea and hypoxemia requiring hospital admission shows mid and lower lung zone predominant peripheral heterogeneous pulmonary opacities.
- 6. AP chest radiograph of a 44-year-old patient with PCR-proven COVID-19 who developed acute respiratory distress syndrome (ARDS) shows bilateral heterogeneous opacities and a dense left basilar consolidation. ARDS is a known complication of Coronaviridae-associated pulmonary infections.
- 7. PA chest radiograph of 55-yr-old patient with mild dyspnea, low- grade fever shows subtle hazy opacities in right upper and left lower lung zones. These findings can be easily overlooked but were new when compared to an old chest radiograph (not shown).
- 8. AP chest radiograph of same patient 5 days later after PCR-proven COVID-19 shows extensive bilateral heterogeneous opacities in right upper and left mid to lower lung zones. Patient required intubation shortly thereafter due to severe dyspnea and hypoxemia.
- 9. PA chest radiograph of patient with Middle East respiratory syndrome (MERS) shows multifocal bilateral heterogeneous opacities and a right upper lobe coalescent heterogeneous consolidation. (Courtesy Kyung Soo Lee, MD.)
- 10. Axial CECT of the same patient shows right upper lobe ground-glass opacity on a background of septal thickening, the so-called crazy-paving CT pattern. (Courtesy Kyung Soo Lee, MD.)
- 11. Axial NECT of 77-yr-old man obtained 5 days after diagnosis of symptomatic COVID-19 shows subtle bilateral ill-defined peripheral ground-glass opacities. Two images published in The Lancet Infectious Diseases, Shi H et. al. Radiological Findings of 81 Patients with COVID-19. Copyright Elsevier (2020).
- 12. Axial NECT of same patient obtained 15 days after the initial onset of symptoms shows progression of bilateral pulmonary involvement manifesting with bilateral peripheral consolidations and ground-glass opacities.
- 13. AP chest radiograph of a patient with Middle East respiratory syndrome (MERS) obtained 10 days after presentation shows interval endotracheal intubation and disease progression with diffuse bilateral heterogeneous consolidations consistent with acute respiratory distress syndrome (ARDS). (Courtesy Kyung Soo Lee, MD.)
- 14. Axial NECT of a patient with Middle East respiratory syndrome (MERS) shows a left lower lobe peribronchovascular consolidation and surrounding centrilobular acinar ground-glass opacities. (Courtesy Kyung Soo Lee, MD.)
- 15. AP chest radiograph of a patient on chronic steroids for treatment of systemic lupus erythematosus who presented with pneumonia shows ill-defined left greater than right heterogeneous pulmonary opacities.
- 16. Axial NECT of the same patient shows left lung-predominant ill-defined ground-glass opacities and a small left pleural effusion. Coronavirus may cause upper and lower respiratory infections and may sporadically result in epidemics that tend to be associated with a high mortality.
- 17. AP chest radiograph of a patient with pulmonary hypertension, chronic atrial fibrillation, and community-acquired coronavirus pneumonia shows right basilar heterogeneous consolidation
- 18. Axial NECT of the same patient shows scattered bilateral peribronchovascular ground- glass and airspace opacities that predominantly affect the middle and right lower lobes. Coronavirus is a common etiology of viral upper respiratory infection but causes up to 3% of all community-acquired pneumonias.
- 19. Axial NECT of a patient with severe acute respiratory syndrome (SARS) shows multifocal bilateral left greater than right patchy ground- glass opacities and nodular consolidations. (Courtesy Yeun-Chung Chang, MD.)
- 20. Axial CECT of a patient with SARS shows a left lung peribronchovascular consolidation and ground-glass opacities. (Courtesy Yeun-Chung Chang, MD.)
- 21. AP chest radiograph of 58-yr-old patient with PCR-proven COVID- 19 who presented with cough, fever, chills shows ill-defined peripherally predominant opacities bilaterally. Ferritin level: 551 ng/ml and C-reactive protein: 193 mg/l.
- 22. Axial CECT of same patient shows peripheral, subpleural, well-demarcated ground-glass opacities interspaced with central areas of spared lung . Preliminary incidental pathologic reports have shown some features suggesting acute fibrinous organizing pneumonia (AFOP).
- 23. Coronal CECT of the same patient shows well- demarcated, peripheral, subpleural ground-glass opacities bilaterally, which are reminiscent of areas of organizing pneumonia.
- 24. AP chest radiograph of a 47-year-old patient with PCR-proven COVID-19 with history of gestational diabetes shows a right lower lobe mass.
- 25. Axial CECT of the same patient shows subpleural mass-like area of ground-glass opacities and denser peripheral opacities (i.e., reversed halo sign). Features of organizing pneumonia (possibly acute fibrinous organizing pneumonia, AFOP) have been described as early histologic changes in COVID-19 infection.