Biomedical Visualisation Volume11 Paul M Rea
download
https://ebookbell.com/product/biomedical-visualisation-
volume-11-paul-m-rea-46703898
Explore and download more ebooks at ebookbell.com
2.
Here are somerecommended products that we believe you will be
interested in. You can click the link to download.
Biomedical Visualisation Volume 7 Advances In Experimental Medicine
And Biology 1262 1st Ed 2020 Paul M Rea Editor
https://ebookbell.com/product/biomedical-visualisation-
volume-7-advances-in-experimental-medicine-and-biology-1262-1st-
ed-2020-paul-m-rea-editor-11191338
Biomedical Visualisation Volume 12 The Importance Of Context In
Imagemaking Leonard Shapiro
https://ebookbell.com/product/biomedical-visualisation-volume-12-the-
importance-of-context-in-imagemaking-leonard-shapiro-46171028
Biomedical Visualisation Volume 13 The Art Philosophy And Science Of
Observation And Imaging Leonard Shapiro
https://ebookbell.com/product/biomedical-visualisation-volume-13-the-
art-philosophy-and-science-of-observation-and-imaging-leonard-
shapiro-48702836
Biomedical Visualisation Volume 14 Covid19 Technology And
Visualisation Adaptations For Biomedical Teaching Ourania Varsou
https://ebookbell.com/product/biomedical-visualisation-
volume-14-covid19-technology-and-visualisation-adaptations-for-
biomedical-teaching-ourania-varsou-48723270
3.
Biomedical Visualisation Volume15 Visualisation In Teaching Of
Biomedical And Clinical Subjects Anatomy Advanced Microscopy And
Radiology Eiman Abdel Meguid
https://ebookbell.com/product/biomedical-visualisation-
volume-15-visualisation-in-teaching-of-biomedical-and-clinical-
subjects-anatomy-advanced-microscopy-and-radiology-eiman-abdel-
meguid-49464472
Biomedical Visualisation Volume 6 1st Ed Paul M Rea
https://ebookbell.com/product/biomedical-visualisation-volume-6-1st-
ed-paul-m-rea-22448156
Biomedical Visualisation Volume 8 1st Ed Paul M Rea
https://ebookbell.com/product/biomedical-visualisation-volume-8-1st-
ed-paul-m-rea-22505508
Biomedical Visualisation Volume 9 Paul M Rea
https://ebookbell.com/product/biomedical-visualisation-volume-9-paul-
m-rea-27986746
Biomedical Visualisation Volume 10 1st Edition Paul M Rea
https://ebookbell.com/product/biomedical-visualisation-volume-10-1st-
edition-paul-m-rea-34525266
5.
Advances in ExperimentalMedicine and Biology 1356
Paul M. Rea Editor
Biomedical
Visualisation
Volume 11
6.
Advances in ExperimentalMedicine
and Biology
Volume 1356
Series Editors
Wim E. Crusio, Institut de Neurosciences Cognitives et Intégratives
d’Aquitaine, CNRS and University of Bordeaux, Pessac Cedex, France
Haidong Dong, Departments of Urology and Immunology, Mayo Clinic,
Rochester, MN, USA
Heinfried H. Radeke, Institute of Pharmacology & Toxicology, Clinic of the
Goethe University Frankfurt Main, Frankfurt am Main, Hessen, Germany
Nima Rezaei, Research Center for Immunodeficiencies, Children’s Medical
Center, Tehran University of Medical Sciences, Tehran, Iran
Ortrud Steinlein, Institute of Human Genetics, LMU University Hospital,
Munich, Germany
Junjie Xiao, Cardiac Regeneration and Ageing Lab, Institute of Cardiovas-
cular Science, School of Life Science, Shanghai University, Shanghai, China
7.
Advances in ExperimentalMedicine and Biology provides a platform for
scientific contributions in the main disciplines of the biomedicine and the
life sciences. This series publishes thematic volumes on contemporary
research in the areas of microbiology, immunology, neurosciences, biochem-
istry, biomedical engineering, genetics, physiology, and cancer research.
Covering emerging topics and techniques in basic and clinical science, it
brings together clinicians and researchers from various fields.
Advances in Experimental Medicine and Biology has been publishing
exceptional works in the field for over 40 years, and is indexed in SCOPUS,
Medline (PubMed), Journal Citation Reports/Science Edition, Science Cita-
tion Index Expanded (SciSearch, Web of Science), EMBASE, BIOSIS,
Reaxys, EMBiology, the Chemical Abstracts Service (CAS), and Pathway
Studio.
2020 Impact Factor: 2.622
More information about this series at https://link.springer.com/bookseries/5584
Editor
Paul M. Rea
AnatomyFacility, School of Life Sciences
University of Glasgow
Glasgow, United Kingdom
ISSN 0065-2598 ISSN 2214-8019 (electronic)
Advances in Experimental Medicine and Biology
ISBN 978-3-030-87778-1 ISBN 978-3-030-87779-8 (eBook)
https://doi.org/10.1007/978-3-030-87779-8
# The Editor(s) (if applicable) and The Author(s), under exclusive license to Springer Nature
Switzerland AG 2022
This work is subject to copyright. All rights are solely and exclusively licensed by the Publisher,
whether the whole or part of the material is concerned, specifically the rights of translation,
reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any
other physical way, and transmission or information storage and retrieval, electronic adaptation,
computer software, or by similar or dissimilar methodology now known or hereafter developed.
The use of general descriptive names, registered names, trademarks, service marks, etc. in this
publication does not imply, even in the absence of a specific statement, that such names are
exempt from the relevant protective laws and regulations and therefore free for general use.
The publisher, the authors, and the editors are safe to assume that the advice and information in
this book are believed to be true and accurate at the date of publication. Neither the publisher nor
the authors or the editors give a warranty, expressed or implied, with respect to the material
contained herein or for any errors or omissions that may have been made. The publisher remains
neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This Springer imprint is published by the registered company Springer Nature Switzerland AG.
The registered company address is: Gewerbestrasse 11, 6330 Cham, Switzerland
10.
Preface
The utilisation oftechnologies in the biomedical and life sciences, medicine,
dentistry, surgery, veterinary medicine and surgery, and the allied health
professions has grown at an exponential rate over recent years. The way we
view and examine data now is significantly different to what has been done
over recent years.
With the growth, development and improvement of imaging and data
visualisation techniques, the way we are able to interact with data is much
more engaging than it has ever been.
These technologies have been used to enable improved visualisation in the
biomedical fields, but also how we engage our future generations of
practitioners when they are students within our educational environment.
Never before have we had such a wide range of tools and technologies
available to engage our end-stage user. Therefore, it is a perfect time to
bring this together to showcase and highlight the great investigative works
that is going on globally.
This book will truly showcase the amazing work that our global colleagues
are investigating, and researching, ultimately to improve student and patient
education, understanding and engagement. By sharing best practice and
innovation we can truly aid our global development in understanding how
best to use technology for the benefit of society as a whole.
Glasgow, UK Paul M. Rea
v
11.
Acknowledgements
I would liketo truly thank every author who has contributed to the eleventh
edition of Biomedical Visualisation. By sharing our innovative approaches we
can truly benefit students, faculty, researchers, industry, and beyond, in our
quest for the best uses of technologies and computers in the field of life
sciences, medicine, the allied health professions, and beyond. In doing so,
we can truly improve our global engagement and understanding about best
practice in the use of these technologies for everyone. Thank you!
I would also like to extend a personal note of thanks to the team at Springer
Nature who have helped make this possible. The team I have been working
with have been so incredibly kind and supportive, and without you, this would
not have been possible. Thank you kindly!
vii
12.
About the Book
Followingon from the success of the first ten volumes, Biomedical
Visualisation, Volume 11, will demonstrate the numerous options we have
in using technology to enhance, support, and challenge education, clinical
settings, and professional training. The chapters presented here highlight the
wide use of tools, techniques, and methodologies we have at our disposal in
the digital age. These can be used to image the human body, to educate
patients, the public, faculty, and students in the plethora of how to use
cutting-edge technologies in visualising the human body and its processes,
to create and integrate platforms for teaching and education, to visualise
biological structures and pathological processes, and to aid visualisation of
the historical arenas.
The chapters presented in this volume cover such a diverse range of topics,
with something for everyone. We present here chapters on 3D visualising
novel stent grafts to aid treatment of aortic aneurysms, confocal microscopy
constructed vascular models in patient education, 3D patient-specific virtual
reconstructions in surgery, virtual reality in upper limb rehabilitation in
patients with multiple sclerosis, and virtual clinical wards.
In addition, we present chapters on artificial intelligence in ultrasound-
guided regional anaesthesia, carpal tunnel release visualisation techniques,
visualising for embryology education, and artificial intelligence data on bone
mechanics.
Finally, we conclude with chapters on visualising patient communication
in a general practice setting, digital facial depictions of people from the past,
instructor made cadaveric videos, novel cadaveric techniques for enhancing
visualisation of the human body, and finally, interactive educational videos
and screencasts.
ix
13.
Contents
1 Creating InteractiveThree-Dimensional Applications to
Visualise Novel Stent Grafts That Aid in the Treatment
of Aortic Aneurysms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Sara Bakalchuk, Caroline Walker, Craig Daly, Louise Hill,
and Matthieu Poyade
2 Using Confocal Microscopy to Generate an Accurate
Vascular Model for Use in Patient Education Animation . . . . 31
Angela Douglass, Gillian Moffat, and Craig Daly
3 Methods and Applications of 3D Patient-Specific Virtual
Reconstructions in Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . 53
Jordan Fletcher
4 Proof of Concept for the Use of Immersive Virtual Reality
in Upper Limb Rehabilitation of Multiple Sclerosis
Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
Rachel-Anne Hollywood, Matthieu Poyade, Lorna Paul,
and Amy Webster
5 Virtual Wards: A Rapid Adaptation to Clinical
Attachments in MBChB During the COVID-19 Pandemic . . . 95
Camille Huser, Kerra Templeton, Michael Stewart,
Safiya Dhanani, Martin Hughes, and James G. Boyle
6 Artificial Intelligence: Innovation to Assist in the
Identification of Sono-anatomy for Ultrasound-Guided
Regional Anaesthesia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 117
James Lloyd, Robert Morse, Alasdair Taylor, David Phillips,
Helen Higham, David Burckett-St. Laurent,
and James Bowness
7 A Systematic Review of Randomised Control Trials
Evaluating the Efficacy and Safety of Open and Endoscopic
Carpal Tunnel Release . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
Eilidh MacDonald and Paul M. Rea
xi
14.
8 Exploring Visualisationfor Embryology Education:
A Twenty-First-Century Perspective . . . . . . . . . . . . . . . . . . . 173
Eiman M. Abdel Meguid, Jane C. Holland, Iain D. Keenan,
and Priti Mishall
9 How Artificial Intelligence and Machine Learning
Is Assisting Us to Extract Meaning from Data on Bone
Mechanics? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 195
Saeed Mouloodi, Hadi Rahmanpanah, Colin Martin,
Soheil Gohari, and Helen M. S. Davies
10 Visual Communication and Creative Processes Within the
Primary Care Consultation . . . . . . . . . . . . . . . . . . . . . . . . . . 223
Holly Quinton
11 Digital 2D, 2.5D and 3D Methods for Adding
Photo-Realistic Textures to 3D Facial Depictions
of People from the Past . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 245
Mark Roughley and Ching Yiu Jessica Liu
12 Teaching with Cadavers Outside of the Dissection Room
Using Cadaveric Videos . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 281
Danya Stone, Catherine M. Hennessy, and Claire F. Smith
13 A Novel Cadaveric Embalming Technique for Enhancing
Visualisation of Human Anatomy . . . . . . . . . . . . . . . . . . . . . . 299
Brian Thompson, Emily Green, Kayleigh Scotcher,
and Iain D. Keenan
14 Assessing the Impact of Interactive Educational Videos
and Screencasts Within Pre-clinical Microanatomy
and Medical Physiology Teaching . . . . . . . . . . . . . . . . . . . . . 319
Alistair Robson, Yarrow Scantling-Birch, Stuart Morton,
Deepika Anbu, and Scott Border
xii Contents
15.
Editor and Contributors
Aboutthe Editor
Paul M. Rea is a Professor of Digital and Anatomical Education at the
University of Glasgow. He is qualified with a medical degree (MBChB), an
MSc (by research) in craniofacial anatomy/surgery, a PhD in neuroscience,
the Diploma in Forensic Medical Science (DipFMS), and an MEd with Merit
(Learning and Teaching in Higher Education). He is an elected Fellow of the
Royal Society for the Encouragement of Arts, Manufactures and Commerce
(FRSA), elected Fellow of the Royal Society of Biology (FRSB), Senior
Fellow of the Higher Education Academy, professional member of the Insti-
tute of Medical Illustrators (MIMI), and a registered medical illustrator with
the Academy for Healthcare Science.
Paul has published widely and presented at many national and international
meetings, including invited talks. He sits on the Executive Editorial Committee
for the Journal of Visual Communication in Medicine, is Associate Editor for the
European Journal of Anatomy, and reviews for 25 different journals/publishers.
He is the Public Engagement and Outreach lead for anatomy coordinating
collaborative projects with the Glasgow Science Centre, NHS, and Royal
College of Physicians and Surgeons of Glasgow. Paul is also a STEM ambas-
sador and has visited numerous schools to undertake outreach work.
His research involves a long-standing strategic partnership with the School
of Simulation and Visualisation, The Glasgow School of Art. This has led to
multi-million pound investment in creating world-leading 3D digital datasets to
be used in undergraduate and postgraduate teaching to enhance learning and
assessment. This successful collaboration resulted in the creation of the world’s
first taught MSc Medical Visualisation and Human Anatomy combining anat-
omy and digital technologies. The Institute of Medical Illustrators also accredits
it. It has created college-wide, industry, multi-institutional, and NHS research
linked projects for students. Paul is the Programme Director for this degree.
Contributors
Deepika Anbu Centre for Learning Anatomical Sciences, Primary Care,
Population Sciences and Medical Education, Mailpoint 845, University
Hospital Southampton, Southampton, UK
xiii
16.
Sara Bakalchuk AnatomyFacility, School of Life Sciences, College of
Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow, UK
School of Simulation and Visualisation, Glasgow School of Art, Glasgow,
UK
Scott Border Centre for Learning Anatomical Sciences, Primary Care,
Population Sciences and Medical Education, Mailpoint 845, University
Hospital Southampton, Southampton, UK
James G. Boyle School of Medicine, University of Glasgow, Glasgow, UK
NHS Greater Glasgow and Clyde, Glasgow, UK
James Bowness Aneurin Bevan University Health Board, University of
Oxford, Oxford, UK
David Burkett-St Laurent Royal Cornwall Hospitals NHS Trust, Truro,
UK
Craig Daly School of Life Sciences, College of Medical, Veterinary and Life
Sciences, University of Glasgow, Glasgow, UK
Helen M. S. Davies Department of Veterinary Biosciences, University of
Melbourne, Melbourne, VIC, Australia
Safiya Dhanani School of Medicine, University of Glasgow, Glasgow, UK
NHS Greater Glasgow and Clyde, Glasgow, UK
Angela Douglass Anatomy Facility, School of Life Sciences, College of
Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow, UK
School of Simulation and Visualisation, Glasgow School of Art, Glasgow,
UK
Jordan Fletcher St Mark’s Hospital, Harrow, UK
Soheil Gohari Department of Mechanical Engineering, University of
Melbourne, Melbourne, VIC, Australia
Emily Green School of Medical Education, Newcastle University,
Newcastle upon Tyne, UK
Helen Higham Oxford University Hospitals NHS Foundation Trust,
London, UK
Louise Hill Terumo Aortic, Renfrewshire, UK
Jane C. Holland Department of Anatomy, RCSI University of Medicine and
Health Sciences, Dublin, Ireland
Rachel-Anne Hollywood Department of Physiotherapy and Paramedicine,
Glasgow Caledonian University, Glasgow, UK
Martin Hughes School of Medicine, University of Glasgow, Glasgow, UK
NHS Greater Glasgow and Clyde, Glasgow, UK
Camille Huser School of Medicine, University of Glasgow, Glasgow, UK
xiv Editor and Contributors
17.
Iain D. KeenanSchool of Medical Education, Newcastle University,
Newcastle upon Tyne, UK
Jessica Liu Liverpool School of Art and Design, Liverpool John Moores
University, Liverpool, UK
James Lloyd Aneurin Bevan University Health Board, Newport, UK
Eilidh Macdonald Anatomy Facility, School of Life Sciences, College of
Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow, UK
Colin Martin Department of Veterinary Biosciences, University of
Melbourne, Melbourne, VIC, Australia
Eiman M. Abdel Meguid Centre for Biomedical Sciences Education,
School of Medicine, Dentistry and Biomedical Sciences, Queen’s University
Belfast, Belfast, UK
Priti Mishall Department of Anatomy and Structural Biology and Depart-
ment of Ophthalmology and Visual Sciences, Albert Einstein College of
Medicine, Bronx, NY, USA
Gillian Moffat School of Simulation and Visualisation, Glasgow School of
Art, Glasgow, UK
Stuart Morton Centre for Learning Anatomical Sciences, Primary Care,
Population Sciences and Medical Education, Mailpoint 845, University
Hospital Southampton, Southampton, UK
Robert Morse Intelligent Ultrasound Limited, Cardiff, UK
Saeed Mouloodi Department of Mechanical Engineering, University of
Melbourne, Melbourne, VIC, Australia
Lorna Paul Department of Physiotherapy and Paramedicine, Glasgow
Caledonian University, Glasgow, UK
David Phillips Aneurin Bevan University Health Board, Newport, UK
Matthieu Poyade School of Simulation and Visualisation, Glasgow School
of Art, Glasgow, UK
Holly Quinton TBC, London, UK
Hadi Rahmanpanah Department of Mechanical Engineering, University of
Melbourne, Melbourne, VIC, Australia
Paul M. Rea Anatomy Facility, School of Life Sciences, College of Medical,
Veterinary and Life Sciences, University of Glasgow, Glasgow, UK
Alistair Robson Centre for Learning Anatomical Sciences, Primary Care,
Population Sciences and Medical Education, Mailpoint 845, University
Hospital Southampton, Southampton, UK
Mark Roughley Liverpool School of Art and Design, Liverpool John
Moores University, Liverpool, UK
Editor and Contributors xv
18.
