Download to read offline





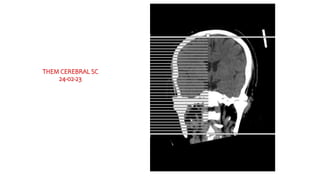





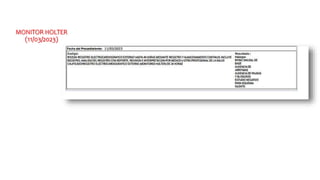







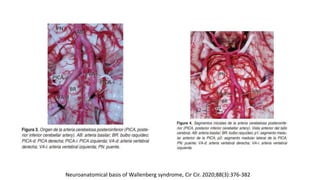
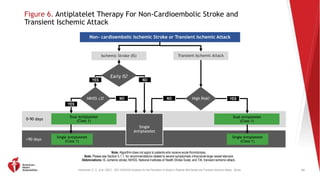
![Kleindorfer, D. O., et al. (2021). 2021 AHA/ASA Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack. Stroke.
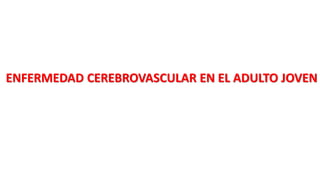
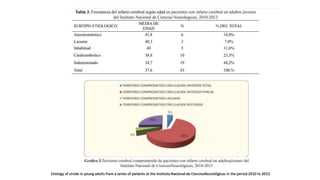
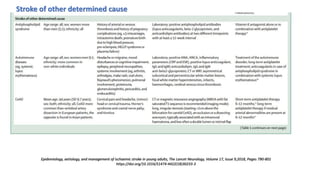
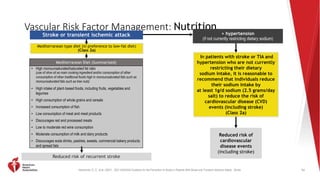
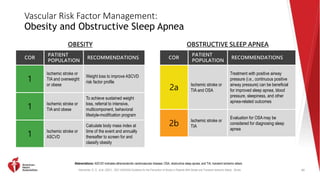
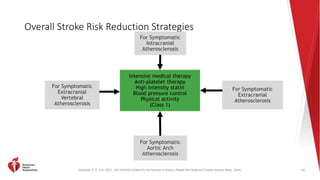
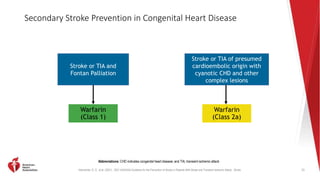
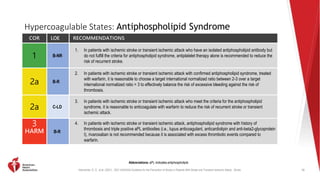
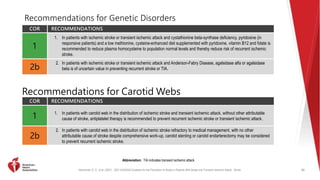
Figure 2. Algorithm for Evaluating Patients with Clinical Diagnosis of Stroke for
Optimizing Prevention of Recurrent Ischemic Stroke
53
Abbreviations: CT indicates computed tomography; CTA, computed tomography angiogram; ECG, electrocardiogram; MRA, magnetic resonance angiography; MRI, magnetic resonance imaging; SOE, source of embolism; TEE,
transesophageal echo; TIA; transient ischemic attack: and US, ultrasound. †When a patient has a transient neurological deficit clinically characteristic of transient ischemic attack, the patient should be evaluated in the same manner as a
patient who has an ischemic stroke with a corresponding cerebral infarct on imaging.
YES NO
Shows
ischemic
stroke†
Manage
accordingly
ECG and basic laboratory
tests*
(Class 1)
YES
NO
CT or MRI
shows ischemic
stroke mimic
Consider delayed
reimaging with CT or
MRI if not done initially
(Class 2a)
Manage accordingly
Anterior
circulation
infarct
Non-invasive
cervical carotid
imaging
[CTA, MRA, or US]
(Class 1)
Echocardiography
to evaluate for
cardiac SOE (Class
2a)
Non-invasive intracranial and
extracranial imaging of
vertebrobasilar arterial system
(Class 2a)
Cause
identified
Based on age,
medical
comorbidities
and clinical
syndrome,
consider:
Long-term cardiac rhythm monitoring (Class 2a)
Test for genetic stroke syndrome (Class 2a)
Test for infectious vasculitis (Class 2a)
TEE, Cardiac CT or Cardiac MRI (Class 2b)
Evaluate for other rare causes of stroke
CT or MRI (Class 1)
YES NO
YES
NO
Non-invasive
intracranial arterial
imaging (Class 2a)](https://image.slidesharecdn.com/casoclnicoevc-240205092652-0abba365/85/CASO-CLINICO-EVC-pptx-caso-clinico-medicina-interna-53-320.jpg)
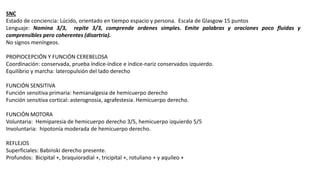
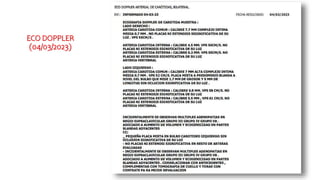
![Kleindorfer, D. O., et al. (2021). 2021 AHA/ASA Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack. Stroke.
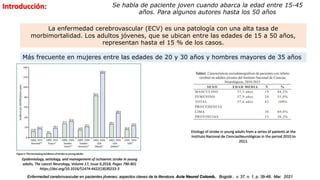
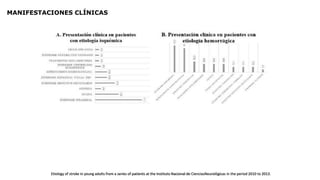
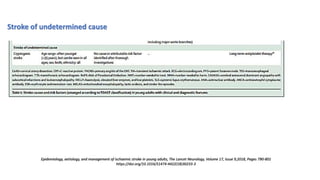
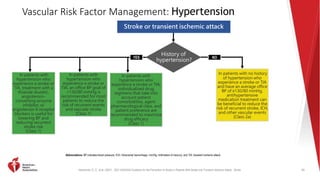
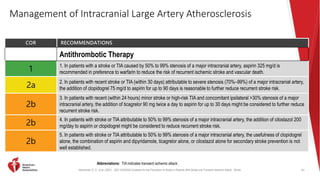
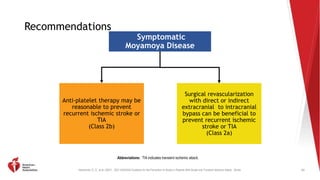
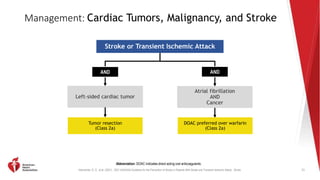
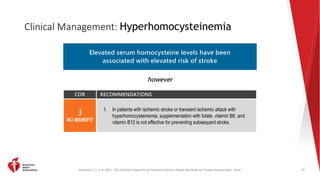
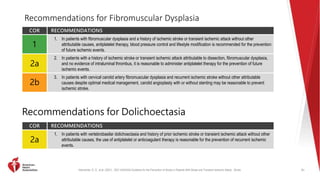
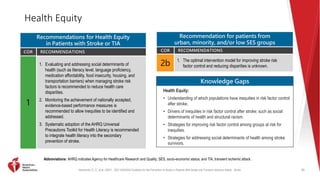
Vascular Risk Factor Management:
Hyperlipidemia and Hypertriglyceridemia
COR RECOMMENDATIONS
2a
In patients with ischemic stroke or TIA, with fasting triglycerides 135 to 499 mg/dL and LDL-C of 41 to 100
mg/dL, on moderate- or high-intensity statin therapy, with HbA1c <10%, and with no history of pancreatitis, AF, or
severe heart failure, treatment with icosapent ethyl (IPE) 2 g twice a day is reasonable to reduce risk of recurrent
stroke.
2a
In patients with severe hypertriglyceridemia (ie, fasting triglycerides ≥500 mg/dL [≥5.7 mmol/L]), it is reasonable
to identify and address causes of hypertriglyceridemia and, if triglycerides are persistently elevated or increasing,
to further reduce triglycerides in order to lower the risk of ASCVD events by implementation of a very low-fat diet,
avoidance of refined carbohydrates and alcohol, consumption of omega-3 fatty acids, and, if necessary to
prevent acute pancreatitis, fibrate therapy.
57
Abbreviations: AF indicates atrial fibrillation; ASCVD, atherosclerotic cardiovascular disease; HbA1c, glycated hemoglobin A1c; LDL-C, low-density lipoprotein cholesterol; and TIA, transient ischemic attack.
HYPERTRIGLYCERIDEMIA](https://image.slidesharecdn.com/casoclnicoevc-240205092652-0abba365/85/CASO-CLINICO-EVC-pptx-caso-clinico-medicina-interna-57-320.jpg)

