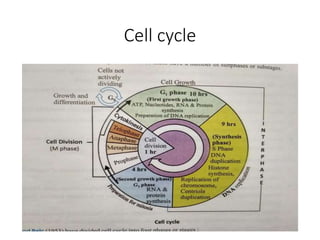
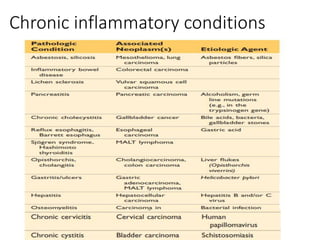
This document provides an overview of cancer biology. It discusses the history of cancer discovery, epidemiology, carcinogenesis and the hallmarks of cancer. It describes the cell cycle, apoptosis, cancer genes and genetic lesions. Enabling factors of cancer like genomic instability and tumor-promoting inflammation are explained. The clinical presentation, screening, prevention and management of cancer are also summarized. Key topics covered include the cell cycle, tumor suppressor genes, oncogenes, angiogenesis, invasion and metastasis, and evasion of immune surveillance. Grading and staging of cancer as well as laboratory diagnosis are also outlined.