WHAT IS APPENDIX?
The, appendix is a small tube like structure attached to the large
intestine (colon).
It is a vestigial organ.
Location-attached to the caecum(starting part of the large intestine).
Size- about 5-10cm long (2-4 inches).
WHAT IS APPENDICITIS?
It is the inflammation of the appendix.
WHAT IS APPENDECTOMY?
It is the surgical procedure to remove the appendix.
3.
DEMOGRAPHICS DATA:-
NAME-Sameer Shah
AGE- 18Yr.
GENDER- male.
ADDRESS- Nawab ni chali near welcome bakery , shah e aalam
OCCUPATION- Student(11th
)
SOCIOECONOMIC CONDITION-Lower middle class (according to kuuppuswamy scale).
DATE OF ADDMISION- 30/12/25
DATE OF SURGERY- 7/1/26
DATE OF EVALUATION- (pre op) - 5/1/26 , (post op) - 8/1/26
REFFERED BY- Self
HANDEDNESS- Right
4.
CHIEF COMPLAIN:-
PRE OPCOMPLAIN:-
Pain in right lower abdomen(rt
iliac fossa).
Pain while doing all ADL &
sleep.
Episodes of vomiting after
eating.
POST OP COMPLAIN:-
Pain over surgical area.
5.
PRESENT HISTORY:-
On 30th
December2025 around 10:00AM ,the 18yr old male child,
came to LG hospital with complain of epigastric region pain
which was insidious in onset & gradually increased in intensity ,
and also had complain of 7-8 episodes of vomiting 1 day prior
before admitting. After that doctor examined and advised them
to go for ultrasonography and blood report which reveals that
patient has grade 1 fatty liver, gall bladder is partially distended.
After that medications were started .on 2nd
January 2026 MDCT
SCAN OF ABDOMIN AND PELVIS was done which reveals that
there is 11mm dilation fluid filled inflammation in appendix , liver
& spleen appears enlarged. So After this reports doctor
suggested them to go for Laparoscopic appendectomy.
6.
PAST HISTORY:-
Before3 months ago the patient has episode of pain in right iliac fossa(appendix
pain).
SURGICAL HISTORY:-
On 6th
of January 2026 from mid12:00am patient was nil by mouth then ,On 7th
of
January 2026 morning 10:30am the patient was taken to OT for removal of
appendix (laparoscopic appendectomy) was done & Inj metro was given& general
anesthesia was given(Inj propofol 130mg IV).
PERSONAL HISTORY:-
Diet – mixed.
Sleep – adequate.
Appetite –was normal.
He is occasional ciggarate smoker.
7.
DRUG HISTORY:-
PRE OP:-
Inj zostum 1.5gm IV (12hrly)
(antibiotics)
Inj mika 500 IV(12hrly)(antibiotics)
Inj metro 10 IV (5hrly)(antibiotics)
Tab diclo 1-0-1 (painkiller)
Cap omez 1-0-1(antacid)
POST OP:-
Inj ceftriaxone 1gm IV (12hrly)
(antibiotics)
Inj metro 10 IV (8hrly)(antibiotics)
Inj dynapar 1A IV (8hrly)(painkiller)
Cap omez (20) 1-0-1 (antaacid)
8.
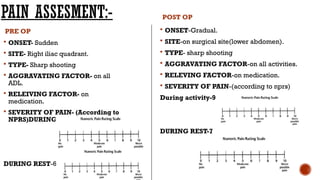
PAIN ASSESMENT:-
PRE OP
ONSET- Sudden
SITE- Right iliac quadrant.
TYPE- Sharp shooting
AGGRAVATING FACTOR- on all
ADL.
RELEIVING FACTOR- on
medication.
SEVERITY OF PAIN- (According to
NPRS)DURING ACTIVITY- 9
DURING REST-6
POST OP
ONSET-Gradual.
SITE-on surgical site(lower abdomen).
TYPE- sharp shooting
AGGRAVATING FACTOR-on all activities.
RELEVING FACTOR-on medication.
SEVERITY OF PAIN-(according to nprs)
During activity-9
DURING REST-7
9.
VITALS SIGNS:-(pre op)
TEMPRATURE-98.6f.
PULSE RATE-76 beats/min.
RESPIRATORY RATE-16 breaths/min.
BLOOD PRESSURE-110/78 mm hg.
SPO2-98%.
(POST OP)-
TEMPRATUR-98.6 F.
PULDE RATE-104 beats/min.
RESPIRATORY RATE-16 breaths/min.
BLOOD PRESSURE-124/86 mm hg.
SPO2-98%.
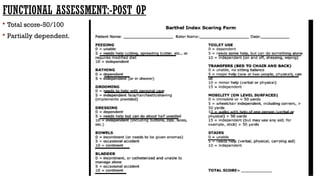
10.
ON OBSERVATION:-
LEVEL OFCONSCIOUSNESS- (according to GCS)-(pre
op)15/15 conscious ,oriented.
(post op) 15/15 conscious & oriented.
BODY BUILT-ectomorph.
MODE OF AMBULATION-(pre op) Independent,(post
op)-dependent.
ATTITUDE OF LIMB- normal.
11.
SWELLING-(pre op)overlower right side of abdomen (right iliac fossa).
SCAR(post op)- lower abdomen ,laparoscopic method
EXTERNAL APPLIANCE-(pre op)iv cannula drip(rt side back of forearm).
(post op) iv cannula drip(Lt side back of forearm).
TROPHICAL CHANGES-not present.
BREATHING PATTERN-Abdomino-thoracic
12.