Yarrow Scantling-Birch Centrefor Learning Anatomical Sciences, Primary
Care, Population Sciences and Medical Education, Mailpoint 845, University
Hospital Southampton, Southampton, UK
Kayleigh Scotcher School of Medical Education, Newcastle University,
Newcastle upon Tyne, UK
Michael Stewart School of Medicine, University of Glasgow, Glasgow, UK
NHS Greater Glasgow and Clyde, Glasgow, UK
Alasdair Taylor NHS Tayside, Dundee, UK
Kerra Templeton School of Medicine, University of Glasgow, Glasgow,
UK
NHS Greater Glasgow and Clyde, Glasgow, UK
Brian Thompson School of Medical Education, Newcastle University,
Newcastle upon Tyne, UK
Caroline Walker Anatomy Facility, School of Life Sciences, College of
Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow, UK
School of Simulation and Visualisation, Glasgow School of Art, Glasgow,
UK
Amy Webster Department of Physiotherapy and Paramedicine, Glasgow
Caledonian University, Glasgow, UK
xvi Editor and Contributors
19.
Creating Interactive Three-Dimensional
Applicationsto Visualise Novel Stent
Grafts That Aid in the Treatment
of Aortic Aneurysms
1
Sara Bakalchuk, Caroline Walker, Craig Daly, Louise Hill,
and Matthieu Poyade
Abstract
Three-Dimensional (3D) medical animations
incorporated into applications are highly ben-
eficial for clinical outreach and medical com-
munication purposes that work towards
educating the clinician and patient. Aortic
aneurysms are a clinically important area to
communicate with multiple audiences about
various treatment options; both abdominal
and thoracic aortic aneurysms were selected
to create 3D animations and applications to
educate medical professionals and patients
regarding treatment options. Fenestrated
endovascular aortic repair (FEVAR) and tho-
racic endovascular aortic repair (TEVAR) are
both tried and tested minimally invasive surgi-
cal methods for treating thoracic aortic
aneurysms respectively. The Terumo Aortic
Custom Relay Proximal Scalloped stent graft
and Fenestrated Anaconda stent graft were
both designed specifically for these
procedures; however, it can be difficult to
visually communicate to clinicians and
patients in a straightforward way how these
devices work. Therefore, we have developed
two interactive applications that use 3D
visualisation techniques to demonstrate how
these aortic devices function and are
implemented. The objective of these
applications is to engage both clinicians and
patients, therefore demonstrating that the addi-
tion of anatomically accurate 3D visualisations
within an interactive interface would have a
positive impact on public engagement while
also ensuring that clinicians will have the best
possible understanding of the potential uses of
both devices, enabling them to exploit their
key features to effectively broaden the treat-
able patient population.
Detailed anatomical modelling and anima-
tion was used to generate realistic and accurate
rendered videos showcasing both products.
These videos were integrated into an interac-
tive application within a modern, professional
graphic interface that allowed the user to
explore all aspects of the stent device. The
resulting applications were broken down into
three modules: deployment, clinical perfor-
mance and features. Following application
development, these applications were
S. Bakalchuk · C. Walker (*)
Anatomy Facility, School of Life Sciences, College of
Medical, Veterinary and Life Sciences, University of
Glasgow, Glasgow, UK
School of Simulation and Visualisation, Glasgow School
of Art, Glasgow, UK
e-mail: cmw93@cam.ac.uk
C. Daly
School of Life Sciences, College of Medical, Veterinary
and Life Sciences, University of Glasgow, Glasgow, UK
L. Hill
Terumo Aortic, Glasgow, UK
M. Poyade
School of Simulation and Visualisation, Glasgow School
of Art, Glasgow, UK
# The Author(s), under exclusive license to Springer Nature Switzerland AG 2022
P. M. Rea (ed.), Biomedical Visualisation, Advances in Experimental Medicine and Biology 1356,
https://doi.org/10.1007/978-3-030-87779-8_1
1
20.
evaluated by professionalsin the field. Over-
all, positive feedback was received regarding
the user-friendly nature of the applications and
highly effective animations to showcase the
products. The clinical applications and feature
modules were particularly successful, while
the deployment modules had a neutral
response. Biomedical applications such as
these show great potential for communicating
the key features of medical devices and pro-
moting discussion between clinicians and
patients; further testing would need to be
conducted on a larger group of participants in
order to validate the learning effectiveness of
the applications.
Keywords
Abdominal aortic aneurysms · Thoracic aortic
aneurysms · Interactive application · 3D
modelling · Medical animation · Medical
communication
1.1 Introduction
Communicating novel medical devices in a visu-
ally logical and innovative way is essential in the
changing healthcare climate, specifically for
diseases with alternative treatment options that
healthcare professionals may not be aware
of. The methodology described in this paper
outlines the use of cutting-edge technologies to
visualise treatment approaches that clinicians can
use to enhance treatment of aortic aneurysms.
Aortic aneurysms can be subcategorised into
abdominal and thoracic aneurysms, depending on
the location of the swelling and site of rupture.
Aortic aneurysms are leading causes of death
globally. While both abdominal aortic aneurysms
(AAAs) and thoracic aortic aneurysms (TAAs)
contribute to this, abdominal aneurysms specifi-
cally are the tenth leading cause of death globally
(Howard et al. 2015). Although advanced treat-
ment options can help reduce mortality rates, it is
essential to increase the awareness of clinicians
about novel stent grafts that can reduce the risk of
rupture and help treat both AAAs and TAAs with
complex aortic anatomy (Filardo et al. 2015).
Fenestrated endovascular aortic repair
(FEVAR) and thoracic endovascular aortic repair
(TEVAR) are tried and tested minimally invasive
surgical methods for treating AAAs and TAAs
with novel stent grafts. It can be difficult to visu-
ally communicate to clinicians how these stent
grafts work in real time; thus, the visualisations
created would subsequently benefit patient out-
come specifications through a series of three-
dimensional (3D) animations embedded into
interactive applications. These applications
ensure that clinicians have the best possible
understanding of the potential uses of the medical
devices, enabling them to exploit key features to
effectively broaden the treatable patient popula-
tion of both AAAs and TAAs. Thus, the resulting
applications should have a positive impact while
ensuring that clinicians understand the potential
uses and customisations of the two visualised
stent grafts—the Fenestrated Anaconda stent
graft and the Relay Proximally Scalloped stent
graft—to treat juxtarenal aneurysms and thoracic
aneurysms involving the arch, respectively.
Advances in stent graft surgical techniques
and treatment options have led to the need for
the creation of interactive applications to engage
healthcare workers and increase their knowledge
of alternative devices for better patient treatment.
This visualisation research explores the method-
ology of creating anatomically correct models
and animations for an interactive application.
Through collaboration with Terumo Aortic, two
applications were generated by creating multiple
3D medical animations from anatomically accu-
rate models for use in public and medical engage-
ment outreach. Various 3D modelling and
animation techniques, as well as application
development software, were utilised in order to
produce the animations that would showcase the
most important characteristics of the Fenestrated
and Relay devices. The visualisation approaches
used to create scientific animations in 3D
programs were unique and are discussed through-
out the paper. The research and methodologies
used to create these scientific animations and
corresponding applications show a useful way of
communicating advanced medical devices
through cutting-edge, intuitive, technological
methods.
2 S. Bakalchuk et al.
21.
1.2 Background
This chapterreviews the global problem of aortic
aneurysms in the elderly population and explores
the surgical interventions and technology needed
to visualise surgical techniques, thus generating
understanding and awareness of the disease.
1.2.1 Aortic Aneurysm Background
An aortic aneurysm can be defined as a swelling
or bulging at any point along the aorta. An aneu-
rysm is a blood vessel that results in a permanent
dilation by at least 150% of the regular vessel
diameter (Shaw et al. 2020). A neurysms are
most likely to occur at the section of the aorta
where the wall is weakened and has lost its elastic
properties, as it does not return to its normal shape
after the blood has passed through (British Heart
Foundation 2020). If the dilation is left untreated,
vessel wall degeneration progresses, leading to an
increase in swelling and thinning of the vessel
wall. The risk of rupture is directly correlated
with the increase of aneurysm diameter (Avishay
and Reimon 2020). Aortic aneurysms can be
subcategorised into abdominal and thoracic aortic
aneurysms, depending on the location of the
swelling. Aortic aneurysms are classified as either
small or large, 3–5 cm and > 5 cm, respectively
(Powell et al. 2011). Approximately of aortic
aneurysms occur in the abdomen; the remainder
are thoracic aneurysms (Kuivaniemi et al. 2015).
The aneurysm requires close monitoring or treat-
ment once detected as the aortic wall can continue
to weaken over time and be unable to withstand
the pressing blood pressure forces, resulting in
rupture (Filardo et al. 2015). The level of stress
on the wall is directly proportional to an increase
in aortic diameter and is considered to be a signif-
icant factor in the growth rate of aneurysms.
1.2.1.1 Thoracic Aortic Aneurysms
Thoracic aortic aneurysms (TAAs) make up
approximately of aneurysms (British Heart Foun-
dation 2020) and are characterised by swelling or
bulging of the aorta within the region of the chest.
TAAs may involve one or more aortic segments,
either the aortic root, ascending aorta, arch, or
descending aorta. Sixty percent of thoracic aortic
aneurysms involve the aortic root and/or ascending
aorta, involve the descending aorta, involve the
arch, and involve the thoracoabdominal aorta
(with some involving >1 segment) (Isselbacher
2005). The treatment of thoracic aneurysms differs
for each of these segments. If the aneurysm were to
rupture, immediate surgery is required to repair the
aorta with numerous possible surgical
interventions depending on the severity and pro-
gression. While open surgery used to be the indus-
try standard for this type of procedure, it is
becoming increasingly common to perform mini-
mally invasive endovascular operations using a
custom stent graft (Ben Abdallah et al. 2016).
1.2.1.2 Abdominal Aortic Aneurysms
Abdominal aortic aneurysm (AAA) is a life-
threatening condition that affects the aorta and
account for 75% of all aortic aneurysms
(Kuivaniemi et al. 2015). AAAs are often detected
incidentally due to their asymptomatic nature
(Kuivaniemi et al. 2015). AAAs are responsible
for approximately 5000 deaths in the UK every
year and more than 175,000 deaths globally
(Howard et al. 2015). One percent of deaths in
men over 68 years are attributed to ruptured
AAA, coming in as the tenth leading cause of
death in older men (Avishay and Reimon 2020).
The mortality rate of a ruptured AAA is over; thus
early diagnosis, monitoring and treatment are criti-
cal before the aneurysm’s rupture (Howard et al.
2015). Undetected, untreated AAAs result in
expansion, rupture, haemorrhage and often death
(Howard et al. 2015).
1.2.2 Surgical Interventions for AAAs
and TAAs
1.2.2.1 Open Surgical Repair
and Endovascular Aneurysm
Repair of AAAs
Treatment of large abdominal aortic aneurysms is
changing over time to include more advanced
surgical techniques for higher-risk patients. Treat-
ment is suggested when the aneurysm reaches
5 cm to 5.5 cm to prevent rupture and its
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 3
22.
corresponding high mortalityrate (Wang et al.
2018). Treatment options include open surgical
repair (OSR), endovascular aneurysm repair
(EVAR) and FEVAR (Wang et al. 2018).
Open surgical repair (OSR) has been the tradi-
tional clinical method for AAA (Wang et al.
2018). While rupture has an 80% mortality rate
(Dueck et al. 2004; Heikkinen et al. 2002; Ashton
et al. 2002), elective surgical repair of unruptured
AAA has only a 2–6% 30-day mortality rate
(Brown et al. 2012; Cosford and Leng 2007).
Endovascular aneurysm repair (EVAR) is a
recommended surgical substitute for AAA
higher-risk patients who are unsuitable for open
repair (De Bruin et al. 2010). However, up to 45%
of individuals with AAA are not suitable for
EVAR. Advanced AAA cases such as patients
with juxtarenal, thoracoabdominal and pararenal
aneurysms, or short, angulated or reversed aortic
neck anatomy, cannot be treated by EVAR
endografts (Dijkstra et al. 2014). This percentage
of AAAs are unsuitable for EVAR surgery but
can safely undergo fenestrated endovascular
aneurysm (FEVAR) device surgery. FEVAR
treatment is a minimally invasive surgery that
allows the aorta to be repaired in the patient’s
groin or arms while preserving blood flow to
major arteries (Park et al. 1996). EVAR treatment
with a fenestrated endovascular aneurysm
(FEVAR) device was introduced in 1996 to com-
bat complex aneurysms (Park et al. 1996).
Custom-made devices for FEVAR are now
utilised in patients that are higher risk for open
repair surgery. These stent grafts allow clinicians
to accommodate renal and mesenteric vessels by
inserting custom devices where disease progres-
sion has occurred, higher up in the aorta (Colgan
et al. 2018). FEVAR has since shown high tech-
nical success rate, low mortality, and short, inter-
mediate and long-term complication rates
(Bungay et al. 2011). As a result, Terumo Aortic
has developed a fenestrated graft stent system, the
Fenestrated Anaconda™, as seen in Fig. 1.1.
1.2.2.2 Open Surgical Repair
and Endovascular Aneurysm
Repair of TAAs
In order to decide whether to perform elective,
pre-emptive aneurysmectomy, the specific risk
versus benefit from resection needs to be
estimated, which ultimately depends on the surgi-
cal method chosen (Elefteriades 2002). Open-
chest surgical repair using prosthetic graft inter-
position has been the conventional treatment for
TAAs (Abraha et al. 2009). However, despite
improvements in surgical procedures, periopera-
tive complications remain significant. The alter-
native option of thoracic endovascular aneurysm
repair (TEVAR) is considered a less invasive and
potentially safer technique, with lower morbidity
and mortality compared to open surgical repair,
making it an appealing therapeutic option (Alsafi
et al. 2014). Fortunately, this approach is becom-
ing increasingly common, as both acute and
chronic traumatic lesions of the descending aorta
can be treated via an endovascular approach in
specialised centres, with low morbidity and mor-
tality rates (Kato et al. 1997). Endovascular repair
is particularly attractive for treating patients
whose associated injuries or comorbid conditions
put them at greater risk for the open-chest repair
surgery (Kasirajan et al. 2003).
Fig. 1.1 (a) Fenestrated Anaconda stent graft and (b)
Fenestrated Anaconda device and aneurysm with angula-
tion device stents and legs (Vascutek Lmtd. 2020)
4 S. Bakalchuk et al.
23.
The main advantagesof the endovascular pro-
cedure include shorter time and lower operative
risk. If the patient is not affected by other high-
priority life-threatening injuries, endovascular
repair should be performed first before any other
surgical treatment in order to eliminate the risk of
sudden aortic rupture (Ferrari et al. 2006). Another
benefit of this surgical technique is the absence of
cardiopulmonary bypass and the low-dose sys-
temic heparinisation (Ferrari et al. 2006). Despite
great achievements from endovascular stent grafts,
several complications of endovascular stenting
have remained. Although complications do not
occur frequently, endoleak, stent collapse, subcla-
vian occlusion, stroke, embolisation, bronchial
obstruction, implant syndrome, dissection, migra-
tion and paralysis may develop (Karmy-Jones et al.
2009). When the treatment segment of the thoracic
aorta, most commonly the aortic arch, present cer-
tain anatomical challenges, technically complex
stent graft designs are sometimes needed. There-
fore, endovascular treatment of aortic arch disease
may require a custom-made endograft to maintain
the patency of the supra-aortic trunks (SATs) in the
event of a short healthy proximal aortic neck
(Fernández-Alonso et al. 2018). In specific cases
such as these, the custom Terumo Aortic Relay
proximal scalloped stent graft has been particularly
successful (Fig. 1.2). Consequently, anatomically
accurate and interactive 3D visualisations of this
product would be helpful for communicating its
correct usage and other various benefits to both
patients and clinicians.
1.2.3 Potential of Medical
Visualisations for Surgical
Techniques
1.2.3.1 Imaging Modalities
in a Healthcare Setting
In today’s clinical setting, medical imaging is an
essential component of the entire healthcare con-
tinuum, from wellness and screening to early
diagnosis, treatment selection and follow-up.
Some of the most common imaging modalities
used today are computed tomography (CT) and
magnetic resonance imaging (MRI) (Liu et al.
2007). CT imaging allows for clinicians to gain
high levels of detail for anatomical structures and
soft tissue, while MRI [T1 and T2] can assess not
only morphology but also metabolic function
detected by changes in blood flow.
Advancements in computer graphics have
allowed for fast, real-time medical imaging inter-
pretation, giving radiologists the ability to process
a huge amount of data, compare prior studies and
create multiplanar and three-dimensional image
reconstructions. This is done through very thin
(fractions of a millimetre) slices obtained, for
example, in the DICOM image format, and sub-
sequently segmented in an editing software such
as 3D Slicer, Amira, MITK, ITK and Osirix. The
3D volume generated from these imaging
modalities allows for accurate and efficient
visualisation of the patient’s anatomy and physi-
ology (Bercovich and Javitt 2018). CT and MRI
visualisation combined with interactive technol-
ogy allowing for 3D reconstructions will continue
to further the understanding of human disease and
allow a personalised approach to treatment plans.
The process of converting medical imaging
into 3D visualisations follows a general imaging
pipeline (Fig. 1.3). A summary of this pipeline is
as follows: acquiring data, analysing and
visualising medical images for use in diagnosis,
education, or research purposes. Medical imaging
is especially useful to help guide surgical
procedures and enable correct spatial accuracy
visualisation in connection with understanding
cardiac-related complications. Advanced cardiac
CT visualisation technology such as coronary CT
angiography (CTA) is an innovative clinical
imaging tool that allows a non-invasive and
highly specific approach for cardiac diagnosis
and treatment (Saremi 2017; Coelho-Filho et al.
2013; Burt et al. 2014). As aforementioned, gen-
eration of a 3D model from a CT scan can be used
for many reasons to increase patient understand-
ing, surgical planning and informing clinicians
understanding of medical devices for specific
patient treatment (Bercovich and Javitt 2018).
