Report
Share

Recommended
Carotid endarterectomy
Carotid artery disease is commonly seen in association with atherosclerosis and complicate the situation. clearcut guidelines with necessary surgical details are provided in presentations.
Anesthesia for-carotid-endarterectomy
The document discusses carotid endarterectomy (CEA) including:
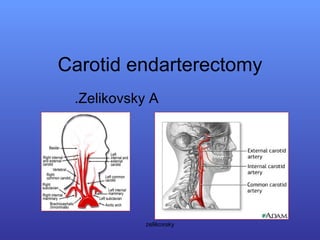
- Anatomy of carotid arteries and cerebral blood supply
- Risk factors for and clinical presentations of carotid artery disease
- Evaluation and treatment options including CEA and angioplasty/stenting
- Perioperative considerations for CEA including hemodynamic management, anesthesia techniques, neurologic monitoring, and goals of maintaining cerebral perfusion and blood pressure stability.
Postop carotid endarterectomy
The document provides guidelines for postoperative care after carotid endarterectomy, noting that patients should be closely monitored for complications like hypertension, hypotension, hematoma, and cardiac issues in the first 48 hours after surgery. It also discusses potential complications like hyperperfusion syndrome, intracerebral hemorrhage, and seizures that require strict blood pressure control. The guidelines emphasize vigilant monitoring and management of hemodynamics and neurological symptoms in the postoperative period to optimize outcomes and prevent complications.
Estenose c
Carotid vascular disease is a leading cause of stroke in the US. Treatment options include carotid endarterectomy (CEA) surgery and nonsurgical carotid revascularization using angioplasty and stenting. Studies have shown conflicting results comparing the two approaches. CEA is generally recommended but angioplasty and stenting may be better for high-risk surgical patients or those with significant comorbidities. More research is still needed to refine treatment recommendations.
Current indications & therapies for Carotid Artery Stenosis
Brought to you from the caring and expert staff of the beautiful modern Vascular Center at Sisters' of Charity Hospital of Buffalo, 2157 Main Street Buffalo, New York 14214 USA
Anesthesia for Carotid Endarterectomy: Risks, Benefits, Alternatives
Anesthesia for Carotid Endarterectomy: Risks, Benefits, AlternativesNC Association of Nurse Anesthetists
This document summarizes key points about carotid endarterectomy and anesthesia considerations for the procedure. It discusses risks of carotid artery disease and benefits of carotid endarterectomy in reducing stroke risk. It reviews advantages and disadvantages of local, regional, and general anesthesia. It also outlines important perioperative management considerations like maintaining cerebral perfusion and minimizing hemodynamic fluctuations. Monitoring techniques and advances in agents are reviewed to aid neuroprotection during the surgery. Complications are also summarized.350 Carotid endarterectomy
This document describes the technique for carotid endarterectomy. It discusses preoperative evaluation and indications based on randomized controlled trials showing benefit for recently symptomatic stenosis of 70-99% or 50-69% if risk is low. Asymptomatic patients may benefit from surgery for >60% stenosis if risk is <3%. The technique involves exposure of the carotid bifurcation, endarterectomy to remove plaque, possible shunt placement, closure of the arteriotomy with patch or sutures, and postoperative care including blood pressure management to prevent complications.
Guidelines in the management of carotid stenosis
This document provides an overview of guidelines for the management of carotid stenosis. It discusses:
1) Stroke is a major cause of death, with many caused by carotid artery disease. The risk of stroke is directly related to the degree of stenosis.
2) Natural history studies show that the risk of stroke is highest in the first year after symptoms and then declines over time. The risk is higher for more severe stenosis.
3) Early trials demonstrated the benefits of carotid endarterectomy (CEA) in reducing stroke risks compared to medical management alone for symptomatic and some asymptomatic patients.
4) Later trials evaluated carotid angioplasty and stenting (CAS) as an alternative to CEA but
Recommended
Carotid endarterectomy
Carotid artery disease is commonly seen in association with atherosclerosis and complicate the situation. clearcut guidelines with necessary surgical details are provided in presentations.