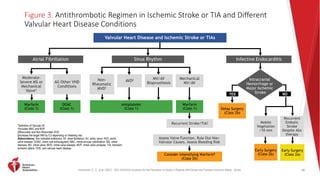

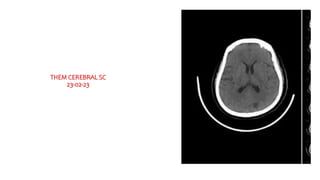
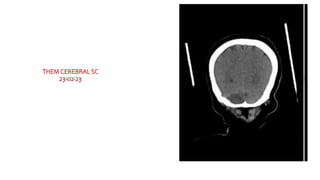
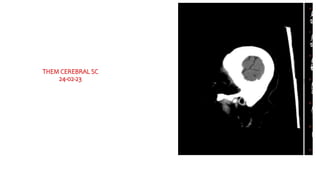
This document presents the case of a 50-year-old female patient who was admitted to the emergency room with right hemiparesis and sensory loss. She had recently undergone a hysterectomy and right salpingo-oophorectomy for myomas and an ovarian tumor. Neurological examination revealed right hemiplegia, sensory loss, and dysarthria consistent with a right cerebellar infarction. Laboratory tests and imaging studies including MRI were performed. She was diagnosed with a post-operative hypercoagulable state leading to a right cerebellar infarction. The patient was discussed with neurology and other services and treated medically.






























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