1.2.3.2 Public Engagement for Medical
Visualisation
When examining 3D visualisation for education,
it is also important to consider how well these
technologies are able to educate or otherwise
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 5
24.
engage a broaderaudience (Holliman et al. 2009).
Public engagement with science is an important
aspect of society at a number of levels (Taylor and
Wessels 2019). The ability of the public to under-
stand healthcare information is particularly
important, as it has been shown that adults with-
out sufficient health literacy are twice as likely to
be hospitalised than those with an adequate
understanding (Baker et al. 1998; Baker et al.
2002). Furthermore, public engagement with sci-
ence is vital to scientific progress as well, as the
incorporation of new media technologies has
increased the opportunities available for scientists
to engage the general public in understanding
their work (Holliman et al. 2009). Previous
work has shown the use of mobile technology or
tablets to access information and learning
materials from anywhere and at any time is par-
ticularly effective for this type of engagement
(Ford and Leinonen 2009). This allows for the
user to learn at their own pace and time, following
whatever information they find interesting and
therefore building a broader knowledge base
(Traxler 2007). These research findings define
the need for producing a means of visualising
various surgical methods to treat aortic aneurysms
to clinicians, patients, and the general public.
Overall, the use of imaging modalities in
healthcare to better treat and diagnose diseases
shows the value that visualisations bring to under-
standing and educating about medical conditions.
This displays the need for a public engagement
tool for aortic aneurysms that are frequent in the
elderly population. These research findings define
the need for producing a means of visualising
various surgical methods to treat aortic aneurysms
to clinicians, patients, and the general public. This
informative application, surrounding two differ-
ent types of aneurysms, will generate awareness
regarding surgical methods, customisable treat-
ment options, clinical performance success statis-
tics, risk factors, and awareness of innovative
stent grafts for AAA and TAA cases.
Fig. 1.2 (a) Terumo Aortic Relay proximal scalloped endograft. (b) Schematic showing a scalloped stent graft with the
radiopaque markers used during positioning (Alsafi et al. 2014)
6 S. Bakalchuk et al.
25.
1.3 Methods
The purposeof this project was to create clear,
informative, and anatomically accurate interactive
applications that communicate the important facts
and figures concerning both aforementioned stent
grafts. Specifically, 3D animations and anatomical
models will be utilised to highlight the key features
of the product, its deployment and its clinical
performance. The below sections will demonstrate
how the surgical techniques work for patients and
will help ensure that clinicians have the best possi-
ble understanding of the potential uses of the
devices. Therefore, these applications will enable
clinicians to have an understanding of the alterna-
tive medical devices and exploit their key features
to effectively broaden the treatable patient
population.
1.3.1 Conceptual Development
(Storyboard/Outline)
This stage commenced with conceptual ideation,
which subsequently led to the creation of a story-
board and mood board. A contact at Terumo
Aortic was consulted regarding exactly what
they were looking for within the applications,
and their specifications were used to create a
storyboard and mood board in keeping with
their desires and graphic style. The storyboard
specifically allowed for a clear idea of the flow
of the applications, as well as identifying the
key features to be highlighted. The storyboards
for both applications are depicted in Figs. 1.4
and 1.5.
1.3.2 Digital 3D Content Production
Once the flow of the applications was developed,
3D content production began for both
applications. This was composed of segmenta-
tion, retopology, 3D modelling, and texturing.
These assets were then used to create animated
videos and integrated into the 3D applications
within Unity.
1.3.2.1 Segmentation of the Aorta,
Kidneys and Associated Vessels
Open-source software 3D Slicer for medical
image informatics was utilised to segment the
aorta and surrounding anatomy that were
generated into 3D models and incorporated into
the 3D animations. Contrast and brightness were
manipulated to allow visualisation of distinct
anatomical structures; this allowed for precise
segmentation from medical data. Segmentation
was completed by using the editor module and
utilising the paint brush tool with a threshold of
100 to 1000. Segmentation was repeated, moving
through every slide of the dataset and manually
segmenting the needed organs. Once the models
were created, they were decimated by 20% to
Fig. 1.3 Imaging pipeline
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 7
26.
Fig. 1.4 TAAapplication storyboard
Fig. 1.5 AAA application storyboard
8 S. Bakalchuk et al.
27.
reduce the polycount.Models were then exported
in OBJ format for use across Autodesk platforms.
The same segmentation process was repeated for
the kidney, renals, and celiac vessels.
The lung model for the TAA application
followed a similar pipeline. It was first created
in slicer based off the CT chest pre-set. The Fast-
Marching tool within the editor module was
utilised to segment the lungs, while the threshold
paint tool was used to segment the trachea and
bronchi. The Surface toolbox was then used to
smooth the model and fill the holes. Figure 1.6
shows the segmentation process and the final
model rendered within 3D Slicer.
1.3.2.2 Bifrost Visual Programming
1.3.2.2.1 Voxel Volume Remeshing Using
Bifrost Graph Editor
Bifrost Graph is a Maya Plugin with a new visual
programming framework that generates voxel
volumes from 3D graphics. This was used due
to the complexity of the generated segmented
models from 3D Slicer; the models were unable
to be retopologised automatically with the high
polygon count generated in 3D Slicer. The step-
by-step process can be found in Fig. 1.7; the
images describe the Bifrost workflow utilised to
achieve the desired new Maya mesh. This process
was applied to all 3D Slicer models, so that there
were had manageable polycounts in Maya. The
end result is a new model with clean Maya mesh;
voxelating and rebuilding the mesh in Bifrost
fixed the holes in the mesh, lamina faces, and
nonmanifold geometry. It was important to per-
form Bifrost visual programming framework to
these models from 3D Slicer, so Autodesk would
function properly, and the resulting animations
would be able to render at quick speed.
1.3.2.3 Retopology and Sculpting
Once the 3D Slicer models were converted to
usable Maya mesh, they were retopologised to
change the mesh from triangular to quadrilateral
mesh and ensure full Maya functionality in the
modelling and animation editors. See Fig. 1.8 for
retopology and remesh workflow. Automatic
retopology allowed a lower polygon count by
50–75%, which helped maintain a clean Maya
workspace that did not crash. Retopologising
also allowed the model to be sculpted, textured,
and animated effectively using quadrilateral
mesh. All 3D Slicer models were retopologised
after undergoing the Bifrost process.
After the structures were successfully
retopologised, sculpting occurred on the models.
This involved using Maya’s sculpt tools to
smooth and adjust the models. Figure 1.9 shows
the various sculpting tools and a selection of the
models before and after being sculpted in
Autodesk Maya. A similar process was carried
out for the lungs in the TAA application.
1.3.2.4 Modelling of the Heart
The heart was modelled manually in Maya with
anatomical references. As a reference, the 3D
heart model on BioDigital.com was used as this
website is very reliable and is highly noted for its
Fig. 1.6 Fast-Marching lung segmentation
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 9
28.
anatomical accuracy (Qualteret al. 2012). The
model was created in Autodesk Maya, by first
sculpting a primitive cylinder against the refer-
ence images and then extruding a portion of the
mesh for the atriums and extruding the various
blood vessels. The same process was used for
modelling the thoracic aorta and the branch
vessels. The thoracic aorta was manually cut
open in the area of the aneurysm to reveal the
inner layer of the vessel and then subsequently
attached to the abdominal aorta. See Fig. 1.10 for
the untextured model and the polygon mesh of the
heart and aorta.
Fig. 1.7 Bifrost visual framework workflow
10 S. Bakalchuk et al.
29.
1.3.2.5 Modelling ofRelay Endograft
The Relay stent graft was modelled using a pro-
cess of both photogrammetry and manual
retopology. First, multiple photographs of the
stent graft were taken and imported into Agisoft
Metashape for automatic photogrammetry. The
photogrammetry process is illustrated in
Fig. 1.11. Through this process, a rough mesh
was achieved that while unsuitable for automatic
retopologising, contained an accurate representa-
tion of the stent, which was used as a model
reference.
To create the model within Maya, the surface
of the photogrammetry mesh was made live, and
the CV curve tool was used to trace along the
outline of the imported mesh to create an accurate
representation of the springs comprising the struc-
ture of the stent. Once the springs were traced,
duplicated, and aligned, the quad draw tool was
utilised to model the fabric connecting each row
of wires. Figure 1.12 depicts the process of using
the photogrammetry mesh as a reference for cre-
ating the shape of the stent using the Maya
retopology tools, as well as the resulting model
from this process.
1.3.2.6 Modelling of Fenestrated
Anaconda Endograft
Terumo aortic provided a physical Fenestrated
Anaconda stent to reference for modelling a
four-fenestration stent graft (Inchinnan, Scotland,
UK). Measurements of the physical stent were
Fig. 1.8 Remesh and retopology workflow
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 11
30.
taken, and threecylinders created in Maya and
taken into Illustrator and measured using the ruler
tool to ensure accurate model dimensions; this
process is seen in Fig. 1.13.
1.3.2.6.1 Wires and Stitching of Stent Graft
After the stent base mesh was created, the CV
curve tool was used to depict the wires on the
stent. The wires and stitching of the Fenestrated
Anaconda needed to be depicted as rolling curves
Fig. 1.9 (a) Autodesk Maya 2020 Sculpting tools used.
(b) Kidney before and after smoothing. (c) Superior
mesenteric artery before and after smoothing. (d)
Abdominal aortic aneurysm before and after smoothing.
(e) Top aorta before and after smoothing
Fig. 1.10 Final heart mesh for use in animation
12 S. Bakalchuk et al.
31.
that were perfectlysmooth; this was extremely
important to depict as wires that had a slight
bend, or were not perfectly even, could cause
fractures or occlusion in patients. Dimensions
were provided by Terumo Aortic (Fig. 1.14) so
the peaks and valley features were accurately
modelled as well as the wires. The valley and
legs modelled off of the provided dimensions
are seen in Figs. 1.14 and 1.15. Once the stent
body and wires were recreated, stitching was
Fig. 1.11 Stent photogrammetry in Agisoft Metashape. This still depicts the automatic process by which the application
converts a point cloud generated from image data to a polygonal mesh
Fig. 1.12 (a) Process of creating stent based off of photogrammetry mesh. (b) Final untextured model of Relay stent
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 13
32.
applied to themodel. The stitching for the seams
of the stent graft was completed using Maya
Plugin, MASH; the process is seen in Fig. 1.16.
1.3.2.6.2 Stitches and Fine Details of Graft
To replicate the seams, small cylinders, and torus
shapes were added to the stent graft; this can be
seen in Fig. 1.17. These were assigned
aiStandardSurface materials.
1.3.2.6.3 Additional Stent Body Models
Additional models were needed that are used
during stent deployment. Figure 1.18 shows the
Iliac Leg model designed in Autodesk Maya by
creating a cylinder and then selecting every other
edge and inverting the model. Edge loops were
applied on either side of this model to create a
smooth look and allow for colouring of the wire
to be applied to the model.
1.3.2.6.4 Deployment Devices
Deploying the stent required the use of five addi-
tional models which can be found in Fig. 1.19.
These were created on Maya through a series of
modelling and referring to the surgical manual for
FEVAR surgery.
Fig. 1.13 Process of measurements for stent graft starting
with base cylinders
Fig. 1.14 Dimensions provided and resulting modelled peak and valley
Fig. 1.15 Smooth rolling wire curve
14 S. Bakalchuk et al.
33.
1.3.2.7 Texturing inSubstance Painter
The application Substance Painter was used in the
case of the TAA application to paint realistic
textures onto the 3D assets created. For the heart
model, once the mesh was completed, it was
exported into Substance Painter to automatically
unwrap the UVs and paint on various texture
maps with a Wacom tablet. This application was
utilised to paint the texture of the heart muscle
and all of the coronary arteries. Figure 1.20 shows
the painting process, as well as the finished prod-
uct created on substance painter. The resulting
texture maps were then exported into Maya and
attached as bitmaps onto various channels on an
Arnold aiStandard shader material. Figure 1.21
shows a map of the Arnold texture utilised.
The lungs were also exported into Substance
Painter for UV unwrapping and manual genera-
tion of texture maps. An assortment of the
application’s default brush settings was used to
paint a texture onto the surface of the model, as
well as the bump map paint brushes to make the
surface of the lungs appear more realistic. Fig-
ure 1.22 depicts the manual brushwork and tex-
turing performed within Substance Painter and a
Fig. 1.16 MASH process for creating the stent’s stitching
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 15
34.
final rendering ofthe lungs once exported back to
Maya.
Finally, the stent graft was brought into Sub-
stance Painter to add textures and fine details
within the stent. This included stitching, wires
and a number of other important markers featured
on the device. Additionally, a fabric texture was
created for the body of the stent and a metal
texture for the wires. Figure 1.23 depicts the
process of texturing the model within Substance
Painter, as well as the finished product created.
1.3.2.8 Informational Animations
The following headlines outline the methodology
implemented to generate a series of animations to
visualise FEVAR and TEVAR surgical technique
Fig. 1.17 Stitching details: close-up and far away on rolling curve wires
Fig. 1.18 Anaconda™
Iliac Leg (a, b) created
based on the Terumo Iliac
Leg photograph (c)
16 S. Bakalchuk et al.
35.
Fig. 1.19 Deploymentdevices. (a) All deployment
devices together. (b) Iliac Legs used after Fenestrated
Anaconda deployed to connect to associated vessels. (c)
Sheath used for deployment of the stent. (d) Deployment
tube. (e) Deployment wires for guiding the sheath. (f)
Sheath aid tip
Fig. 1.20 Textured heart in Substance Painter: process (a) and final texture map (b)
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 17
36.
for AAA andTAA patients, respectively, and
clinical successes after inserting the stents.
Different animations per stent were produced for
the three modules: deployment, features and clin-
ical performance.
1.3.2.8.1 Animations for the Fenestrated
Anaconda Stent Graft
Manual sculpting and modelling adjustments to
the aorta and associated vessels had to be made
for different animations. The faces on the front
side of the aorta and renal arteries were manually
selected and detached from the main mesh. As a
result, a realistic view of the aorta was created to
allow for femoral access to be visualised.
All of the deployment tools were animated
using the curve warp deformer in Maya. The
deformer firstly allows for objects to be deformed
along a curve path and enables manipulation of
the length scale and offset of the 3D object; this
made animating quite a challenge given the
factors, such as scale, rotation and smoothed
movement, considered when setting key frames.
A lattice and cluster system was used to animate
the deployment and unsheathing of the stent.
Each cluster was animated, and keys set individ-
ually to control scaling, position and rotation of
the stent unsheathing and expanding. A
visualisation of the lattice, clusters and twist han-
dle is seen in Fig. 1.24.
Fig. 1.21 Graph of aiStandard Arnold texture settings
Fig. 1.22 Lung texturing process in Substance Painter and rendering of the textured model in Maya
18 S. Bakalchuk et al.
37.
The proximal accessanimation for the feature
module was created and animated by using the
curve warp deformer. By creating an opaque
stent, the camera was able to zoom in and out of
the stent to show access from the upper aorta and
down into the fenestration. The repositioning ani-
mation required the camera to be animated in
various positions in order to depict a close-up
visualisation of the stent moving, rescaling and
inflating after unsheathing, one of the key com-
petitive features of the Fenestrated Anaconda.
The versatility animation was also created by
animating a camera around the stent to show the
various positions and sizes of the fenestrations
and how they are uncompromised by stents or
wires (Colgan et al. 2018; Dijkstra et al. 2014;
Midy et al. 2017). Figure 1.25 shows resulting
stills from these two animations.
Terumo Aortic required four clinical perfor-
mance statistics about this specific graft to be
showcased in the animations. For this, the Maya
Plugin ‘MASH’ was utilised to animate red blood
cells (RBCs) going through the stents and into the
vessels. This was an easily accessible system to
use and apply changes to animation speed, dis-
tance apart, randomness and rotation. The process
of creating a MASH network for the RBC anima-
tion portion is discussed in more detail below.
1.3.2.8.2 Animations for the Proximal Relay
Stent Graft
The animation process began by animating the
delivery system. To animate the stent lead wire,
a cylinder was created, and the curve warp tool
was utilised to animate the wire moving along a
curve going up the length of the aorta. This was
done so that the wire can be portrayed climbing
through the aorta and into the aortic arch. Next,
the sheath was animated by creating a larger
cylinder that follows the same path of the lead
wire and lands within the aortic arch. This anima-
tion was created by animating the max length of
Fig. 1.23 Texturing the Relay stent in Substance Painter: process and final rendering
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 19
38.
the sheath withthe curve warp deformer and
repeated so that there was both an inner and
outer sheath portrayed. In order to animate the
stent deployment, the curve warp deformer was
utilised to allow the stent to be deployed along the
curve, followed by a flare deformer, which
allowed for the stent to be scaled up as it is
deployed. A separate flare deformer was used
for the top springs of the stent, to portray them
detaching from the tip capture mechanism after
Fig. 1.24 Stent animation
process by lattice, cluster
and twist handle
20 S. Bakalchuk et al.
39.
the stent isfully deployed. After this, the same
curve warp method was used to reverse the direc-
tion of the wires and the sheath comprising the
delivery system, in order to demonstrate how
these components exit the aorta. Figure 1.26
shows the set-up for the delivery system, as well
as the flare deformer and curve warp deformer
settings utilised for this animation.
In order to animate the heart beating, multiple
lattice deformers were used on each part of the
heart in a synchronised loop. This loop made it so
that three different parts of the heart were
expanded and then shrunk in synchrony. Fig-
ure 1.27 portrays the lattice deformers and graph
editor utilised for this animation within Maya.
1.3.2.8.3 Red Blood Cell Flow Animations
To create the animation of the blood cells flowing
through the aorta, the MASH tool was used on the
previously modelled red blood cell to create a
network of particles that flow along
predetermined curves. A CV curve was fashioned
Fig. 1.25 Proximal and repositionable animation stills to visualise the benefit of these custom surgical techniques
Fig. 1.26 Depiction of stent deployment animation process for TAA animations
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 21
40.
for each potentialRBC path, and a corresponding
MASH network for each of the four paths was
created. The paths and the MASH network
settings can be seen in Fig. 1.28. A randomness
node was also added to the MASH settings so that
the rotation and orientation of the cells would be
varied.
