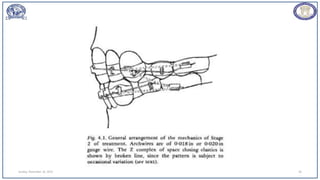
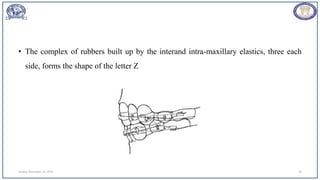
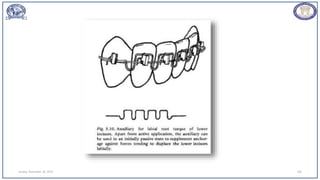
This document discusses the Begg technique for orthodontic treatment, which involves 3 stages. Stage 2 focuses on closing extraction sites by retracting incisors using light archwires and intra/inter-maxillary elastics. The goals are to eliminate remaining space while maintaining the edge-to-edge incisor relationship and Class I buccal occlusion achieved in Stage 1. Intra-maxillary elastics alone risk protruding lower incisors, so inter-maxillary elastics are also used to reinforce upper incisor retraction and provide posterior support to the lower arch.
















![REFERENCES
• Adler T. (1969) Increasing posterior force vectors in Beggtreatment procedures.
Begg]. Orthod. 5, 7-16.
• Angle E. H. (1907) Treatment of Malocclusion of theTeeth. (7th ed.) Philadelphia,
The S. S. White Manufacturing Co.
• Ballard C. F. (1966-7) The morphological bases ofprognosis determination and
practical treatmentplanning. Trans. Br. Soc. Study Orthod. pp. 95-105.
• Barrer H. G. (1967) Elastic thread with the Begg Technique.]. Pract; Orthod. 1,122-
123.
• Barrer H. G. (1969) Nonextraction treatment with theBegg Technique. Am.]. Orthod.
Sunday, November 26, 2023 112](https://image.slidesharecdn.com/beggsseminar0000-231126130118-1e1dc27d/85/beggs-seminar0000-pptx-112-320.jpg)
![• Barrer H. G. (1975) Protecting the integrity of mandibular incisor position.]. Clin.
Orthod. 9,486-494.
• Begg P. R. (1938) Progress report of observations onattrition of the teeth in its relation
to pyorrhea andtooth decay. Aust.]. Dent. 42, 315-320.
• Begg P. R. (1954) Stone Age man's dentition. Am. ].Orthod. 40,298-312, 373-
383,462-475,517-531
Sunday, November 26, 2023 113](https://image.slidesharecdn.com/beggsseminar0000-231126130118-1e1dc27d/85/beggs-seminar0000-pptx-113-320.jpg)
![• Begg P. R. (1956) Differential force in orthodontic treatment. Am.]. Orthod. 42,481-
510.
• Begg P. R. (1961) Light archwire technique. Am. ]. Orthod.47, 33-48.
• Begg P. R. (1962) Questions and answers. Begg]. Orthod.1,55-62
Sunday, November 26, 2023 114](https://image.slidesharecdn.com/beggsseminar0000-231126130118-1e1dc27d/85/beggs-seminar0000-pptx-114-320.jpg)








![Alexander_Discipline_(PART_2)[1] complete.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/alexanderdisciplinepart21-251118184023-04d0c3b3-thumbnail.jpg?width=640&height=640&fit=bounds)



























