1. Antenatal Care
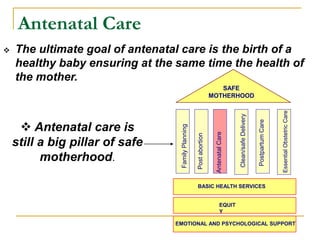
The ultimate goal of antenatal care is the birth of a
healthy baby ensuring at the same time the health of
the mother.
.
Post
abortion
Postpartum
Care
Family
Planning
Antenatal
Care
Clean/safe
Delivery
Essential
Obstetric
Care
BASIC HEALTH SERVICES
EMOTIONAL AND PSYCHOLOGICAL SUPPORT
EQUIT
Y
SAFE
MOTHERHOOD
Antenatal care is
still a big pillar of safe
motherhood.
3. Objectives of ANC …….
To promote, protect and maintain the health of the mother
during pregnancy.
To detect “high risk” cases and give them special attention.
To foresee complications and prevent them.
To remove anxiety and dread associated with delivery.
To reduce maternal and infant mortality and morbidity.
To teach the mother elements of child care, nutrition,
personal hygiene and environmental sanitation.
To sensitize the mother to the need for family planning,
including advice to cases seeking medical termination of
pregnancy.
To attend to the under fives accompanying the mother.
4. To promote, protect and maintain the health
of the mother during pregnancy
• Promote and maintain the
physical, mental and social
well-being of both the mother
and baby by providing
education on :
-danger signals
-nutrition
-rest
-sleep
-personal hygiene
PLUS the environment of the
pregnancy and birth;
* Keeping normal “normal”*
5. The “DANGER SIGNS” of pregnancy
1. Vaginal bleeding
2. Persistent vomiting
3. Fever with chills
4. Dysuria
5. Abdominal pain or cramping
6. Swelling of the face or fingers
7. Blurring of vision, dizziness, mental confusion, spots before
the eyes - signs of severe preeclampsia
8. Oliguria
9. Headaches
10. Leakage of fluid from vagina
11. Marked reduction in intensity or frequency of foetal
movements.
6. To reduce maternal and infant mortality
and morbidity:
India - where do we stand ?
1ST country in world with population policy
– 1976
2ND highest IMR in SEAR (68) below Timor-
Leste
3RD highest MMR (407), below Timor-Leste
(800) & Nepal (415) in SEAR
IMR halved in 50 years – still higher than in
developed countries, SL, Cuba & China
“SLOW PROGRESSORS” – WHR 2005
7.
8. To teach the mother elements of child care and
nutrition :
Nutrition Requirements:-
• A pregnancy in total consumes about
60000 kcal.
• Child survival – birth weight – weight gain
of mother
Good antenatal nutrition includes:-
• Meeting the caloric needs
• Eating foods which supply specific
micronutrients
• Providing micronutrient supplementation
• An underweight mother increases the
likelihood of a low birth weight (LBW) baby;
• Low iron intake contributes to anemia.
NUTRITIONAL ADVICE:
SIMPLE
REALISTIC
9. Additional nutritional requirements
in pregnancy
Calorie 150 kcal more in first trimester,
350 kcal more subsequently
Protein 60g (44 g in non-pregnant)
Major difference of RDA in pregnancy:
Folate 400 ug (180 ug in non-pregnant)
Calcium 1200 mg (800 mg in non-pregnant)
Iron 30 mg (15 mg in non-pregnant)
10. To sensitize the mother to the need for
family planning:
The mother is psychologically more receptive
to advice on family planning than at other
times.
If the mother has had 2 or more children, she
should be motivated for puerperal
sterilization.
All India hospital post partum programme.
11. To detect high risk cases and give them special
care:
The main goal of ANC in developing countries-
to identify and refer them at the appropriate
time.
Referred to a hospital facility where necessary
medical care and expertise is available.
This approach is known as the Risk Approach
(RA) strategy.
12. What constitutes a “high risk”
case?
1. Universal factors
1. Age < 16 yrs and > 35 years
2. Weight < 45 kgs or > 70 kgs
3. Height < 145 cms
4. Primigravidas / more than 4
children
5. Low socio-economic status
2. Medical disorders
complicating
pregnancy
1. Diabetes mellitus
2. Cardiac disease
3. Thyroid disease
4. Hypertension
5. Anaemia
6. Tuberculosis
•The following conditions are considered at risk and require the services
of a specialist gynaecologist :
13. 3. Previous poor obstetric
outcome
1. Recurrent abortions / Pregnancy
loss
2. Previous still birth / Intrauterine
death / neonatal death
3. Previous preterm labour /
premature rupture of membranes
4. History of congenital
malformations
4. Past Obstetric history
1. Small for dates (IUGR)
2. Large for dates
3. History of LSCS or myomectomy
4. Preterm labour
5. Preeclampsia / eclampsia
6. PPH / manual removal of placenta
5. Obstetrical conditions
in the present
pregnancy
1. Severe IUGR
2. Preeclampsia / eclampsia
3. Multiple pregnancy
4. Early pregnancy bleeding
5. Ante partum haemorrhage
6. Post-dated pregnancy
7. Malpresentations
8. Rh - ve pregnancy
14. Function properly only if the women
identified at risk agree to give birth in a
hospital on the one hand, and if they
can indeed reach this hospital on the
other hand.
Expected to significantly reduce
maternal morbidity and mortality.
Risk approach
15. “Risk approach”……less than ideal??
Risk approach is not an efficient or effective strategy for
maternal mortality reduction:
“Risk factors” cannot predict complications: usually not
direct cause of complication
What do you do once you identify risks? What about
“low risk?”
Maternal mortality is relatively rare in population at risk
(all women of reproductive age); “risk factors” are
relatively common in same population, these “risk
factors” do not appear to be good indicators of which
women will experience complications
Majority of women who experienced complication
were considered “low risk;” vast majority of women
considered to be “high risk” gave birth without
experiencing a complication
16. “Risk approach” ...a summary
“Risk factors,” = “factors associated with complications”
rather than “indicators” of complications.
Their importance for each pregnancy and childbirth
should be considered on individual basis.
Not recommend abandoning antenatal care.
Patients often have pre-existing disease, or develop
diseases during pregnancy that require care at regular
intervals
Antenatal care cannot be used to predict complications
later.
It is not useful as a screening tool.
It is important for detecting current problems and for
keeping the normal pregnancy, “normal."
17. To attend to the under fives accompanying the
mother
A pediatrician should be
present at all antenatal
clinics.
19. REFERENCES:
Prenatal care-Dr. Shalini Rajaram
WHO- Reproductive health research.
Park’s Text Book of Preventive and Social
medicine.
The Internet.