Anesthesia for-carotid-endarterectomy
The document discusses carotid endarterectomy (CEA) including:
- Anatomy of carotid arteries and cerebral blood supply
- Risk factors for and clinical presentations of carotid artery disease
- Evaluation and treatment options including CEA and angioplasty/stenting
- Perioperative considerations for CEA including hemodynamic management, anesthesia techniques, neurologic monitoring, and goals of maintaining cerebral perfusion and blood pressure stability.
Postop carotid endarterectomy
The document provides guidelines for postoperative care after carotid endarterectomy, noting that patients should be closely monitored for complications like hypertension, hypotension, hematoma, and cardiac issues in the first 48 hours after surgery. It also discusses potential complications like hyperperfusion syndrome, intracerebral hemorrhage, and seizures that require strict blood pressure control. The guidelines emphasize vigilant monitoring and management of hemodynamics and neurological symptoms in the postoperative period to optimize outcomes and prevent complications.
Estenose c
Carotid vascular disease is a leading cause of stroke in the US. Treatment options include carotid endarterectomy (CEA) surgery and nonsurgical carotid revascularization using angioplasty and stenting. Studies have shown conflicting results comparing the two approaches. CEA is generally recommended but angioplasty and stenting may be better for high-risk surgical patients or those with significant comorbidities. More research is still needed to refine treatment recommendations.
Current indications & therapies for Carotid Artery Stenosis
Brought to you from the caring and expert staff of the beautiful modern Vascular Center at Sisters' of Charity Hospital of Buffalo, 2157 Main Street Buffalo, New York 14214 USA
Anesthesia for Carotid Endarterectomy: Risks, Benefits, Alternatives
Anesthesia for Carotid Endarterectomy: Risks, Benefits, AlternativesNC Association of Nurse Anesthetists
This document summarizes key points about carotid endarterectomy and anesthesia considerations for the procedure. It discusses risks of carotid artery disease and benefits of carotid endarterectomy in reducing stroke risk. It reviews advantages and disadvantages of local, regional, and general anesthesia. It also outlines important perioperative management considerations like maintaining cerebral perfusion and minimizing hemodynamic fluctuations. Monitoring techniques and advances in agents are reviewed to aid neuroprotection during the surgery. Complications are also summarized.350 Carotid endarterectomy
This document describes the technique for carotid endarterectomy. It discusses preoperative evaluation and indications based on randomized controlled trials showing benefit for recently symptomatic stenosis of 70-99% or 50-69% if risk is low. Asymptomatic patients may benefit from surgery for >60% stenosis if risk is <3%. The technique involves exposure of the carotid bifurcation, endarterectomy to remove plaque, possible shunt placement, closure of the arteriotomy with patch or sutures, and postoperative care including blood pressure management to prevent complications.
Guidelines in the management of carotid stenosis
This document provides an overview of guidelines for the management of carotid stenosis. It discusses:
1) Stroke is a major cause of death, with many caused by carotid artery disease. The risk of stroke is directly related to the degree of stenosis.
2) Natural history studies show that the risk of stroke is highest in the first year after symptoms and then declines over time. The risk is higher for more severe stenosis.
3) Early trials demonstrated the benefits of carotid endarterectomy (CEA) in reducing stroke risks compared to medical management alone for symptomatic and some asymptomatic patients.
4) Later trials evaluated carotid angioplasty and stenting (CAS) as an alternative to CEA but
AORTO-ILIAC INTERVENTIONS
This document summarizes techniques for endovascular treatment of aorto-iliac occlusive disease. It discusses:
1) Technical success rates are high but complications can occur, especially with chronic total occlusions. Primary stenting is preferred over PTA with provisional stenting for long lesions.
2) Patency rates at 5-10 years range from 46-96% depending on the location and type of lesion. Risk factors for restenosis include occlusion length and poor runoff.