1.3.2.8.4 Post Processing
The application Adobe After Effects was used to
compile the multiple series of still images ren-
dered into videos. In order to create the
compositions in After Effects, the rendered PNG
sequence was selected for each video and then
imported as a composition into the software.
Once all of the videos were compiled, various
features of the application were used to add
unique text and graphics.
1.3.2.9 Application Development
1.3.2.9.1 Home Screen
Construction of the home screen required com-
bining three relevant renderings in Photoshop
with a standard background circle provided by
Terumo Aortic to create buttons. These buttons
lead the user to the three main sections of the
applications: features, deployment and clinical
performance. In addition to the home screen
buttons, a number of other custom UI features
were created that appear within the applications.
All of these were designed to fit the Terumo
Aortic graphic style while still remaining intuitive
and simplistic. Figure 1.29 depicts the home
screen for both applications.
Fig. 1.27 Lattice deformers utilised for heart beat animation
Fig. 1.28 MASH network
set-up for TAA blood flow
animations
22 S. Bakalchuk et al.
41.
1.3.2.9.2 Features Section
Tocreate the interactive applications, all the 3D
models required were imported into Unity. These
were all exported as FBX’s with their
corresponding textures and imported into the
features section of the applications. A
corresponding icon was added to a portion of
the model for each feature, and the buttons were
coded so that a specific video would come up
when the user clicked on a feature. Figure 1.30
shows the ‘Features’ unity scene for both
applications with the imported models and cus-
tom UI.
1.3.2.9.3 Clinical Performance
and Deployment Sections
For the clinical performance and deployment
modules, the rendered MP4s and relevant UI
were imported into the scene. The videos were
then placed onto a raw image with a render tex-
ture, so they played seamlessly on the screen.
Simple scripts were added in order to create a
play button, a pause button, and a replay button.
Additionally, a script for a progress bar was cre-
ated with the help of supervisor Dr. Matthieu
Poyade. This feature was created underneath the
video so that the user can track the video progress
and interact with the bar to fast forward or rewind
the video. Figure 1.31 depicts the video interface
created within Unity for both deployment
modules, while Fig. 1.32 depicts the video inter-
face created for both clinical performance
modules.
1.4 Results
1.4.1 Outcomes from Evaluating
the Finished Application
with Clinical Professionals
Following application development, both
products underwent a process of evaluation by
clinical professionals at Terumo to assess their
effectiveness in communicating the key features
of the devices to a broader medical audience. For
Fig. 1.29 Home screen for TAA application (left) and AAA application (right)
Fig. 1.30 Features section of TAA application (left) and AAA application (right)
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 23
42.
the most part,this evaluation process provided
valuable feedback about the effectiveness of
these applications. Both received high ratings
for face validity and content validity across all
three sections of the application. However, it was
reported that the deployment models and
animations within the TAA app could have been
improved. Similarly, the Iliac Leg stent used for
completing the FEVAR technique in the AAA
app could have been improved regarding
modelling and texturing techniques. Additionally,
the blood flow simulations were reported to be
distracting with the texturing of the aorta and red
blood cells. There was an overall consensus that
the applications were easy to use and very intui-
tive to figure out. In general, both applications
effectively communicated the most important
aspects of the device, while the deployment sec-
tion of the TAA and AAA apps could benefit
from a few improvements to enhance its accu-
racy. In the future, an updated version of these
applications could be created that contains a more
detailed and accurate depiction of the stents.
While future testing still needs to be conducted,
these preliminary results offer a valuable starting
point to indicate how these applications will be
received by patients and professionals in the field.
Moreover, the research and methodologies used
to create these scientific animations and
corresponding applications show a useful way of
communicating advanced medical devices
through cutting-edge, intuitive, technological
methods.
1.5 Discussion
The aim of this project was to create two user-
friendly interactive applications with various 3D
visualisations of the two corresponding stent
grafts. These visualisations would demonstrate
to clinicians how these products function and
Fig. 1.31 Deployment section of TAA application (left) and AAA application (right)
Fig. 1.32 Clinical performance section of TAA application (left) and AAA application (right)
24 S. Bakalchuk et al.
43.
aid cardiac patientsto understand the key features
and surgical process of the stent deployment.
1.5.1 Discussion of Development
Process
The development process of these applications
was simplified by the fact that Terumo Aortic
had a clear idea of what information to include
in the applications. The ideation and co-design
process with the company lead to the joint con-
clusion that both apps should be broken down
into three modules: deployment, features and
clinical performance. Once this became clear,
designing the layout of the applications and deter-
mining the required UI and 3D assets came natu-
rally. The data extraction, modelling, animation
and application development each came with
their own limitations. Slicer 3D was utilised
only to segment the medical data, so this was a
fairly quick process. On the other hand, the
modelling, specifically of the stent, was a
prolonged, capricious process due to multiple
factors, including limitations to resources and
time. This was especially challenging because
not only did the structure of the stent have to be
exactly like the Terumo Aortic model, but it also
had to be constructed in a manner that allowed for
it to be animated. However, modelling of the
surrounding anatomy, specifically the heart,
aorta, lungs and kidneys, was an enjoyable and
exciting learning process. The texturing process
for the TAA application was one of the most
rewarding aspects of the whole development pro-
cedure, as the application Substance Painter made
it quite easy to paint hyper realistic and detailed
textures directly onto the models. This was espe-
cially necessary due to the small coronary arteries
in the heart and the many small stiches on the
stent.
The animation process was the most challeng-
ing by far for both applications, particularly the
deployment animations. In the case of the AAA
app, the discovery of a technique to animate the
stent unsheathing provided a successful final out-
come, while the TAA application was slightly
less accurate, as the curved shape of the stent
meant that the aforementioned stent unsheathing
technique would not work. The blood flow
animations were created seamlessly with the
user-friendly and intuitive MASH toolkit within
Maya. For the AAA app specifically, the MASH
network created a nice outcome for the RBCs to
be seen flowing through the Fenestrated Ana-
conda, Advanta V12 Balloon stent and Iliac Leg
stents. In retrospect, this type of project could
have been approached differently given the time
constraints and feedback received. Nonetheless,
the 3D models and animations concluded with a
positive outcome.
Troubleshooting had to occur to produce
Arnold renders that were both high quality and
reflective of the time allocated for rendering.
Difficulties with the lighting and quality of the
rendering versus time to render each frame were
considered, and render sequences were divided
up amongst computers. Rendering was a time-
consuming, but ultimately rewarding, process.
The application creation process was rather
simple on the other hand, as the deployment and
clinical performance scenes consisted mainly of
imported videos. Scripting the video interface
started off reasonably simple as well, as the cod-
ing required for adding a start, stop, and replay
button was fairly minimal. However, the process
of adding the scroll bar was much more difficult.
While more complex, the features scene was quite
intuitive to set up as well. Once all the models
were imported and textured, it was quite simple to
import the rendered videos and integrate them
into the application. The design of the app was a
back-and-forth process with the graphics team at
Terumo, which ended up being quite laborious.
While the creation of these applications was a
very long and difficult process at times, it was
also extremely worthwhile.
1.5.2 Discussion of Application
Feedback
The feedback received for these applications was
predominantly positive, in that most participants
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 25
44.
agreed that themodels were realistic and accurate,
but the delivery system models could have used
some adjustments. The clinical performance ani-
mation and the features animations got mostly
positive feedback, while the feedback for the
deployment animation was more neutral. The
content validity was rated highly for all three
modules of the applications, as participants gen-
erally agreed that the key facts and figures were
communicated effectively. In regard to the
applications as a whole, the participants found
them very easy to use and very informative. It is
important to keep in mind however that the cohort
utilised for testing were all highly skilled
professionals and extremely knowledgeable
concerning this device, more so than the target
audience would be. Therefore, any negative feed-
back received from this group would not neces-
sarily indicate bad results. If there was more time,
it would have been beneficial to test these
applications on more participants, allowing for
more reliable data.
1.5.3 Benefits and Drawbacks
of the Application/3D
Visualisation Technique
In addition to creating a valuable application for
professionals in the surgical device industry, the
methodology used for this application presents a
novel 3D visualisation technique, which uses a
combination of highly realistic anatomical model
creation and simple, intuitive application design.
This innovative methodology can be adapted for
many different uses, within many different fields,
and therefore marks a significant contribution to
the realm of biomedical visualisation. The new
techniques, however, do come with a set of
benefits and drawbacks that must be considered
before adapting this methodology to future
projects. For instance, it was widely stated that
certain aspects of the application could have been
more realistic, most commonly the medical
devices. Additionally, this technique can also be
more time-consuming and expensive than a sim-
pler 2D animation. Thus, there are significant
benefits to such techniques as well. For instance,
the high level of detail and realism provided by a
3D application makes a complicated topic quite
easy to understand and visualise for a broad audi-
ence. Additionally, the integration of these
visualisations within an interactive application
makes the animations widely accessible and
more easily viewed by the subject.
1.5.4 Limitations
The most apparent limitations to this project were
caused by the current COVID-19 pandemic. Most
notably, all work had to be done remotely, and no
work could be conducted which involved meeting
people in person or working with clinicians.
These factors made it so that the time for devel-
opment was limited. For the AAA application
specifically, it was understood that the stent
model would be provided in an OBJ format,
because the Fenestrated Anaconda is a highly
intricate device with key features. Therefore,
these applications were not completed to the full
potential that they would have been if allotted
more time or resources. The lack of time also
made it so that we were unable to recruit as
many participants as originally planned. Overall,
despite all of these shortcomings, a great deal was
learnt about creating intricate models, Autodesk
plugins, animation networks and final renders to
create high-quality animations.
1.5.5 Further Development
There are many ways in which this application
could be advanced. Most notably, the
applications could be further developed to incor-
porate some feedback from the participants.
Regrettably, the time constraints of the project
and COVID-19 precautions meant that testing at
a medical conference could not occur. Fortu-
nately, ample feedback was provided throughout
collaboration by professionals of Terumo Aortic
that ensured anatomical and stent graft accuracy
during the development process. Once more
refined, it could be very beneficial to create
applications such as this for other Terumo
26 S. Bakalchuk et al.
45.
products, so thatthe company can effectively
communicate the key features of their products
to clinicians and patients in a more appealing
way. The lack of engaging visualisations and
medical interactive applications for clinical
specialists, supported in the literature, show an
obvious need for these applications to be shown
to clinicians to positively impact their choices in
treating complex aneurysms.
1.6 Conclusion
Advances in understanding stent graft surgical
techniques have led to the need for interactive
applications to engage healthcare workers so
they can exploit its key features to effectively
broaden the treatable patient population. Overall,
the demonstrated methods in this project were
successful in creating animations for interactive
applications that showcased new features of novel
stent grafts. The series of animations for both the
Fenestrated Anaconda and the Relay device made
up a practical interactive application that works to
inform both the physician and patient of various
surgical device options for treating rare, complex
anatomical aortic aneurysm cases. These in turn
provide resources for the physician to visually
explain the surgical procedure and long-term
benefits to a patient. Subsequently, this improves
the discussion between patient and physician,
providing a deeper understanding and patient-
centred surgical approach in elderly patients
who suffer from aortic aneurysms.
Although these applications require additional
testing, and still have a few areas that necessitate
further refinement, these preliminary results show
a great potential for the creation of an application
that can utilise 3D visualisation techniques to
successfully engage both physicians and patients.
The interaction with a surgical device company to
create the anatomical and surgical models,
textures, animations and final application devel-
opment provides an innovative approach to
visualising surgical processes, generating aware-
ness about medical conditions and facilitating
treatment discussions between the physician and
those with aortic aneurysms. Given the range of
positive interactions, as supported in the litera-
ture, of the general public with emerging
visualisation technologies, the applications cre-
ated provide a valid visualisation tool to engage
clinicians, as well as the general public, about
new medical devices, treatment alternatives, and
research pertaining to healthcare an easily acces-
sible visual format (Baker et al. 2002; Ford and
Leinonen 2009; Traxler 2007). The creation of
these applications also establishes a methodology
for building informative surgical tools and posi-
tively influences the healthcare field through
accurate dissemination and communication of
surgical procedures and associated statistics.
References
Abraha I, Romagnoli C, Montedori A et al (2009) Tho-
racic stent graft versus surgery for thoracic aneurysm.
Cochrane Database Syst Rev 1:Cd006796. https://doi.
org/10.1002/14651858.CD006796.pub2
Alsafi A, Bicknell CD, Rudarakanchana N et al (2014)
Endovascular treatment of thoracic aortic aneurysms
with a short proximal landing zone using scalloped
endografts. J Vasc Surg 60(6):1499–1506
Ashton HA, Scott R, Bridgewater SG (2002) Randomized
clinical trial of screening for abdominal aortic aneurysm
in women. Br J Surg [online] 89(3):283–285
Autodesk, Inc. (2020) Maya. Available at: https:/autodesk.
com/maya
Avishay DM, Reimon JD (2020) Abdominal aortic repair.
In: StatPearls. StatPearls Publishing, Treasure Island,
FL
Baker DW, Gazmararian JA, Williams MV et al (2002)
Functional health literacy and the risk of hospital
admission among Medicare managed care enrollees.
Am J Public Health 92(8):1278–1283
Baker DW, Parker RM, Williams MV et al (1998) Health
literacy and the risk of hospital admission. J Gen Intern
Med 13(12):791–798
Ben Abdallah I, El Batti S, Sapoval M et al (2016) Proxi-
mal scallop in thoracic endovascular aortic aneurysm
repair to overcome neck issues in the arch. Eur J Vasc
Endovasc Surg 51(3):343–349
Bercovich E, Javitt MC (2018) Medical imaging: from
roentgen to the digital revolution, and beyond.
Rambam Maimonides Med J 9(4):e0034
British Heart Foundation (2020) Thoracic aortic
aneurysms–Causes, symptoms & treatments. Accessed
28/05
Brown LC, Powell JT, Thompson SG, Epstein DM,
Sculpher MJ, Greenhalgh RM (2012) The UK
endovascular aneurysm repair (EVAR) trials:
randomised trials of EVAR versus standard therapy.
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 27
46.
Health Technol Assess16:1–218. https://doi.org/10.
3310/hta16090
Bungay PM, Burfitt N, Sritharan K, Muir L, Khan SL, De
Nunzio MC, Lingam K, Huw Davies A (2011) Initial
experience with a new fenestrated stent graft. J Vasc
Surg 54:1832–1838. https://doi.org/10.1016/j.jvs.
2011.05.115
Burt JR, Zimmerman SL, Kamel IR et al (2014)
Myocardial T1 mapping: techniques and potential
applications. Radiographics 34(2):377–395
Coelho-Filho OR, Rickers C, Kwong RY et al (2013) MR
myocardial perfusion imaging. Radiology 266
(3):701–715
Colgan FE, Bungay PM, Burfitt N, Hatrick A, Clarke MJ,
Davies AH, Jenkins M, Gerrard D, Quarmby JW,
Williams R (2018) Operative and 1-year outcomes of
the custom-made fenestrated anaconda aortic stent
graft-a UK multicenter study. Ann Vasc Surg
46:257–264. https://doi.org/10.1016/j.avsg.2017.05.
027
Cosford PA, Leng GC (2007) Screening for abdominal
aortic aneurysm. Cochrane Database Syst Rev:
CD002945. https://doi.org/10.1002/14651858.
CD002945.pub2
De Bruin JL, Baas AF, Buth J, Prinssen M, Verhoeven
ELG, Cuypers PWM, van Sambeek MRHM, Balm R,
Grobbee DE, Blankensteijn JD, DREAM Study Group
(2010) Long-term outcome of open or endovascular
repair of abdominal aortic aneurysm. N Engl J Med
362:1881–1889. https://doi.org/10.1056/
NEJMoa0909499
Dijkstra ML, Tielliu IFJ, Meerwaldt R, Pierie M, van
Brussel J, Schurink GWH, Lardenoye J-W, Zeebregts
CJ (2014) Dutch experience with the fenestrated Ana-
conda endograft for short-neck infrarenal and
juxtarenal abdominal aortic aneurysm repair. J Vasc
Surg 60:301–307. https://doi.org/10.1016/j.jvs.2014.
02.011
Dueck AD, Kucey DS, Johnston KW, Alter D, Laupacis A
(2004) Survival after ruptured abdominal aortic aneu-
rysm: effect of patient, surgeon, and hospital factors. J
Vasc Surg 39:1253–1260. https://doi.org/10.1016/j.
jvs.2004.02.006
Elefteriades JA (2002) Natural history of thoracic aortic
aneurysms: indications for surgery, and surgical versus
nonsurgical risks. Ann Thorac Surg 74(5):S1877–
S1880. Discussion S1892–1878
Fernández-Alonso L, Fernández Alonso S, Martínez
Aguilar E et al (2018) Endovascular treatment of aortic
arch lesions using scalloped Endografts. Vasc
Endovasc Surg 52(1):22–26
Ferrari E, Tozzi P, von Segesser L (2006) Thoracic aorta
emergencies: is the endovascular treatment the new
gold standard? Interact Cardiovasc Thorac Surg
5(6):730–734
Filardo G, Powell JT, Martinez MA-M, Ballard DJ (2015)
Surgery for small asymptomatic abdominal aortic
aneurysms. Cochrane Database Syst Rev
Ford M, Leinonen T (2009) Mobile learning: transforming
the delivery of education and training, pp 195–214
Heikkinen M, Salenius J-P, Auvinen O (2002) Ruptured
abdominal aortic aneurysm in a well-defined geo-
graphic area. J Vasc Surg 36:291–296. https://doi.org/
10.1067/mva.2002.125479
Holliman R, Whitelegg L, Scanlon E, et al. (2009)
Investigating science communication in the informa-
tion age: implications for public engagement and pop-
ular media
Howard DPJ, Banerjee A, Fairhead JF, Handa A, Silver
LE, Rothwell PM (2015) Age-specific incidence, risk
factors and outcome of acute abdominal aortic
aneurysms in a defined population. Br J Surg
102:907–915. https://doi.org/10.1002/bjs.9838
Isselbacher EM (2005) Thoracic and abdominal aortic
aneurysms. Circulation 111(6):816–828
Karmy-Jones R, Jackson N, Long W et al (2009) Current
management of traumatic rupture of the descending
thoracic aorta. Curr Cardiol Rev 5(3):187–195
Kasirajan K, Heffernan D, Langsfeld M (2003) Acute
thoracic aortic trauma: a comparison of endoluminal
stent grafts with open repair and nonoperative manage-
ment. Ann Vasc Surg 17(6):589–595
Kato N, Dake MD, Miller DC et al (1997) Traumatic
thoracic aortic aneurysm: treatment with endovascular
stent-grafts. Radiology 205(3):657–662
Kuivaniemi H, Ryer EJ, Elmore JR, Tromp G (2015)
Understanding the pathogenesis of abdominal aortic
aneurysms. Expert Rev Cardiovasc Ther 13:975–987.
https://doi.org/10.1586/14779072.2015.1074861
Liu J, Ma W, Liu F et al (2007) Study and application of
medical image visualization technology. Springer,
Berlin, Heidelberg, pp 668–677
Midy D, Becquemin J-P, Mialhe C, Frisch N, Martinez R,
Caradu C, EFEFA Research Group (2017) Results of
the French multicentric study of ANACONDATM
fenestrated endografts in the treatment of complex
aortic pathologies (EFEFA Registry). Ann Vasc Surg
43:151–165. https://doi.org/10.1016/j.avsg.2017.03.
