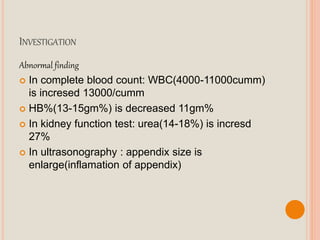
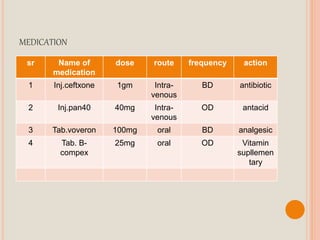
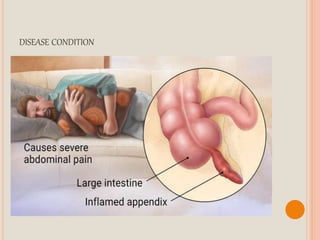
This document presents a case study of a 35-year-old male farmer, Mr. Namdev J. Kokate, who was admitted to the hospital with a chief complaint of abdominal pain, nausea, and vomiting for the past 5 days. Upon examination and testing, he was diagnosed with acute appendicitis. His history, physical exam findings, lab results, and ultrasound results are documented. He received IV antibiotics and analgesics for treatment and underwent an appendectomy surgery. The case presentation covers his medical history, physical assessment, diagnostic workup, treatment plan, and nursing care.
























![Case presentation on_dengue_fever[1]](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationondenguefever1-200706144354-thumbnail.jpg?width=640&height=640&fit=bounds)

















