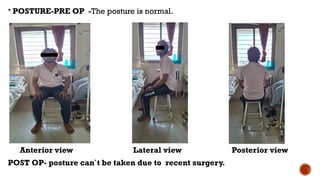
POSTURE-PRE OP-The posture is normal.
Anterior view Lateral view Posterior view
POST OP- posture can`t be taken due to recent surgery.
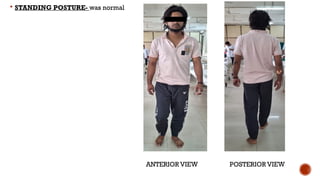
oGAIT-(PRE OP)
gaitis normal
All the phases of gait are present.
Arm swing is also normal.
Cadence,step length,stride length all are
normal.
POST OP-
Can`t be taken due to recent surgery.
15.
ON PALPATION:-
TEMPRATURE(local)-normal.
TENDERNESS-(PRE OP)-Grade 2(pt complains of pain and winces).
(POST OP)-Grade4(pt will not allow to palpate the area).
SCAR(post op)- adherence : not tested due to underbandage.
on examination:-
GCS-(pre op)-conscious&oriented15/15.(post op)-conscious&oriented15/15
SCAR – Length- 0.5-1.5cm , non infected.
SENSORY EXAMINATION- intact.(both pre op& post op).
BOWEL & BLADDER-(pre op)-normal.
(post op)-normal.
CHEST EXPANSION-normal
16.
AUSCULTATION-bowel &heart sounds were normal & heard.
REFLEXES-(pre op)all the abdominal reflexes were normal.
(post op) due to pain cant be taken.
ROM-
MMT-
Lumbar flexion AROM PROM
PRE OP 0-50 0-55
POST OP cant be taken due to Recent surgery
ABDOMINAL S PRE OP POST OP
RECTUS ABDOMINIS 4 Cant be taken due to
OBLIQUES(INT&EXT) 4 Recent surgery
TRANSVERSE
ABDOMINIS
4
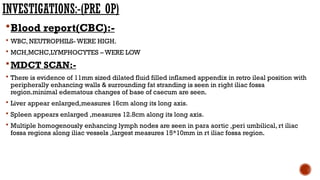
INVESTIGATIONS:-(PRE OP)
Blood report(CBC):-
WBC, NEUTROPHILS- WERE HIGH.
MCH,MCHC,LYMPHOCYTES – WERE LOW
MDCT SCAN:-
There is evidence of 11mm sized dilated fluid filled inflamed appendix in retro ileal position with
peripherally enhancing walls & surrounding fat stranding is seen in right iliac fossa
region.minimal edematous changes of base of caecum are seen.
Liver appear enlarged,measures 16cm along its long axis.
Spleen appears enlarged ,measures 12.8cm along its long axis.
Multiple homogenously enhancing lymph nodes are seen in para aortic ,peri umbilical, rt iliac
fossa regions along iliac vessels ,largest measures 15*10mm in rt iliac fossa region.
20.
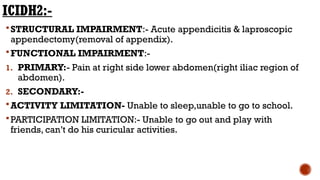
ICIDH2:-
STRUCTURAL IMPAIRMENT:- Acuteappendicitis & laproscopic
appendectomy(removal of appendix).
FUNCTIONAL IMPAIRMENT:-
1. PRIMARY:- Pain at right side lower abdomen(right iliac region of
abdomen).
2. SECONDARY:-
ACTIVITY LIMITATION- Unable to sleep,unable to go to school.
PARTICIPATION LIMITATION:- Unable to go out and play with
friends, can’t do his curicular activities.
21.
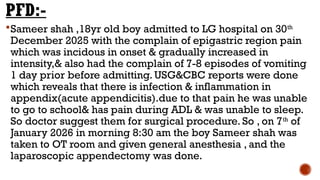
PFD:-
Sameer shah ,18yrold boy admitted to LG hospital on 30th
December 2025 with the complain of epigastric region pain
which was incidous in onset & gradually increased in
intensity,& also had the complain of 7-8 episodes of vomiting
1 day prior before admitting. USG&CBC reports were done
which reveals that there is infection & inflammation in
appendix(acute appendicitis).due to that pain he was unable
to go to school& has pain during ADL & was unable to sleep.
So doctor suggest them for surgical procedure. So , on 7th
of
January 2026 in morning 8:30 am the boy Sameer shah was
taken to OT room and given general anesthesia , and the
laparoscopic appendectomy was done.
22.
CLINICAL CONCLUSION:-
From allthe blood reports and MDCT scan they concluded
that, the patient was having acute appendicitis , grade 1 fatty
liver , partially distended gall bladder,11mm dilation fluid
filled inflammation in appendix , liver & spleen appears
enlarged& WBC & neutrophils and are high in amount ,MCH
& MCHC & LYMPHOCYTES are less in amount.
So from all this we need to remove the appendix
(laparoscopic appendectomy was done).
23.
PROBLEM LIST:-
Patient haspain in right iliac region of abdomen.
He is unable to sleep at night.
Can’t go to school due to severe pain.
Due to pain can’t eat properly & has episode’s of vomiting after
eating.
3. CIRCULATORY EXERCISE:-
Purpose-prevent venous stasis & reduce the risk of DVT.
Ankle pumps.
Toe pumps.
Gentle active movements of ul & LL .
5-6 times/day & 10*3 repetition.
4. PATIENTS EDUCATION:-
Explaination of surgery and post op care.
Teach- deep breathing exercise.
Supported coughing(splinting with pillow).
Importance of early mobilization post surgery.

































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