171
Park JH, Chung JW, Choo IW, Kim SJ, Lee JY, Han MC
(1996) Fenestrated stent-grafts for preserving visceral
arterial branches in the treatment of abdominal aortic
aneurysms: preliminary experience. J Vasc Interv
Radiol 7(6):819–823. https://doi.org/10.1016/s1051-
0443(96)70854-0. PMID: 8951748
Powell JT, Gotensparre SM, Sweeting MJ, Brown LC,
Fowkes FGR, Thompson SG (2011) Rupture rates of
small abdominal aortic aneurysms: a systematic review
of the literature. Eur J Vasc Endovasc Surg 41(1):2–10
Qualter J, Sculli F, Oliker A et al (2012) The biodigital
human: a web-based 3D platform for medical visuali-
zation and education. Stud Health Technol Inform
173:359–361
Saremi F (2017) Cardiac MR imaging in acute coronary
syndrome: application and image interpretation. Radi-
ology 282(1):17–32
28 S. Bakalchuk et al.
47.
Shaw PM, LoreeJ, Gibbons RC (2020) Abdominal aortic
aneurysm (AAA). In: StatPearls. StatPearls Publishing,
Treasure Island, FL
Taylor AM, Wessels Q (2019) Using technology to engage
the public in biomedical sciences. Adv Exp Med Biol
1171:127–135
Traxler J (2007) Defining, discussing and evaluating
mobile learning: the moving finger writes and having
writ. Int Rev Res Open Distr Learn 8(2):43–47
Vascutek Lmtd (2020) Newmains Avenue, Newmains
Ave, Glasgow, Inchinnan, Renfrew PA4 9RR
Wang LJ, Prabhakar AM, Kwolek CJ (2018) Current
status of the treatment of infrarenal abdominal
aortic aneurysms. Cardiovasc Diagn Ther [online]
8(S1):S191–S199
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 29
48.
Using Confocal Microscopyto Generate
an Accurate Vascular Model for Use
in Patient Education Animation
2
Angela Douglass, Gillian Moffat, and Craig Daly
Abstract
Hypertension is a condition requiring lifelong
medication, where patients often feel well with
or without treatment. Uncontrolled hyperten-
sion, however, can lead to permanent
remodelling processes that occur to the vascu-
lar structure, which are seldom understood by
the public. As a result, a significant burden is
placed on healthcare systems globally as a
result of the effects of hypertension and lack
of adherence to prescribed treatment.
Improving patient education through well-
designed interactive applications and anima-
tion is a known strategy that can improve
adherence rates to medication. In the context
of hypertension, little attention has been given
to helping patients understand the unseen dam-
age that occurs to vessels exposed to high
blood pressure. However, generating an accu-
rate representation of a vessel and the changes
that occur can be challenging. Using micros-
copy data is one way for creating an
anatomically correct model, but this often
needs careful consideration as data cannot be
directly imported. Here we describe methods
for creating an accurate 3D model of a small
artery using confocal microscopy data. This
model can then be animated to demonstrate
the substructures and pathological changes
that occur in hypertensive conditions to better
inform patients about the dangers of uncon-
trolled blood pressure.
Keywords
3D modelling · Animation · Patient education ·
Hypertension · Vascular remodelling
2.1 Introduction
Creating computer-generated 3D anatomical
models for animation or interactive applications
for the purposes of education is often fraught with
challenges. The artist must consider the audience
at which the content will be aimed and tailor the
detail accordingly. It is therefore an important
consideration that the models do not contain an
overwhelming amount of information whilst
retaining scientific accuracy (Schwan and
Papenmeier 2017).
This can prove more difficult when consider-
ing the portrayal of microanatomy and structures
at cellular and subcellular levels (Daly et al.
2014). The viewer must be able to appreciate the
scale at which the objects are being observed.
Furthermore, as many of the small cell structures
are colourless, any colour and texture choices
A. Douglass (*) · C. Daly
School of Life Sciences, College of Medical, Veterinary
Sciences, University of Glasgow, Glasgow, UK
e-mail: Angela.Douglas@glasgow.ac.uk
G. Moffat
School of Simulation and Visualisation, Glasgow School
of Art, The Hub, Glasgow, UK
# The Author(s), under exclusive license to Springer Nature Switzerland AG 2022
P. M. Rea (ed.), Biomedical Visualisation, Advances in Experimental Medicine and Biology 1356,
https://doi.org/10.1007/978-3-030-87779-8_2
31
49.
applied to helpthe viewer interpret the models
must not be misleading (Xiao 2013). It is there-
fore important that during the visual development
phase, a balance is struck between artistic licence
and realism.
There are many strategies available to create
3D models, and with the increasing availability of
cheaper computer power as well as open-source
software, it is now even easier to build models
from 3D datasets generated by scanning equip-
ment (e.g. MRI, PET or CT) (Eid et al. 2017). The
same is true for visualising smaller-scale
structures such as tissues and cells using micros-
copy. Improved spatial and temporal resolution of
acquired images means more accurate and
detailed models can be constructed (Daly et al.
2014). This does not come without its challenges.
The shear complexity of this data requires an
expert eye to help tease out the key information,
and models require significant processing prior to
use in any apps, infographics or animations
(McCrorie et al. 2016).
The composition of any rendered images cre-
ated from 3D models must also be a consider-
ation; clear well-structured images with adequate
dialogue help draw attention to features of interest
and are crucial to delivering key messages to the
viewer. Placing things well and giving suitable
context can enhance comprehension of a difficult
topic and increase audience retention (Schwan
and Papenmeier 2017).
Whilst engaging with individuals for the
purposes of education is valuable, the ability to
change an individual’s behaviour in a positive
manner is ultimately the aim for many patient-
focused animations and infographics (McCrorie
et al. 2016). This is particularly true when consid-
ering hypertension, where lifestyle modifications
and adherence to medication reduce a patient’s
risk of potentially debilitating and life-threatening
complications (Milani et al. 2017).
In this chapter we discuss the creation of a
model of a small artery that can be used to explain
their structure and function in health and under
hypertensive conditions. We focus on how this
model can be used within the context of hyper-
tension to explain the importance of adherence to
medication to patients.
2.2 Blood Pressure
Determining an individual’s blood pressure
involves the measurement of two distinct values,
the systolic and diastolic pressures. The systolic
pressure is the pressure at which the blood arrives
at the arteries after being ejaculated from the
heart. The diastolic pressure measures the pres-
sure during the heart’s refilling period between
beats (Vischer and Burkard 2017).
Blood pressure is categorised into ranges that
correlate with cardiovascular health which varies
with a person’s age and sex (Fig. 2.1) (Unger
et al. 2020). Arteries have a propensity to lose
flexibility and stiffen as a part of the normal aging
process which can elevate blood pressure, mean-
ing pressure varies also depending upon age
(Toda et al. 1980). There is also natural variation
between the sexes as hormones such as oestrogen
influence vascular tone (Wang et al. 2020). This is
particularly notable in the post-menopausal years,
where blood pressure can increase more rapidly in
women than at any other time (Cifkova et al.
2008).
2.3 Blood Pressure Regulation
With the exception of the pulmonary arteries, the
arterial system is responsible for transporting
oxygenated blood from the heart to the tissues
of the body. This network of vessels is highly
responsive to external stimuli and adapt quickly
to changing pressures by contraction and relaxa-
tion of the vessel walls, increasing or decreasing
the luminal diameter. The length of the vessel also
changes as part of this response (Mercadante and
Raja 2020).
The regulation of blood pressure is complex
involving multiple organ systems primarily via
the renin-angiotensin-aldosterone system
(RAAS). It serves as a protective mechanism for
tissues, helping to ensure that damaging high
pressures are kept from the terminal capillaries
within organs by constriction of the small arteries
(Warnert et al. 2016). Arteries vary in their size
and structure depending upon their location.
32 A. Douglass et al.
50.
When blood leavesthe heart, the first artery it
comes into contact with is the aorta (Mercadante
and Raja 2020). This large artery is highly elastic
with a large muscular wall. Despite its size its role
in blood pressure regulation is minimal. Instead, it
is the small- to medium-sized arteries that are of
greatest importance (Delong and Sharma 2019).
These arteries, also known as resistance arteries,
respond to internal stimuli such as transmural
pressure and sheer stress within the vessel from
blood flow but also from stimuli from the sympa-
thetic nervous system via vascular nerves that
form a network throughout the vascular system
(Delong and Sharma 2019).
Hormones via the RAAS also influence blood
vessels to help maintain pressure homeostasis.
Juxtaglomerular cells from the kidney release a
hormone called renin into the blood in response to
a drop in blood pressure (Patel et al. 2017). Renin
acts on the freely circulating angiotensinogen
produced by the liver to form angiotensin
I. Angiotensin I is a weak vasoconstrictor that is
then converted to a potent vasoconstrictor, angio-
tensin II by angiotensin-converting enzyme
(ACE) (Fig. 2.2) (Patel et al. 2017).
The production of angiotensin II also
influences production of aldosterone. This hor-
mone acts on the distal tubules of the nephrons
within the kidney to promote reabsorption of
sodium and water and the excretion of potassium,
which results in an increased blood volume and
increased blood pressure (Elliott 2007).
2.4 Pathophysiology
of Hypertension
Whilst cardiac output is important for generating
the pressure within the arterial system, it is the
resistance of the peripheral arteries that influences
the overall pressure of the arterial blood
(Mercadante and Raja 2020). Blood pressure
varies naturally throughout the day, and short
periods of hypertension in response to acute
stresses are normal. However, prolonged expo-
sure of the vasculature to high pressures becomes
pathogenic and warrants a diagnosis of hyperten-
sion (Brown and Haydock 2000). Hypertension
can be further classified into two groups, either
‘essential’ or ‘primary’ hypertension or
Fig. 2.1 Variation of Mean Systolic and Diastolic Blood
pressure between Males and Females with Age. Blood
pressure increases with age and varies between the sexes
in individuals not receiving antihypertensive medication.
Typically, males have a higher systolic and diastolic
pressures compared with women, however this changes
in the post-menopausal years, where females tend to
exhibit higher average pressures. Image taken from
(Beaney et al. 2018)
2 Using Confocal Microscopy to Generate an Accurate Vascular Model for Use. . . 33
51.
secondary hypertension. Essentialhypertension is
typically diagnosed in 90–95% of cases of hyper-
tension (Brown and Haydock 2000). This relates
to cases where there is not a definitive underlying
cause but can be attributed to a lifestyle or meta-
bolic element. Secondary hypertension is
diagnosed where there is a specific cause, com-
monly a chronic kidney condition, that should be
the focus of any treatment plan (Scala et al. 2008).
The trend of blood pressure increases observed
with age occurs most frequently in western
populations, and it is believed to be related to
factors such as higher sodium intake, lower potas-
sium levels, higher likelihood of obesity, alcohol
consumption and reduced physical activity.
Sodium/potassium imbalance and obesity impact
the regulatory mechanisms of blood pressure,
having a negative impact (Scala et al. 2008).
Uncontrolled high blood pressure causes dam-
age to the small arteries and ultimately has an
impact on multiple organ systems. Most com-
monly, this affects the heart which increases the
risk of myocardial infraction or cardiac failure
(Zhou et al. 2018). There are also implications
for the brain, as high blood pressures can lead to
stroke and vascular dementia (Ben Nasr et al.
2018; Warnert et al. 2016). Hypertension also
has a profound effect on the kidneys. The ability
of the kidneys to filter blood efficiently and
remove waste products is dependent upon main-
tenance of normotensive pressures (Mennuni
et al. 2014). Persistent damage to the kidneys
due to high blood pressures can lead to renal
failure. Other disorders include peripheral artery
disease (PAD), vision loss and sexual dysfunction
(Mennuni et al. 2014).
Also the effects on the body, hypertension also
represents a significant global healthcare burden,
contributing to over 18 million deaths each year.
Around one third of all deaths can be attributed to
hypertension (Unger et al. 2020). Alarmingly,
hypertension is affecting younger individuals,
and incidences globally appear to be increasing
(Luo et al. 2020). In Scotland nearly 50% of all
myocardial infarctions and strokes are linked to
uncontrolled hypertension. The issue is further
compounded when considering as many as 30%
of adults have hypertension with only around half
of those diagnosed and many of those are not in
receipt of effective treatment (‘Scotland Factsheet
fear of heart and circulatory diseases 2020).
2.5 Peripheral Resistance Artery
Structure and Vascular
Remodelling in Hypertension
The anatomy of arteries is related to their function
depending upon what organ they supply and
where they are found. Peripheral resistance
arteries that are predominantly involved in the
regulation of blood pressure have a layered struc-
ture consisting of different cell types (Mercadante
and Raja 2020). The inner most layer is a single
cell surface of endothelial cells that face directly
into the lumen of the vessel. Behind this layer is a
Fig. 2.2 Summary of the renin-angiotensin-aldosterone
system. The renin-aldosterone system is the hormone sys-
tem that plays a primary role in blood pressure as well as
sodium, potassium, and fluid balance within the body
34 A. Douglass et al.
52.
thin elastic lamina,followed by a layer of smooth
muscle cells known as the tunica media (Mulvany
and Aalkjaer 1990). Another elastic lamina
encompasses the media, which is surrounded by
the outer most layer, the adventitia. This layer—
unlike the organised arrangement of cells
observed in the other layers—is made up of a
poorly characterised attachment of elastin and
collagen fibres (Briones et al. 2003). It is also
interspersed with a variety of cell types such as
fibroblasts, macrophages and nerve cells, which
are surrounded by adipose tissue (Mulvany and
Aalkjaer 1990). The cells within these layers can
communicate with each other and respond to
internal and external signals to adapt the vessel
shape in response to changing pressures (Intengan
et al. 1999).
When vessels are exposed to high blood
pressures, even over a relatively short period,
these resistance arteries undergo organisational
and structural changes known as vascular
remodelling (Martinez-Quinones et al. 2018). In
the early stages of remodelling, the number of
cells increases in the adventitial layer, and this is
likely an increase in the number of fibroblasts in
response to proinflammatory signals (Martinez-
Quinones et al. 2018). These cells can then
migrate and differentiate to myofibroblasts further
perpetuating the inflammatory response. The
smooth muscle layer also becomes thickened
resulting in a larger, less flexible artery (Touyz
et al. 2018).
Remodelled arteries have more collagen than
healthy arteries and are less able to adapt to pres-
sure changes. The remodelling process is also not
a reversible one; although some recovery is pos-
sible, long-term exposure to high blood pressure
means that it is unlikely to be undone using med-
ication (Schiffrin 2010).
2.6 Treatment of Hypertension
Medications available to counteract hypertension
are relatively inexpensive and are effective at
lowering blood pressure (Katharina et al. 2004).
When considering a treatment pathway, clinicians
weigh up the risk of a patient’s cardiovascular
risk based on their lifestyle, BMI, age and sex in
combination with multiple blood pressure
measurements, before agreeing an appropriate
course of action, rather than basing any decision
solely on blood pressure measurement (NICE
Guidelines, No 136). In some cases of essential
hypertension, modification of lifestyle may be
successful for lowering blood pressure and should
be provided as an option prior to prescribing
medication (Drevenhorn et al. 2007). Where
blood pressure may be in the hypertensive range
and lifestyle medication is either unsuccessful or
not an option, antihypertensive drugs will be the
first line of defence (Unger et al. 2020).
There is an extensive variety of antihyperten-
sive medications available. Typically more than
one medication will be required, and a process of
trial and error is adopted to find the most suitable
medication, whilst being mindful of other
diseases where there may be a contraindication
(Brown and Haydock 2000).
Most antihypertensive medications can be
categorised into four subtypes depending upon
their mechanism of action and are summarised
in Table 2.1.
In most cases, where suitable, beta-blockers
are used to lower blood pressure as a primary
course of action. These drugs act quickly to
lower cardiac output; however, recent evidence
has suggested that these drugs whilst beneficial
fail to reduce the risk of cardiovascular disease
and do not lower blood pressure as effectively as
other more specific medications (Wiysonge et al.
2012). Angiotensin-converting enzyme inhibitors
(ACEI) have been shown to be effective for low-
ering blood pressure. Drugs within this class pre-
vent the conversion of angiotensin I to
angiotensin II. They also reduce excretion of
water and sodium by the kidneys, increasing
blood volume. These drugs are associated with
mild side effects in around 10% of patients but are
generally considered safe (Li et al. 2014). Angio-
tensin receptor blockers (ARBs) also act on the
renin-angiotensin system and are associated with
less side effects. They have been developed as a
second-generation antihypertensive and are also
used in congestive heart failure and diabetic
nephropathy (Brunner 2007).
2 Using Confocal Microscopy to Generate an Accurate Vascular Model for Use. . . 35
53.
Diuretics are alsoconsidered widely as a front-
line drug to treat hypertension. They work by
binding to the thiazide receptor in the kidney
and influence sodium uptake (Schiffrin 2010).
Calcium channel blockers have a vasodilatory
effect and are also considered a good initial
choice for treatment (Elliott 2007).