3) Endovascular treatment has advantages over open surgery like shorter hospital stays and lower complications/mortality, though open bypass has higher long term patency. Drug-eluting devices may help address issues of rest
Iom during carotid endarterectomy 2008
Intraoperative monitoring during carotid endarterectomy provides critical information to surgeons. EEG and SEP modalities are highly sensitive to hemodynamic disturbances and embolism during CEA. EEG monitors cortical activity while SEP detects subcortical ischemia. Multimodal monitoring with EEG and SEP is most effective. Changes in the modalities can indicate mild, moderate or severe ischemia. Close communication between monitoring, surgery and anesthesia teams is important for optimal results during CEA.
Carotid Endarterectomy in Stroke Prevention Update
This document discusses carotid endarterectomy for stroke prevention. It provides background on strokes, defines different types of strokes, and outlines diagnostic techniques. The bulk of the document focuses on carotid endarterectomy, describing what it is, the history of the procedure, how it is performed, and results from major clinical trials demonstrating its effectiveness in reducing stroke risk compared to medical management alone for patients with significant carotid artery stenosis. The document emphasizes awareness of new techniques and treatments to prevent strokes.
Coarctation of aorta
This document discusses coarctation of the aorta, including:
1. The definition and history of coarctation as a congenital narrowing of the upper descending thoracic aorta.
2. Theories on the pathogenesis of coarctation related to reduced blood flow through the left side of the heart or abnormal ductal tissue.
3. Types of coarctation including preductal and postductal, and surgical techniques for repair such as patch aortoplasty or bypass grafting.
4. Presentation varies from heart failure in neonates to hypertension in older children and adults, with complications including aneurysm and rupture.
a rough guide to abdominal aortic aneurysms
The abdominal aorta is the section of the aorta located in the abdomen. Abdominal aortic aneurysms (AAAs) occur when this section of the aorta abnormally enlarges due to weakening of the aortic wall. AAAs are usually asymptomatic until rupture, which can cause life-threatening internal bleeding. Ultrasound screening for men over 65 can detect AAAs and help prevent ruptures. Treatment options for AAAs include open surgical repair and endovascular aneurysm repair (EVAR) via catheter deployment of a stent graft. While EVAR has lower risks, open repair may provide longer-term durability in some cases.
Anesthesia for Lower limb revascularization
This document discusses anaesthesia considerations for lower limb revascularization procedures. It begins with an introduction to peripheral artery disease and classifications. Causes, common sites, and presentations of acute and chronic limb ischemia are described. Preoperative assessment includes cardiovascular and pulmonary evaluation. Risk stratification guidelines are provided. Optimal perioperative management focuses on hemodynamic stability, temperature control, hydration and pain management. Both regional and general anesthesia techniques are reviewed. Postoperative monitoring and analgesia are also discussed.
CAROTID ARTERY STENOSIS
Carotid artery stenosis refers to atherosclerotic narrowing of the carotid arteries. While a correlation between stenosis level and stroke risk is expected, the relationship is unclear. Carotid artery stenosis is variably defined as 60-99% or 50-99% narrowing. Screening for carotid artery stenosis can be done with neck auscultation or ultrasound, but both have limitations in sensitivity and specificity compared to angiography. Noninvasive imaging techniques like ultrasound and MRI are better options for screening and diagnosis of carotid artery stenosis.
Presentation1.pptx, radiological vascular anatomy of the upper and lower limbs.
The document describes the arterial and venous anatomy of the upper and lower limbs. It begins by outlining the arterial supply to the upper limb, starting from the subclavian artery and its branches. It then discusses the arteries of the forearm, hand, and veins of the upper limb. For the lower limb, it discusses the femoral artery and its branches that supply the thigh as well as the arteries of the leg. It includes diagrams to illustrate the key structures and their relationships. CT, MR, and conventional angiography images are also provided to demonstrate the vascular anatomy.
A technical modification of carotid endarterectomy experience with 400 pati...