2.7 Medication Adherence
Although there is a broad spectrum of
medications available for the treatment of hyper-
tension, and diagnosis is simple and
non-invasive, mortality rates due to the
complications of hypertension remain high
(Poulter et al. 2020). The World Health Organi-
zation (WHO) acknowledges that hypertension is
both the largest preventable and treatable issue
affecting health (Zhou et al. 2018). This is in part
due to an estimated four in seven individuals
being undiagnosed, but also of those who are
diagnosed, it is estimated that 50% fail to adhere
to their medication (Burnier 2017). The reasons
for which are multifactorial and complex but
extensive research in the area has identified a
few common issues. Firstly, patients with hyper-
tension are often asymptomatic, particularly in
the case of essential hypertension, and as the
medications for controlling blood pressure are
lifelong, patients may not have the motivation
nor the understanding of their mechanism of
action to stay committed in the long term
(Gavrilova et al. 2019).
Another compounding factor is the pill burden
placed on patients. Typically, medication for
hypertension is taken daily and rarely requires
one tablet. Patients are also likely to be prescribed
statins to help lower blood cholesterol along with
their medication. Patients taking one medication
daily have a greater success rate at adhering to
their medication in the longer term that those that
are required to take multiple pills (Farrell et al.
2013).
It is also challenging to accurately measure
patient adherence. Often, as patient’s adherence
is assessed based on consulting directly with the
patient, this can be an inaccurate method as
patients were found to either misinterpret their
instructions or failed to remember or genuinely
recall their medication-taking habits (Burnier
2017). The lack of accurate monitoring has led
to false diagnoses of resistant hypertension,
resulting in more medication being prescribed
by GPs or in some cases surgical renal denerva-
tion being carried out (Hyman and Pavlik 2015).
2.8 Patient Education Can Improve
Medication Adherence
The complex nature of non-adherence means it is
unlikely that a one-size-fits-all solution will pres-
ent itself. However, a recent review highlighted
that good patient education that encompasses
treatment and long-term complications in addi-
tion to solid patient engagement is most likely to
be the most successful and cost-effective option
to improve patient outcomes (Roldan et al. 2018).
Table 2.1 Antihypertensive medications categorised into four subgroups based on their mechanism of action
Drug category Mode of action Drug examples
Angiotensin-converting enzyme
(ACE) inhibitors
These drugs target and inhibit angiotensin formation,
preventing its activation
Lisinopril, ramipril
and enalapril
Angiotensin II receptor blockers
(ARBs)
ARBs act directly on angiotensin receptors and block its
action
Valsartan and losartan
Calcium channel blockers Reduce calcium entry and inhibiting cellular
vasoconstrictive responses
Amlodipine and
nifedipine
Diuretics Reduce sodium and water content within blood,
reducing blood volume
Chlorothiazide and
amiloride
Beta-blockers Block the stimulatory effects of adrenaline on the heart,
reducing cardia output
Atenolol and
propranolol
36 A. Douglass et al.
54.
Simple strategies, suchas increasing contact
time with specialist nurses to provide information
and promote healthy lifestyle strategies, have a
positive outcome on the blood pressures of
patients (Hacihasanoǧlu and Gözüm 2011).
Although more patient contact time with
healthcare professionals is effective in improving
adherence rates, an individual’s lack of health
literacy can be a barrier to success (Tavakoly
Sany et al. 2018).
Visual aids are a valuable educational
resource. They can be used to help simplify com-
plex information and can also avoid obstacles
relating to language and cultural differences.
They can also be distributed widely and limit
variability of information between healthcare
providers (Pratt and Searles 2017).
Choosing the appropriate format for visual
learning is also key, and 2D images have been
criticised for not providing the breadth and depth
information when trying to communicate
anatomical structures in a teaching environment.
Information can be lost or misinterpreted
(Ballantyne 2011). With the increase in availabil-
ity of cheap 3D printers, more anatomical
structures are now being created and used within
the context to teach, both for medical students,
and to assist with surgical planning but also for
patient education (Garcia et al. 2018).
3D datasets such as MRI, CT and PET imag-
ing can be used to help generate these models.
Although a degree of skill is required to assemble
models digitally for 3D visualisation or printing,
these models can be highly detailed and accurate
(Xiao 2013). Digital 3D models also do not nec-
essarily need to be reserved for 3D printing;
rather they have wide-ranging applications in ani-
mation and interactive mobile applications. 3D
models do not necessarily need to be confined to
the large anatomical structures (Garcia et al.
2018; Bijani et al. 2020). Microscopy imaging
can also generate 3D datasets that can be used to
create 3D digital models providing more visual
aids to enhance understanding of less frequently
observed micro anatomical details (Daly et al.
2002).
Within the context of hypertensive patients,
little information is available as to whether
improving education can be achieved using 3D
models as teaching tools around hypertension and
vascular remodelling. Furthermore, there are lim-
ited studies on visual strategies to demonstrate the
effects of medication on the arteries.
2.9 Generating Digital 3D Models
Using Confocal Microscopy
In vitro imaging of the small resistance arteries
has long been used for research into hypertension
and cardiovascular disease, allowing the physiol-
ogy of the cellular interactions that regulate nor-
mal vascular conditions to be observed
(Martinez-Quinones et al. 2018). These methods
also provide insights into the processes that occur
during arterial remodelling and the changes
vessels undergo when exposed to high blood
pressures, providing valuable models for explor-
ing the roles of drugs and other biological agents
(Schiffrin 2010).
Florescence-based laser scanning confocal
microscopy is a powerful tool used for imaging
individual cells and their substructures to whole
tissue sections and organoids. The method differs
from conventional light microscopy in that it
eliminates noisy out of focus signals using a
pinhole, giving clearer high-resolution images. It
has the capability to acquire serial optical 2D
image sections allowing for 3D reconstruction of
images (Jonkman and Brown 2015). A light
source in the form of lasers or LEDs is used to
excite fluorophores and label specific cell
structures, which emit light at a known wave-
length, allowing for identification of key
structures or cell types. Images for each
fluorophore channel are captured sequentially
and can be overlayed using imaging software
such as Imaris and ImageJ (Hartig 2013; Gautier
and Ginsberg 2021).
Visualisation of whole vessels is challenging
due to the limited size of the scan area of the
microscope. Multiple images must be generated
which requires complex stitching of the data.
Acquisition of the data is also plagued with tech-
nical challenges such as phototoxicity and
photobleaching, particularly when working with
2 Using Confocal Microscopy to Generate an Accurate Vascular Model for Use. . . 37
This ebook isfor the use of anyone anywhere in the United States
and most other parts of the world at no cost and with almost no
restrictions whatsoever. You may copy it, give it away or re-use it
under the terms of the Project Gutenberg License included with this
ebook or online at www.gutenberg.org. If you are not located in the
United States, you will have to check the laws of the country where
you are located before using this eBook.
Title: Nenä
Author: Nikolai Vasilevich Gogol
Release date: July 4, 2016 [eBook #52496]
Language: Finnish
Credits: Produced by Tapio Riikonen
*** START OF THE PROJECT GUTENBERG EBOOK NENÄ ***
61.
Produced by TapioRiikonen
NENÄ
Kirj.
Nikolai Gogol
Suomennos,
Helsingissä, K. E. Holm'in kustantama, 1883.
Suomalaisen Kirjallisuuden Seuran kirjapainossa.
62.
I.
Huhtikuun 25 päivänäoli Pietarissa harvinaisen kummallinen tapaus.
Kotonaan Vosnesenskoi kadun varrella heräsi eräänä aamuna
jokseenkin varhain kuuman leivän hajusta parturi Ivan Jakovlevits
(hänen sukunimensä on unohtunut); eipä katutaulussakaan ole
muuta kuin saippualeukaisen hevosmiehen kuva ynnä kirjoitus:
"myöskin lasketaan verta". Kohotettuaan hiukan päätään huomasi
hän, että hänen kahville harras vaimonsa — arvoisa rouva — otti
juuri uunista paistuneita leipiä.
"Tänään en minä, Praskovja Osipovna, huoli kahvista laisinkaan",
sanoi Ivan Jakovlevits. "Minun mieleni tekee sen sijaan kuumaa
leipää sipulin kanssa." (Se on: Ivan Jakovlevits olisi kyllä tahtonut
molempia, mutta hän tiesi, että oli aivan mahdoton vaatia kahta
asiaa yht'aikaa, sillä Praskovja Osipovna ei voinut laisinkaan
semmoista kärsiä.)
"Antaa hänen hullun syödä leipää; eipä minulle sitä tarvis ole",
ajatteli vaimo itsekseen, "jääpihän minulle kahvia sen enemmän", ja
heitti yhden leivän pöydälle.
63.
Säädyllisyyden vuoksi vetiIvan Jakovlevits, paitasillaan kun oli,
hännystakin ylleen ja istahdettuaan pöydän ääreen, riputti leivälle
suoloja, toi kaksi sipulin pumppua, otti veitsen käteensä ja rupesi
totisen näköisenä leikkaamaan leipää. Jaettuaan leivän kahteen
puoliskoon, katsahtaa hän sen keskustaa — ja kummastuksekseen
huomaa jotain valkeata. Ivan Jakovlevits kaivoi vähän veitsen
kärjellä, koetti sormellaan: "Sitkeätä!" sanot hän itsekseen. "Mitähän
tuo lienee?" Hän pisti sormensa, veti ulos — nenä! — — Ivan
Jakovlevits laski kätensä, hieroi silmiään, koetti uudestaan: "nenä,
totta tosiaan!" Näyttipä se tutultakin. Kauhu ilmaantui Ivan
Jakovlevitsin kasvoille. Tämä kauhu ei kumminkaan ollut mitään sen
kiukun rinnalla, mikä hänen vaimonsa valloitti.
"Keltä sinä, peto, nenän olet leikannut?" tiuskasi tämä
vimmoissaan. "Lurjus, juoppo! Mimmoinen rosvo! Johan minä
kolmelta ihmiseltä olen kuullut, että sinä partaa ajellessasi häärit
nenän ympärillä tuskin kärsittävällä ahneudella."
Ivan Jakovlevits ei enää ollut elossa, eikä kuollutkaan. Hän oli
tullut siihen päätökseen, ettei tämä nenä ollut kenenkään muun kuin
kollegi-assessorin Kovalev'in nenä, jonka partaa hän ajeli joka
sunnuntaina ja keskiviikkona.
"Kuules, Praskovja Osipovna! Minä panen tämän nenän rievun
sisään ja asetan tuonne nurkkaan; antaa sen loikoa siellä vähän
aikaa. Kyllä minä sitten sen korjaan."
"En tahdo kuulla siitä puhuttavankaan! Minäkö antaisin huoneessa
olla leikatun nenän?… Kuivunut raato! Osaat vaan partaveistä
hihnaan hivuttaa, mutta tulet pian kykenemättömäksi koko virkaasi
toimittamaan, heittiö, kelvoton! Että minä sitten saisin sinun tähtesi
64.
oikeudessa vastata?… Viepois se täältä, pois! Vie minne tahansa,
ett'en minä tietäisi haisuakaan siitä! Likaturpa, aasi!"
Ivan Jakovlevits seisoi kuin halolla päähän lyötynä. Tuumaili,
ajatteli — eikä tiennyt mitä ajatella.
"Hiisi sen tietää, miten tässä on käynyt", mutisi hän viimein
kaapaisten kädellään korvantaustaa, "lienenkö minä ollut humalassa,
vai enkö, sitä en totta tosiaan voi varmaan sanoa. Siltä näyttää, että
tässä on jotain tavatonta. Sillä leipä — siinä ei mitään sen
kummempaa, vaan nenä — siinäpä arvoitus. En, en käsitä
laisinkaan!" Ivan Jakovlevits vaikeni. Ajatus, että poliisi ehkä löytää
häneltä nenän, todistaa hänet syylliseksi, saattoi miehen aivot
sekasin, hänen silmiinsä haamoitti jo somasti hopealla koristettu
kaulus, miekka… ja hän vapisi kiireestä kantapäähän. Vihdoin
viimeinkin sai hän käsiinsä alusvaatteensa, saappaansa, puki ylleen
kaiken tuon "joutavan" ja Praskovja Osipovnan tuskastuttavien
saarnojen saattamana läksi kadulle riepuun kääritty nenä kourassa.
Hän tahtoi pistää sen jonnekkin kenenkään huomaamatta: joko
portin patsaan juurelle tahi jollain tapaa muka vahingossa pudottaa
sen kadulle, samalla suikahtaen itse syrjäkadulle. Kaikeksi
onnettomuudeksi sattui vastaan tulemaan joku tuttava, kysellen:
"Minne menet?" tahi "Kenen partaa näin varhain ajelemaan?" niin
ett'ei Ivan Jakovlevits mitenkään saanut sopivaa hetkeä. Jopa hän
kerran pudottikin nenän maahan, mutta kaukaa jo osoitti eräs vartija
kepillään hänelle, älähtäen: "Nosta ylös, sinä pudotit jotain!" ja Ivan
Jakovlevitsin täytyi kuin täytyikin nostaa nenä maasta ja pistää
uudestaan taskuunsa. Hän vaipui yhä suurempaan epätoivoon, koska
ihmisiä rupesi yhä enemmän vilisemään kadulla sen mukaan kuin
makasinit ja puodit avattiin.
65.
Hän päätti mennäIisakin sillalle tuumaellen eikö hänen sieltä
onnistuisi jollakin viekkaudella pudottaa se Nevaan… Mutta
ansaitsenpa moitetta siitä, etten tähän saakka ole virkkanut mitään
Ivan Jakovlevitsista, tuosta monessa suhteessa arvoisasta miehestä.
Ivan Jakovlevits oli, niinkuin kaikki jollaiset venäläiset käsityöläiset,
kauhea juoppo, ja vaikka hän ajelikin joka päivä muitten leukoja, oli
hänen omansa aina ajelematonna. Hännystakki oli hänellä (Ivan
Jakovlevits ei pitänyt koskaan yllään päällystakkia) kirjava, toisin
sanoen se kyllä oli musta, mutta täynnä tummankeltaisia ja harmaita
pilkkuja; kaulus kiiltävä; vaan kolmen napin sijalla rippuivat
ainoastaan rihmat. Ivan Jakovlevits oli oikea syynikkiläinen, ja kuu
kollegi-assessori Kovalev tapansa mukaan partaa ajeltaessa hänelle
sanoi: "Sinun kätesi, Ivan Jakovlevits, haisahtavat jollekin!" niin Ivan
Jakovlevits vastasi kysymykseen: "Millepä ne haisahtaisivat?" "En
tiedä, veikkonen, mutta haisevatpa vaan", sanoi kollegi-assessori, ja
Ivan Jakovlevits, nuuskaa otettuaan, saippuoitti häneltä palkaksi
tästä leuan ja ylähuulen, korvantaustan ja leuanaluksen, sanalla
sanoen — mistä häntä vaan halutti.
Olipa tämä arvoisa porvari jo Iisakin sillalla. Hän katsahti ensin
ympärilleen, kumartui käsipuun ylitse muka tirkistääkseen sillan alle
tokko siellä paljo kaloja uiskenteli, ja pudotti varovasti rievun nenän
kanssa. Hänestä tuntui ikäänkuin kymmenen puntaa olisi harteilta
vierähtänyt: Ivan Jakovlevits oikein naurahti. Sen sijaan, että olisi
virkamiesten leukoja mennyt ajelemaan, käänsi hän askeleensa
laitokseen, jonka oven päällä oli sanat: "Syötävää ja teetä",
pyytääkseen lasillisen totia, kun hän äkkiä hoksasi sillan päässä
seisovan, ylevän näköisen kvartaalin-tarkastajan [korkeampi
poliisivirkamies] leveine poskipartoineen, kolmikulmaisine hattuineen
66.
ja miekkoineen. Hänjähmettyi; samassa tarkastaja viittasi hänelle
sormellaan ja lausui: "Tuleppas tänne, ystäväni!"
Ivan Jakovlevits tunsi puvun ja, otettuaan jo kauempana patalakin
päästään, astui varovasti hänen luokseen lausuen: "Olkaa terveenä,
teidän ylhäisyytenne!"
"Oi, ei tässä ole puhe, veikkonen, ylhäisyydestä — sanoppas, mitä
sinä teit tuolla sillalla?"
"Jumal'avita, herra, kävin partoja ajelemassa ja katsahdin vaan,
juokseeko virta kovasti."
"Valehtelet, valehtelet! Etpä sillä pääse. Vastaappas vaan."
"Minä olen valmis ajelemaan teidän armollisuutenne partaa
kahdesti, vaikkapa kolmesti viikossa vastustelematta", vastasi Ivan
Jakovlevits.
"Äläppäs nyt, veikkonen! Ne ovat loruja vaan. Minulla on kolme
parranajajaa ennestään, ja pitävätpä sitä suurena kunnianaankin.
Mutta sanoppas nyt vaan, mitä sinä siellä teit?"
Ivan Jakovlevits vaaleni… Tähän haihtui kokonaan tapausten
juoksu hämärään, eikä ole mitään tietoa siitä, kuinka sitten kävi.
67.
II.
Kollegi-assessori Kovalev heräsijotensakin varhain ja päästi
huuliltaan äänen örrr!… jonka hän aina teki herätessään, voimatta
itsekään selittää minkätähden. Hän nousi istualleen, käski tuoda
itselleen pienen, pöydällä seisovan peilin. Hän tahtoi katsoa
näpykkää, joka eilisiltana oli noussut hänen nenälleen; mutta
suurimmaksi kummastuksekseen huomaa hän, että nenän sijalla on
ihan tasainen paikka! Säikähtyneenä käski Kovalev tuoda itselleen
vettä ja hieroi pyyhinliinalla silmiänsä: "totta tosiaan, ei ole nenää
laisinkaan!" Hän rupesi hapuroimaan käsillään tullakseen
vakuutetuksi, ett'ei hän nähnyt unta; näyttää siltä, kuin hän
todellakin olisi valveilla! Kollegi-assessori hyppäsi vuoteeltaan,
kaappasi kädellään — ei ole nenää!… Hän käski heti paikalla tuoda
vaatteensa ja läksi kiireimmiten ylipoliisimestarille.
Sillä välin täytyy puhua hiukan Kovalev'ista, jotta lukija voisi
nähdä, mitä lajia tämä kollegi-assessori oikeastaan oli. KoIlegi-
assessoreja, jotka tiedoillaan tämän arvonimen hankkivat, ei saa
laisinkaan verrata niihin kollegi-assessoreihin, jotta siksi tulivat
Kaukasossa. Nämät ovat kaksi aivan eri lajia. Oppineet kollegi-
assessorit… Tämä Venäjä on kumminkin sellainen kummallinen maa,
että jos sanot jotain yhdestä kollegi-assessorista, niin kaikki kollegi-
68.
assessorit Riiasta Kamtschatkaansaakka ottavat sen itseensä; se
tietääkin kaikista nimityksistä ja arvonimistä. Kovalev oli
kaukaasialainen kollegi-assessori. Hänellä oli tämä arvonimi ollut
vasta kaksi vuotta; sentähden hän ei voinut sitä hetkeksikään
unhottaa; mutta lisätäkseen kiitollisuuden tunnetta itseensä, hän ei
koskaan kollegi-assessoriksi itseään nimittänyt, vaan aina majuriksi.
"Kuuleppas eukkoseni", puhui hän tavallisesti kohdatessaan
kadulla muijan, jolla maniskoja oli kaupan, "tuleppas luokseni kotiini;
asuntoni on Sadovoi-kadun varrella, kysy vaan: asuuko täällä majuri
Kovalev, niin sinulle näyttää sen kuka tahansa." Jos hän taas kohtasi
jonkun kaunottaren, niin antoi hän sen lisäksi salaisen viittauksen,
lisäten: "Kysy vaan, kaunokaiseni, majuri Kovalev'in kortteeria."
Tämänpä tähden mekin rupeamme tästä lähtien tätä kollegi-
assessoria majuriksi nimittämään.
Majuri Kovalev'illa oli tapana kävellä joka päivä Nevskin
prospektilla. Hänen maniskansa kaulus oli aina erinomaisen puhdas
ja kiiltävät. Poskiparrat olivat hänellä semmoiset, jommoisia nytkin
saa nähdä läänin- ja piirikunnanmaamittareilla, arkkitekteillä ja
rykmentin lääkäreillä, samoin kaikellaisilla virkamiehillä ja ylimalkaan
kaikilla miehillä, joilla on pulleat punaset posket ja jotka erittäin
hyvin pelaavat "bostonia"; nämä poskiparrat menevät poskien
keskitse suoraan nenään asti, Majurilla riippui kellon perissä suuri
tukku karneooli-sinettejä, vaakunoita ja semmoisia, joihin oli
piirretty: keskiviikko, tuorstai, maanantai y.m. Majuri Kovalev oli
tullut Pietariin asioille, suoraan sanoen — etsimään itselleen sopivata
paikkaa: jos onnistuisi niin vaikkapa virkaatoimittavan kuvernörin,
joll'ei — tuomarin virkaa, jossain näkyvämmässä piirikunnassa. Eipä
majurilla ollut mitään naimisiin menoakaan vastaan, mutta
ainoastaan sillä ehdolla, että morsianta seuraisi kolme sataa tuhatta
69.
ruplaa myötäjäisiä. Tästäpälukija voi itse päättää mimmoinen oli
tämän majurin tila, kun hän huomasi jotensakin kovan ja
säännöllisen nenänsä sijassa tasaisen, sileän syvennyksen.
Ikäänkuin onnettomuudeksi ei näkynyt kadulla yhtään vosikkaa ja
hänen täytyi, kietouduttuansa päällysnuttuunsa, peitettyään
kasvonsa liinalla, mennä jalkasin, teeskennellen, että hänen nenänsä
vuosi verta. "Mutta jospa se näytti vaan minusta siltä; ei se voi olla
mahdollista, että nenä omin päinsä katoaisi", ajatteli hän, astuen
tahallaan kahvilaan katsoakseen peiliin. Onneksi ei kahvilassa ollut
ketään; pojat lakasivat lattioita ja asettelivat tuoleja paikoilleen;
muutamat kantoivat silmät unisina tarjottimilla kuumia piirakoita;
pöydillä ja tuoleilla levisivät siellä täällä eiliset kahvilla valetut
sanomalehdet. "No Jumalan kiitos, ei ole ketään", mutisi Kovalev,
"nytpä saapi tarkastella". Hän meni peläten peilin luo ja katsahti:
"Piru vieköön, tämä on hävytöntä", lausui hän sylkäisten; "vaikkapa
edes jotain olisi nenän sijalla, vaan kun siinä ei ole mitään!"
Harmistuneena huulta purren läksi hän kahvilasta ja päätti vasten
tavallisuutta olla keneenkään katsomatta ja kellekään hymyilemättä.
Äkkiä jäi hän aivan kuin naulatuksi seisomaan erään talon ovelle;
hänen kasvoissaan liikkui selittämätön asia: käytävän eteen
seisattuivat umpivaunut; ovi aukeni ja ulos hyppäsi kyyryselkäinen
herra virkanutussa ja juoksi rappuja ylös. Kuinka suuri Kovalevin
kauhu ja hämmästys oli, kun hän hoksasi, että tuo oli — juuri hänen
nenänsä! Tämän tavattoman seikan tähden huomasi hän silmänsä
pimenevän; päättipä kumminkin, vavisten niinkuin haavanlehti,
odottaa, käyköön sitten miten tahansa, kunnes tuo palaisi
vaunuihinsa. Parin minutin päästä nenä todella palasikin. Hänellä oli
yllä kullalla koristettu, pystykauluksinen virkatakki, jalassa
säämyskäiset roimahousut, miekka vyöllä. Töyhtöhatusta oli helppo
70.
huomata, että hänelläoli valtioneuvoksen arvo. Kaikesta saattoi
päättää, että hän aikoi juuri aamutervehdykselle. Hän katseli
kummallekin puolelle, huudahti ajurille: "Annas tänne!" astui
vaunuihin ja läksi.
Onneton Kovalev oli vähällä menettää järkensä. Hän ei tiennyt
mitä hänen oli ajatteleminenkaan moisen tapauksen johdosta.
Mitenkä se totta tosiaan olikaan mahdollista, että nenä, joka eilen
vielä oli hänellä tuossa poskien välissä, ei voinut ajaa, eikä kävellä,
nyt oli saanut virkatakin yllensä! Hän juoksi vaunujen jälestä, jotka
onneksi eivät vierineetkään kauas, vaan seisattuivat Gostinnoi dvor'in
eteen [oikeastaan vieraspiha; suuri ryhmä makasiineja ja
kauppapuoteja]. Hän juoksi sinne, tunkeutui läpi joukon kerjääjä-
ämmiä, joitten kasvot olivat peitetyt hunnuilla, mihin vaan silmiä
varten oli kaksi aukkoa jätetty, tuon joukon, jota hän ennen niin
kovasti oli pilkannut. Kansaa ei ollut paljo. Kovalev huomasi olevansa
niin suuresti hämmennyksissään, ett'ei hän kyennyt vakavasti
aprikoimaankaan, ja etsi silmillään tuota herraa joka taholta. Vihdoin
äkkäsi hän hänen seisovan erään puodin edessä. Nenän kasvot olivat
kokonaan pystykauluksen takana piilossa, ja hän katseli syviin
ajatuksiin vaipuneena jotakin esinettä.
"Kuinkahan minä lähenisin häntä?" arveli Kovalev. "Kaikesta —
virkanutusta, hatusta — näkyy, että hän on valtioneuvos. Piru ties
miten tässä on tehtävä!"
Hän alkoi yskiä hänen takanaan; mutta nenä ei vaan muuttanut
hetkeksikään asentoansa.
"Armollinen herra", sanoi Kovalev sisällisesti pakoittaen itseään
rohkeuteen, "armollinen herra…"
71.
"Mitä tahdotte?" sanoinenä kääntyen.
"Minua kummastuttaa, armollinen herra… minusta näyttää. Teidän
pitäisi tietää oma paikkanne. Ja nyt minä löydän teidät… missä?…
Ajatelkaahan…"
"Suokaa anteeksi, minä en käsitä mistä te puhutte", lausui nenä.
"Selittäkää asianne!"
"Mitenkä minä hänelle selittäisin!" ajatteli Kovalev ja, rohkaisten
itsensä, alkoi: "Tosin kyllä, minä… muuten, minä olen majuri.
Myönnättehän, etten minä mitenkään saata ilman nenää olla. Joku
tuommoinen kaupittelija-akka, joka Vosnesenskoi-sillan luona
puhdistettuja appelsiineja myypi, voi kyllä istua nenätönnä; mutta
kun ottaa huomioon, että… sitä paitsi, ollessani tuttava useissa
paikoissa naisten kanssa: Tschehtirev'in, valtaneuvoksen rouvan, ja
muitten…. Päättäkää itse… minä en tiedä armollinen herra (tämän
sanottuaan Kovalev kohotti hartioitaan) suokaa anteeksi… jos tämä
soveltuu velvollisuuden ja kunnian lakeihin… Te voitte itse
ymmärtää…"
"En totta tosiaan ymmärrä sanaakaan", vastasi nenä. "Selittäkää
paremmin."
"Armollinen herra", sanoi Kovalev, muistaen oman arvonsa, "minä
en tiedä kuinka minä ymmärtäisin teidän sananne. Tässä on,
luullakseni, koko asia aivan selvä… Vai tahdotteko te…? Olettehan te
— minun oma nenäni!"
Nenä katsahti majuriin, ja hänen kulmansa rypistyivät.
72.
"Te erehdytte, arvoisaherra: minä olen aivan erityinen henkilö.
Muuten meidän välillämme ei voi olla mitään lähempää yhteyttä.
Teidän virkaatekevän nuttunne napeista päättäen kuulutte te aivan
toiseen säätyyn." Tämän sanottuaan käänsi nenä selkänsä.
Kovalev hämmentyi kokonaan tietämättä mitä tehdä ja mitä
ajatellakaan. Silloinpa kuului miellyttävä naisvaatteiden sohina:
lähestyi ijäkäs nainen, kiireestä kantapäähän pitseillä koristettu, ja
hänen perässään solakka neitonen erittäin miellyttävästi pukeutunut
valkeihin varrenmukaisiin vaatteisin, päässä keltanen hattu, keveä
kuin voileipä. Heidän taakseen seisattui, nuuskarasiaansa avaten,
pitkä heitukka pitkine poskipartoineen, kaulassa koko tusina
kauluksia.
Kovalev astui lähemmäs, veti esiin maniskansa patisti-kauluksen,
korjasi kiiltävissä perissä rippuvat sinetit ja hymy huulilla vilkuen
kummallekin puolelle, käänsi koko huomionsa tuohon hentoon
naiseen, joka keväisen kukan keveydellä nyykäytteli päätään ja vei
otsalleen valkean, melkein läpinäkyvän kätensä. Hymy Kovalev'in
kasvoissa tuli yhä suuremmaksi, kun hän hatun alta näki ympyriäisen
loistavan valkean leuan ja osan poskea kevään ensiruusun
varjostamana; mutta äkkiä hypähti hän taaksepäin ikäänkuin olisi
polttanut itsensä. Hänelle johtui mieleen, ettei hänellä nenän sijalla
ollut mitään, ja kyyneleet vierivät hänen silmistään. Hän kääntyi heti
toisaalle, sanoakseen tuolle herralle virkatakissa, että hän vaan oli
tekeytynyt valtioneuvokseksi, ettei hän ollut muu, kuin lurjus ja
hunsvotti, ja ettei hän ollut mikään muu kuin hänen oma nenänsä…
Mutta nenää ei enää löytynytkään; hän ennätti ajaa tiehensä,
varmaankin jollekin aamutervehdykselle.
73.
Tämä saattoi Kovalev'inepätoivoon. Hän läksi takasin ja seisattui
hetkeksi pylväsrivin alle huolellisesti katsellen joka taholle, eikö
sattuisi jostain nenä tulemaan. Hän muisti aivan hyvin, että sillä oli
töyhtöhattu päässä, kullalla ommeltu virkatakki yllä, mutta hänen
päällysnuttuaan ei hän muistanut huomanneensa, ei hänen
vaunujensa väriä, ei hevosta, eikä edes sitäkään, oliko hänellä
vaunujen takana lakeija, ja millaisessa puvussa. Sitä paitsi kulki
vaunuja niin paljo edestakasin ja semmoisella vauhdilla, että oli
vaikea eroittaa niitä toisistaankin; vaikkapa hän sitten olisi
merkinnytkin jonkun niistä, ei hänellä ollut mitään keinoa saada niitä
seisattumaan. Päivä oli ihana ja lämmin. Nevskillä pilveili ihmisiä;
naisia kihisi, niinkuin vesipisaroita kukkasruiskun hanikasta.
Poliisikamarin kohdalta aina Anitschkin'in sillalle saakka. Tuossapa
tulee hänen tuttavansa hovineuvoskin, jota hän överstiksi nimitti,
erittäinkin jos syrjäläisiä sattui läsnä olemaan. Tuollapa Jarjigin,
sekin hänen hyvä ystävänsä, joka bostonia pelatessa aina menetti
kun kahdeksan henkeä oli osaa ottamassa. Kah! toinen majuri, joka
Kaukasossa assessoriksi oli tullut, viittilöipi häntä kädellään luokseen.
"Piru vieköön!" mutisi Kovalev. "Vosikka hoi! Ajappas suoraan
poliisimestarille!"
Kovalev istuutui troskaan ja yhtämittaa huudahteli ajajalle: "Anna
luisua!"
"Onko poliisimestari kotona?" kysyi hän, astuttuaan etehiseen.
"Ei ole, herra", vastasi ovenvartija, "vast'ikään läksi hän kotoa."
"Sepä kaunista!"
74.
"Niin", lisäsi ovenvartija,"ei siitä paljon aikaa ole, mutta
mennythän vaan onpi; jospa olisitte hiukkasta ennen tulleet, niin
olisitte ehkä tavanneet hänet kotona."
Ottamatta vaatetta kasvoiltaan, astui Kovalev takasin vosikalle ja
huudahti epätoivon äänellä: "Anna mennä!"
"Minne?" sanoi vosikka.
"Suoraan eteenpäin."
"Mitenkä suoraan eteenpäin? Tässä on käännös oikeaan tahi
vasempaan?"
Tuo kysymys seisotti Kovalev'in ja pakoitti hänet taas
ajattelemaan. Oikeastaan olisi hänen nyt pitänyt muitta mutkitta
kysyä neuvoa järjestys-toimistosta, ei suinkaan sentähden, eikä sillä
on suoranaista tekemistä poliisin kanssa, vaan siitä syystä, että sen
toimet saattoivat olla paljoa nopeampia kuin muitten; suoraa
ajattelemattomuutta olisi ollut mennä etsimään korvausta sen paikan
esimiehiltä, jossa nenä näkyi palvelevan, sillä nenän omista sanoista
oli helppo päättää, ett'ei sille miehelle mikään pyhää ollut ja että hän
siellä voi valehdella samoin kuin hän valehteli vakuuttaessaan, ett'ei
hän ollut häntä koskaan nähnytkään.
Jopa Kovalev oli käskeä ajamaan järjestys-toimistoon, kun hänelle
johtui mieleen, että tuo lurjus, ilkiö, joka ensi kerran kohdatessa
käyttäytyi niin hävyttömällä tavalla, voisi käyttää aikaa hyödykseen
ja suilahtaa kaupungista — ja silloin tulisivat kaikki etsimiset turhiksi
tahi kestäisivät — Jumala sen estäköön — ehkä kokonaisen
kuukauden. Vihdoin näytti ikäänkuin itse taivas olisi tullut hänelle
avuksi. Hän päätti lähteä suoraan sanomalehti-toimistoon ja ajoissa
75.
ilmoittaa hänen ominaisuutensa,että kuka tahansa, joka nenän
kohtaisi, heti paikalla voisi hänet hänelle toimittaa, taikka ainakin
ilmaista missä nenä oleskeli. Niinpä hän nyt, tämän päätettyään,
käski vosikan ajaa sanomalehti-toimistoon, koko matkan yhtä mittaa
kolhien häntä nyrkillään selkään ja äännähdellen: "Pikemmin lurjus,
pikemmin tolvana!"
"Voi teitä, herra!" sanoi vosikka ravistaen päätään ja lyöden
ohjaksilla hevostaan, jolla oli yhtä pitkä karva kuin katurakilla.
Ruoska seisattui viimein ja Kovalev juoksi hengästyneenä pieneen
vastaanotto-huoneesen, jossa harmaapäinen virkamies, vanha
hännystakki yllä, silmälasit silmillä, istui pöydän takana ja kynä
hampaissa luki vasta tuotuja vaskitahoja. "Kuka täällä ottaa
ilmoituksia vastaan", huusi Kovalev, "hyvää huomenta!"
"Terve tullut", sanoi virkamies kohottaen hetkeksi silmänsä ja
laskien ne takasin vieretysten asetettuihin vaskiraharöykkiöihin.
"Minä tahdon painattaa…"
"Sallikaa, pyydän hiukan odottamaan", lausui virkamies, kirjoittaen
yhdellä kädellään numeroja paperille ja muuttaen vasemman käden
sormilla helmilaudassa kaksi helmeä vasemmalle. Lakeija
nauhuksineen ja puvussa, josta voi päättää hänen palvelevan jossain
ylimysperheessä, seisoi kirje kädessä pöydän luona ja rupesi
näyttämään omaa arvostelukykyään lausuen:
"Uskotteko, herra, ett'ei koira maksa kahdeksaa riunaa [10
kopekkaa], se on minä en siitä maksaisi kahdeksaa rossaa [1/2
kopekkaa], mutta kreivitär, Jumal'aut', rakastaa sitä — senpätähden
se, joka sen löytää, saa sata ruplaa! Totta tosiaan, niin aivan kuin
me tässä, ovat ihmisten maut erilaiset; jos kerran olet koirien ihailija,
76.
Welcome to ourwebsite – the perfect destination for book lovers and
knowledge seekers. We believe that every book holds a new world,
offering opportunities for learning, discovery, and personal growth.
That’s why we are dedicated to bringing you a diverse collection of
books, ranging from classic literature and specialized publications to
self-development guides and children's books.