This document discusses techniques for carotid endarterectomy based on the experience of 400 patients. It finds that eversion carotid endarterectomy had a lower restenosis rate of 1.7% compared to 9.3% for primary closure and 6.5% for patch angioplasty. Additionally, eversion carotid endarterectomy had a faster mean operative time of 31 minutes compared to 39 minutes for primary closure and 46 minutes for patch angioplasty. Finally, a study of over 1,900 carotid endarterectomies found primary closure was associated with significantly higher risks of perioperative stroke at 5.6% and stroke or death at 6.0% compared to 2.2-2.5% for
Angiography and Angioplasty
This document discusses angiography and angioplasty procedures. It explains that angiography uses imaging techniques to visualize blood vessels, while angioplasty widens narrowed vessels. The document outlines different types of each procedure and describes how they are performed. It also discusses stents, which are used to prop open vessels after angioplasty and discusses advantages and disadvantages of various stent materials.
Nursing Care of Clients with Peripheral Vascular Disorders Part 2 of 3
Nursing Care of Clients with Peripheral Vascular Disorders Part 2 of 3: Arterial disorders such as Arterial occlusive disease, Arterial embolism, Arterial thrombosis, Thromboangiitis obliterans (Buerger’s disease), Aortitis, Aortoiliac disease, Aneurysms, Raynaud’s disease, and Thoracic outlet syndrome
Anatomy and intervention in cerebral vasculature
1. The cerebral vasculature includes the internal carotid and vertebral arteries which supply blood to the brain. Venous drainage occurs through dural sinuses and cerebral veins.
2. The Circle of Willis is a major vascular structure that connects the arteries of the brain. It includes components like the anterior and posterior cerebral arteries.
3. Imaging techniques used to evaluate the cerebral vasculature include conventional angiography, CT angiography, MR angiography, ultrasound and digital subtraction angiography. Each has advantages and disadvantages for assessing the anatomy and identifying abnormalities.
Abdominal Aortic Aneurysm
This document discusses abdominal aortic aneurysms (AAAs). It notes that Albert Einstein died from an AAA, which affects over 700,000 people in Europe. AAAs are a silent killer as they often show no symptoms. The main risk factors are being male, smoking history, hypertension, family history, and increasing age. Ultrasound is an effective way to diagnose AAAs. If left untreated, AAAs over 5cm have a high risk of rupture. Small AAAs under 4cm should be monitored annually, while larger AAAs may require surgical or endovascular treatment.
Abdominal Aortic Aneurysms
This document discusses a case of a 52-year-old male presenting for elective repair of a large abdominal aortic aneurysm (AAA). It provides background on AAAs including risk factors, pathophysiology, epidemiology, presentation, natural history, and treatment options including surveillance and surgical repair. Treatment focuses on risk factor modification, antibiotics, analgesia, DVT prophylaxis, and management of postoperative complications. The patient underwent successful AAA repair with bifemoral bypass and subsequently recovered from postoperative pneumonia and arrhythmia.
Carotid artery disease
I am a Neurosurgeon with advanced training in Interventional vascular Neurosurgery(FINR) from Zurich, Switzerland, and FMINS-Fellowship in minimally invasive and Endoscopic Neurosurgery from Germany.
I am presently working in Columbia asia hospitals, Bangalore.
My areas of interest are Vascular Neurosurgery, Stroke specialist, interventional neuroradiology, Endoscopic and minimally invasive Neurosurgery, Endoscopic spine surgery.
More Related Content
Viewers also liked
AORTO-ILIAC INTERVENTIONS
This document summarizes techniques for endovascular treatment of aorto-iliac occlusive disease. It discusses:
1) Technical success rates are high but complications can occur, especially with chronic total occlusions. Primary stenting is preferred over PTA with provisional stenting for long lesions.
2) Patency rates at 5-10 years range from 46-96% depending on the location and type of lesion. Risk factors for restenosis include occlusion length and poor runoff.
3) Endovascular treatment has advantages over open surgery like shorter hospital stays and lower complications/mortality, though open bypass has higher long term patency. Drug-eluting devices may help address issues of rest
Iom during carotid endarterectomy 2008
Intraoperative monitoring during carotid endarterectomy provides critical information to surgeons. EEG and SEP modalities are highly sensitive to hemodynamic disturbances and embolism during CEA. EEG monitors cortical activity while SEP detects subcortical ischemia. Multimodal monitoring with EEG and SEP is most effective. Changes in the modalities can indicate mild, moderate or severe ischemia. Close communication between monitoring, surgery and anesthesia teams is important for optimal results during CEA.
Carotid Endarterectomy in Stroke Prevention Update
This document discusses carotid endarterectomy for stroke prevention. It provides background on strokes, defines different types of strokes, and outlines diagnostic techniques. The bulk of the document focuses on carotid endarterectomy, describing what it is, the history of the procedure, how it is performed, and results from major clinical trials demonstrating its effectiveness in reducing stroke risk compared to medical management alone for patients with significant carotid artery stenosis. The document emphasizes awareness of new techniques and treatments to prevent strokes.
Coarctation of aorta
This document discusses coarctation of the aorta, including:
1. The definition and history of coarctation as a congenital narrowing of the upper descending thoracic aorta.
2. Theories on the pathogenesis of coarctation related to reduced blood flow through the left side of the heart or abnormal ductal tissue.
3. Types of coarctation including preductal and postductal, and surgical techniques for repair such as patch aortoplasty or bypass grafting.
4. Presentation varies from heart failure in neonates to hypertension in older children and adults, with complications including aneurysm and rupture.
a rough guide to abdominal aortic aneurysms
The abdominal aorta is the section of the aorta located in the abdomen. Abdominal aortic aneurysms (AAAs) occur when this section of the aorta abnormally enlarges due to weakening of the aortic wall. AAAs are usually asymptomatic until rupture, which can cause life-threatening internal bleeding. Ultrasound screening for men over 65 can detect AAAs and help prevent ruptures. Treatment options for AAAs include open surgical repair and endovascular aneurysm repair (EVAR) via catheter deployment of a stent graft. While EVAR has lower risks, open repair may provide longer-term durability in some cases.
Anesthesia for Lower limb revascularization
This document discusses anaesthesia considerations for lower limb revascularization procedures. It begins with an introduction to peripheral artery disease and classifications. Causes, common sites, and presentations of acute and chronic limb ischemia are described. Preoperative assessment includes cardiovascular and pulmonary evaluation. Risk stratification guidelines are provided. Optimal perioperative management focuses on hemodynamic stability, temperature control, hydration and pain management. Both regional and general anesthesia techniques are reviewed. Postoperative monitoring and analgesia are also discussed.
CAROTID ARTERY STENOSIS
Carotid artery stenosis refers to atherosclerotic narrowing of the carotid arteries. While a correlation between stenosis level and stroke risk is expected, the relationship is unclear. Carotid artery stenosis is variably defined as 60-99% or 50-99% narrowing. Screening for carotid artery stenosis can be done with neck auscultation or ultrasound, but both have limitations in sensitivity and specificity compared to angiography. Noninvasive imaging techniques like ultrasound and MRI are better options for screening and diagnosis of carotid artery stenosis.
Presentation1.pptx, radiological vascular anatomy of the upper and lower limbs.
The document describes the arterial and venous anatomy of the upper and lower limbs. It begins by outlining the arterial supply to the upper limb, starting from the subclavian artery and its branches. It then discusses the arteries of the forearm, hand, and veins of the upper limb. For the lower limb, it discusses the femoral artery and its branches that supply the thigh as well as the arteries of the leg. It includes diagrams to illustrate the key structures and their relationships. CT, MR, and conventional angiography images are also provided to demonstrate the vascular anatomy.
A technical modification of carotid endarterectomy experience with 400 pati...