More than just a book-buying platform, we strive to be a bridge
connecting you with timeless cultural and intellectual values. With an
elegant, user-friendly interface and a smart search system, you can
quickly find the books that best suit your interests. Additionally,
our special promotions and home delivery services help you save time
and fully enjoy the joy of reading.
Join us on a journey of knowledge exploration, passion nurturing, and
personal growth every day!
ebookbell.com





















![The main advantages of the endovascular pro-
cedure include shorter time and lower operative
risk. If the patient is not affected by other high-
priority life-threatening injuries, endovascular
repair should be performed first before any other
surgical treatment in order to eliminate the risk of
sudden aortic rupture (Ferrari et al. 2006). Another
benefit of this surgical technique is the absence of
cardiopulmonary bypass and the low-dose sys-
temic heparinisation (Ferrari et al. 2006). Despite
great achievements from endovascular stent grafts,
several complications of endovascular stenting
have remained. Although complications do not
occur frequently, endoleak, stent collapse, subcla-
vian occlusion, stroke, embolisation, bronchial
obstruction, implant syndrome, dissection, migra-
tion and paralysis may develop (Karmy-Jones et al.
2009). When the treatment segment of the thoracic
aorta, most commonly the aortic arch, present cer-
tain anatomical challenges, technically complex
stent graft designs are sometimes needed. There-
fore, endovascular treatment of aortic arch disease
may require a custom-made endograft to maintain
the patency of the supra-aortic trunks (SATs) in the
event of a short healthy proximal aortic neck
(Fernández-Alonso et al. 2018). In specific cases
such as these, the custom Terumo Aortic Relay
proximal scalloped stent graft has been particularly
successful (Fig. 1.2). Consequently, anatomically
accurate and interactive 3D visualisations of this
product would be helpful for communicating its
correct usage and other various benefits to both
patients and clinicians.
1.2.3 Potential of Medical
Visualisations for Surgical
Techniques
1.2.3.1 Imaging Modalities
in a Healthcare Setting
In today’s clinical setting, medical imaging is an
essential component of the entire healthcare con-
tinuum, from wellness and screening to early
diagnosis, treatment selection and follow-up.
Some of the most common imaging modalities
used today are computed tomography (CT) and
magnetic resonance imaging (MRI) (Liu et al.
2007). CT imaging allows for clinicians to gain
high levels of detail for anatomical structures and
soft tissue, while MRI [T1 and T2] can assess not
only morphology but also metabolic function
detected by changes in blood flow.
Advancements in computer graphics have
allowed for fast, real-time medical imaging inter-
pretation, giving radiologists the ability to process
a huge amount of data, compare prior studies and
create multiplanar and three-dimensional image
reconstructions. This is done through very thin
(fractions of a millimetre) slices obtained, for
example, in the DICOM image format, and sub-
sequently segmented in an editing software such
as 3D Slicer, Amira, MITK, ITK and Osirix. The
3D volume generated from these imaging
modalities allows for accurate and efficient
visualisation of the patient’s anatomy and physi-
ology (Bercovich and Javitt 2018). CT and MRI
visualisation combined with interactive technol-
ogy allowing for 3D reconstructions will continue
to further the understanding of human disease and
allow a personalised approach to treatment plans.
The process of converting medical imaging
into 3D visualisations follows a general imaging
pipeline (Fig. 1.3). A summary of this pipeline is
as follows: acquiring data, analysing and
visualising medical images for use in diagnosis,
education, or research purposes. Medical imaging
is especially useful to help guide surgical
procedures and enable correct spatial accuracy
visualisation in connection with understanding
cardiac-related complications. Advanced cardiac
CT visualisation technology such as coronary CT
angiography (CTA) is an innovative clinical
imaging tool that allows a non-invasive and
highly specific approach for cardiac diagnosis
and treatment (Saremi 2017; Coelho-Filho et al.
2013; Burt et al. 2014). As aforementioned, gen-
eration of a 3D model from a CT scan can be used
for many reasons to increase patient understand-
ing, surgical planning and informing clinicians
understanding of medical devices for specific
patient treatment (Bercovich and Javitt 2018).
1.2.3.2 Public Engagement for Medical
Visualisation
When examining 3D visualisation for education,
it is also important to consider how well these
technologies are able to educate or otherwise
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 5](https://image.slidesharecdn.com/23351949-250521174800-b3c6a6e5/85/Biomedical-Visualisation-Volume-11-Paul-M-Rea-23-320.jpg)








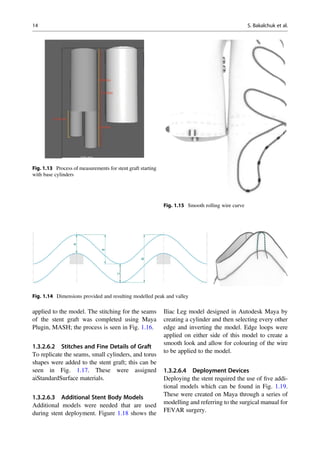












![products, so that the company can effectively
communicate the key features of their products
to clinicians and patients in a more appealing
way. The lack of engaging visualisations and
medical interactive applications for clinical
specialists, supported in the literature, show an
obvious need for these applications to be shown
to clinicians to positively impact their choices in
treating complex aneurysms.
1.6 Conclusion
Advances in understanding stent graft surgical
techniques have led to the need for interactive
applications to engage healthcare workers so
they can exploit its key features to effectively
broaden the treatable patient population. Overall,
the demonstrated methods in this project were
successful in creating animations for interactive
applications that showcased new features of novel
stent grafts. The series of animations for both the
Fenestrated Anaconda and the Relay device made
up a practical interactive application that works to
inform both the physician and patient of various
surgical device options for treating rare, complex
anatomical aortic aneurysm cases. These in turn
provide resources for the physician to visually
explain the surgical procedure and long-term
benefits to a patient. Subsequently, this improves
the discussion between patient and physician,
providing a deeper understanding and patient-
centred surgical approach in elderly patients
who suffer from aortic aneurysms.
Although these applications require additional
testing, and still have a few areas that necessitate
further refinement, these preliminary results show
a great potential for the creation of an application
that can utilise 3D visualisation techniques to
successfully engage both physicians and patients.
The interaction with a surgical device company to
create the anatomical and surgical models,
textures, animations and final application devel-
opment provides an innovative approach to
visualising surgical processes, generating aware-
ness about medical conditions and facilitating
treatment discussions between the physician and
those with aortic aneurysms. Given the range of
positive interactions, as supported in the litera-
ture, of the general public with emerging
visualisation technologies, the applications cre-
ated provide a valid visualisation tool to engage
clinicians, as well as the general public, about
new medical devices, treatment alternatives, and
research pertaining to healthcare an easily acces-
sible visual format (Baker et al. 2002; Ford and
Leinonen 2009; Traxler 2007). The creation of
these applications also establishes a methodology
for building informative surgical tools and posi-
tively influences the healthcare field through
accurate dissemination and communication of
surgical procedures and associated statistics.
References
Abraha I, Romagnoli C, Montedori A et al (2009) Tho-
racic stent graft versus surgery for thoracic aneurysm.
Cochrane Database Syst Rev 1:Cd006796. https://doi.
org/10.1002/14651858.CD006796.pub2
Alsafi A, Bicknell CD, Rudarakanchana N et al (2014)
Endovascular treatment of thoracic aortic aneurysms
with a short proximal landing zone using scalloped
endografts. J Vasc Surg 60(6):1499–1506
Ashton HA, Scott R, Bridgewater SG (2002) Randomized
clinical trial of screening for abdominal aortic aneurysm
in women. Br J Surg [online] 89(3):283–285
Autodesk, Inc. (2020) Maya. Available at: https:/autodesk.
com/maya
Avishay DM, Reimon JD (2020) Abdominal aortic repair.
In: StatPearls. StatPearls Publishing, Treasure Island,
FL
Baker DW, Gazmararian JA, Williams MV et al (2002)
Functional health literacy and the risk of hospital
admission among Medicare managed care enrollees.
Am J Public Health 92(8):1278–1283
Baker DW, Parker RM, Williams MV et al (1998) Health
literacy and the risk of hospital admission. J Gen Intern
Med 13(12):791–798
Ben Abdallah I, El Batti S, Sapoval M et al (2016) Proxi-
mal scallop in thoracic endovascular aortic aneurysm
repair to overcome neck issues in the arch. Eur J Vasc
Endovasc Surg 51(3):343–349
Bercovich E, Javitt MC (2018) Medical imaging: from
roentgen to the digital revolution, and beyond.
Rambam Maimonides Med J 9(4):e0034
British Heart Foundation (2020) Thoracic aortic
aneurysms–Causes, symptoms & treatments. Accessed
28/05
Brown LC, Powell JT, Thompson SG, Epstein DM,
Sculpher MJ, Greenhalgh RM (2012) The UK
endovascular aneurysm repair (EVAR) trials:
randomised trials of EVAR versus standard therapy.
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 27](https://image.slidesharecdn.com/23351949-250521174800-b3c6a6e5/85/Biomedical-Visualisation-Volume-11-Paul-M-Rea-45-320.jpg)

![Shaw PM, Loree J, Gibbons RC (2020) Abdominal aortic
aneurysm (AAA). In: StatPearls. StatPearls Publishing,
Treasure Island, FL
Taylor AM, Wessels Q (2019) Using technology to engage
the public in biomedical sciences. Adv Exp Med Biol
1171:127–135
Traxler J (2007) Defining, discussing and evaluating
mobile learning: the moving finger writes and having
writ. Int Rev Res Open Distr Learn 8(2):43–47
Vascutek Lmtd (2020) Newmains Avenue, Newmains
Ave, Glasgow, Inchinnan, Renfrew PA4 9RR
Wang LJ, Prabhakar AM, Kwolek CJ (2018) Current
status of the treatment of infrarenal abdominal
aortic aneurysms. Cardiovasc Diagn Ther [online]
8(S1):S191–S199
1 Creating Interactive Three-Dimensional Applications to Visualise Novel. . . 29](https://image.slidesharecdn.com/23351949-250521174800-b3c6a6e5/85/Biomedical-Visualisation-Volume-11-Paul-M-Rea-47-320.jpg)










![This ebook is for the use of anyone anywhere in the United States
and most other parts of the world at no cost and with almost no
restrictions whatsoever. You may copy it, give it away or re-use it
under the terms of the Project Gutenberg License included with this
ebook or online at www.gutenberg.org. If you are not located in the
United States, you will have to check the laws of the country where
you are located before using this eBook.
Title: Nenä
Author: Nikolai Vasilevich Gogol
Release date: July 4, 2016 [eBook #52496]
Language: Finnish
Credits: Produced by Tapio Riikonen
*** START OF THE PROJECT GUTENBERG EBOOK NENÄ ***](https://image.slidesharecdn.com/23351949-250521174800-b3c6a6e5/85/Biomedical-Visualisation-Volume-11-Paul-M-Rea-60-320.jpg)



![Hän päätti mennä Iisakin sillalle tuumaellen eikö hänen sieltä
onnistuisi jollakin viekkaudella pudottaa se Nevaan… Mutta
ansaitsenpa moitetta siitä, etten tähän saakka ole virkkanut mitään
Ivan Jakovlevitsista, tuosta monessa suhteessa arvoisasta miehestä.
Ivan Jakovlevits oli, niinkuin kaikki jollaiset venäläiset käsityöläiset,
kauhea juoppo, ja vaikka hän ajelikin joka päivä muitten leukoja, oli
hänen omansa aina ajelematonna. Hännystakki oli hänellä (Ivan
Jakovlevits ei pitänyt koskaan yllään päällystakkia) kirjava, toisin
sanoen se kyllä oli musta, mutta täynnä tummankeltaisia ja harmaita
pilkkuja; kaulus kiiltävä; vaan kolmen napin sijalla rippuivat
ainoastaan rihmat. Ivan Jakovlevits oli oikea syynikkiläinen, ja kuu
kollegi-assessori Kovalev tapansa mukaan partaa ajeltaessa hänelle
sanoi: "Sinun kätesi, Ivan Jakovlevits, haisahtavat jollekin!" niin Ivan
Jakovlevits vastasi kysymykseen: "Millepä ne haisahtaisivat?" "En
tiedä, veikkonen, mutta haisevatpa vaan", sanoi kollegi-assessori, ja
Ivan Jakovlevits, nuuskaa otettuaan, saippuoitti häneltä palkaksi
tästä leuan ja ylähuulen, korvantaustan ja leuanaluksen, sanalla
sanoen — mistä häntä vaan halutti.
Olipa tämä arvoisa porvari jo Iisakin sillalla. Hän katsahti ensin
ympärilleen, kumartui käsipuun ylitse muka tirkistääkseen sillan alle
tokko siellä paljo kaloja uiskenteli, ja pudotti varovasti rievun nenän
kanssa. Hänestä tuntui ikäänkuin kymmenen puntaa olisi harteilta
vierähtänyt: Ivan Jakovlevits oikein naurahti. Sen sijaan, että olisi
virkamiesten leukoja mennyt ajelemaan, käänsi hän askeleensa
laitokseen, jonka oven päällä oli sanat: "Syötävää ja teetä",
pyytääkseen lasillisen totia, kun hän äkkiä hoksasi sillan päässä
seisovan, ylevän näköisen kvartaalin-tarkastajan [korkeampi
poliisivirkamies] leveine poskipartoineen, kolmikulmaisine hattuineen](https://image.slidesharecdn.com/23351949-250521174800-b3c6a6e5/85/Biomedical-Visualisation-Volume-11-Paul-M-Rea-65-320.jpg)

![huomata, että hänellä oli valtioneuvoksen arvo. Kaikesta saattoi
päättää, että hän aikoi juuri aamutervehdykselle. Hän katseli
kummallekin puolelle, huudahti ajurille: "Annas tänne!" astui
vaunuihin ja läksi.
Onneton Kovalev oli vähällä menettää järkensä. Hän ei tiennyt
mitä hänen oli ajatteleminenkaan moisen tapauksen johdosta.
Mitenkä se totta tosiaan olikaan mahdollista, että nenä, joka eilen
vielä oli hänellä tuossa poskien välissä, ei voinut ajaa, eikä kävellä,
nyt oli saanut virkatakin yllensä! Hän juoksi vaunujen jälestä, jotka
onneksi eivät vierineetkään kauas, vaan seisattuivat Gostinnoi dvor'in
eteen [oikeastaan vieraspiha; suuri ryhmä makasiineja ja
kauppapuoteja]. Hän juoksi sinne, tunkeutui läpi joukon kerjääjä-
ämmiä, joitten kasvot olivat peitetyt hunnuilla, mihin vaan silmiä
varten oli kaksi aukkoa jätetty, tuon joukon, jota hän ennen niin
kovasti oli pilkannut. Kansaa ei ollut paljo. Kovalev huomasi olevansa
niin suuresti hämmennyksissään, ett'ei hän kyennyt vakavasti
aprikoimaankaan, ja etsi silmillään tuota herraa joka taholta. Vihdoin
äkkäsi hän hänen seisovan erään puodin edessä. Nenän kasvot olivat
kokonaan pystykauluksen takana piilossa, ja hän katseli syviin
ajatuksiin vaipuneena jotakin esinettä.
"Kuinkahan minä lähenisin häntä?" arveli Kovalev. "Kaikesta —
virkanutusta, hatusta — näkyy, että hän on valtioneuvos. Piru ties
miten tässä on tehtävä!"
Hän alkoi yskiä hänen takanaan; mutta nenä ei vaan muuttanut
hetkeksikään asentoansa.
"Armollinen herra", sanoi Kovalev sisällisesti pakoittaen itseään
rohkeuteen, "armollinen herra…"](https://image.slidesharecdn.com/23351949-250521174800-b3c6a6e5/85/Biomedical-Visualisation-Volume-11-Paul-M-Rea-70-320.jpg)




![ilmoittaa hänen ominaisuutensa, että kuka tahansa, joka nenän
kohtaisi, heti paikalla voisi hänet hänelle toimittaa, taikka ainakin
ilmaista missä nenä oleskeli. Niinpä hän nyt, tämän päätettyään,
käski vosikan ajaa sanomalehti-toimistoon, koko matkan yhtä mittaa
kolhien häntä nyrkillään selkään ja äännähdellen: "Pikemmin lurjus,
pikemmin tolvana!"
"Voi teitä, herra!" sanoi vosikka ravistaen päätään ja lyöden
ohjaksilla hevostaan, jolla oli yhtä pitkä karva kuin katurakilla.
Ruoska seisattui viimein ja Kovalev juoksi hengästyneenä pieneen
vastaanotto-huoneesen, jossa harmaapäinen virkamies, vanha
hännystakki yllä, silmälasit silmillä, istui pöydän takana ja kynä
hampaissa luki vasta tuotuja vaskitahoja. "Kuka täällä ottaa
ilmoituksia vastaan", huusi Kovalev, "hyvää huomenta!"
"Terve tullut", sanoi virkamies kohottaen hetkeksi silmänsä ja
laskien ne takasin vieretysten asetettuihin vaskiraharöykkiöihin.
"Minä tahdon painattaa…"
"Sallikaa, pyydän hiukan odottamaan", lausui virkamies, kirjoittaen
yhdellä kädellään numeroja paperille ja muuttaen vasemman käden
sormilla helmilaudassa kaksi helmeä vasemmalle. Lakeija
nauhuksineen ja puvussa, josta voi päättää hänen palvelevan jossain
ylimysperheessä, seisoi kirje kädessä pöydän luona ja rupesi
näyttämään omaa arvostelukykyään lausuen:
"Uskotteko, herra, ett'ei koira maksa kahdeksaa riunaa [10
kopekkaa], se on minä en siitä maksaisi kahdeksaa rossaa [1/2
kopekkaa], mutta kreivitär, Jumal'aut', rakastaa sitä — senpätähden
se, joka sen löytää, saa sata ruplaa! Totta tosiaan, niin aivan kuin
me tässä, ovat ihmisten maut erilaiset; jos kerran olet koirien ihailija,](https://image.slidesharecdn.com/23351949-250521174800-b3c6a6e5/85/Biomedical-Visualisation-Volume-11-Paul-M-Rea-75-320.jpg)