This document discusses techniques for carotid endarterectomy based on the experience of 400 patients. It finds that eversion carotid endarterectomy had a lower restenosis rate of 1.7% compared to 9.3% for primary closure and 6.5% for patch angioplasty. Additionally, eversion carotid endarterectomy had a faster mean operative time of 31 minutes compared to 39 minutes for primary closure and 46 minutes for patch angioplasty. Finally, a study of over 1,900 carotid endarterectomies found primary closure was associated with significantly higher risks of perioperative stroke at 5.6% and stroke or death at 6.0% compared to 2.2-2.5% for
Angiography and Angioplasty
This document discusses angiography and angioplasty procedures. It explains that angiography uses imaging techniques to visualize blood vessels, while angioplasty widens narrowed vessels. The document outlines different types of each procedure and describes how they are performed. It also discusses stents, which are used to prop open vessels after angioplasty and discusses advantages and disadvantages of various stent materials.
Nursing Care of Clients with Peripheral Vascular Disorders Part 2 of 3
Nursing Care of Clients with Peripheral Vascular Disorders Part 2 of 3: Arterial disorders such as Arterial occlusive disease, Arterial embolism, Arterial thrombosis, Thromboangiitis obliterans (Buerger’s disease), Aortitis, Aortoiliac disease, Aneurysms, Raynaud’s disease, and Thoracic outlet syndrome
Anatomy and intervention in cerebral vasculature
1. The cerebral vasculature includes the internal carotid and vertebral arteries which supply blood to the brain. Venous drainage occurs through dural sinuses and cerebral veins.
2. The Circle of Willis is a major vascular structure that connects the arteries of the brain. It includes components like the anterior and posterior cerebral arteries.
3. Imaging techniques used to evaluate the cerebral vasculature include conventional angiography, CT angiography, MR angiography, ultrasound and digital subtraction angiography. Each has advantages and disadvantages for assessing the anatomy and identifying abnormalities.
Abdominal Aortic Aneurysm
This document discusses abdominal aortic aneurysms (AAAs). It notes that Albert Einstein died from an AAA, which affects over 700,000 people in Europe. AAAs are a silent killer as they often show no symptoms. The main risk factors are being male, smoking history, hypertension, family history, and increasing age. Ultrasound is an effective way to diagnose AAAs. If left untreated, AAAs over 5cm have a high risk of rupture. Small AAAs under 4cm should be monitored annually, while larger AAAs may require surgical or endovascular treatment.
Abdominal Aortic Aneurysms
This document discusses a case of a 52-year-old male presenting for elective repair of a large abdominal aortic aneurysm (AAA). It provides background on AAAs including risk factors, pathophysiology, epidemiology, presentation, natural history, and treatment options including surveillance and surgical repair. Treatment focuses on risk factor modification, antibiotics, analgesia, DVT prophylaxis, and management of postoperative complications. The patient underwent successful AAA repair with bifemoral bypass and subsequently recovered from postoperative pneumonia and arrhythmia.
Carotid artery disease
I am a Neurosurgeon with advanced training in Interventional vascular Neurosurgery(FINR) from Zurich, Switzerland, and FMINS-Fellowship in minimally invasive and Endoscopic Neurosurgery from Germany.
I am presently working in Columbia asia hospitals, Bangalore.
My areas of interest are Vascular Neurosurgery, Stroke specialist, interventional neuroradiology, Endoscopic and minimally invasive Neurosurgery, Endoscopic spine surgery.
Viewers also liked (16)
Carotid Endarterectomy in Stroke Prevention Update
Carotid Endarterectomy in Stroke Prevention Update
Presentation1.pptx, radiological vascular anatomy of the upper and lower limbs.
Presentation1.pptx, radiological vascular anatomy of the upper and lower limbs.
A technical modification of carotid endarterectomy experience with 400 pati...
A technical modification of carotid endarterectomy experience with 400 pati...
Nursing Care of Clients with Peripheral Vascular Disorders Part 2 of 3
Nursing Care of Clients with Peripheral Vascular Disorders Part 2 of 3
Carotid Endarterectomy
- 1. Carotid endarterectomy Zelikovsky A. zelikovsky
- 10. CT zelikovsky
- 14. zelikovsky
- 15. CEA zelikovsky
- 16. CEA + SHUNT zelikovsky
- 17. PTA + STENT zelikovsky
- 18. zelikovsky