
Recommended
More Related Content
What's hot
What's hot (20)
Similar to anatomy of eyelid ophthalmology presentation
Similar to anatomy of eyelid ophthalmology presentation (20)
More from SandeepKrishnan42
More from SandeepKrishnan42 (14)
Recently uploaded
Recently uploaded (20)
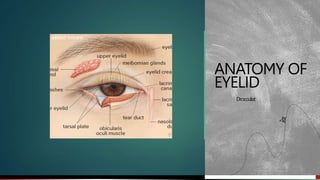
anatomy of eyelid ophthalmology presentation
- 2. Development of eyelid Formed by reduplication of surface ectoderm above and below the cornea during 2nd month of gestation The folds enlarge and their margins meet and fuse with each other Lids cut off a space called conjunctival sac The folds thus formed contain some mesoderm which would form muscles of lid and tarsal plate Lids separate after 7th month of intrauterine life 2
- 3. Gross anatomy . Extent The upper eyelid extends from the eyebrow downward to end in a free margin which forms the superior boundary of palpebral fissure Lower eyelids below merge into the skin of the cheek Position In primary position of gaze upper eyelid covers 1/6th of cornea while lower eyelid just touches the cornea 3
- 4. Lid folds Superior lid fold : 4mm above the edge of eyelid Formed by attatchment of LPS aponeurosis to skin Divide upper eyelid into an orbital portion (above) and a tarsal portion (below) Inferior lid fold On skin of lower eyelid Less distinct Formed by fibrous slips arising from fascia surrounding inferior rectus muscle and are inserted into skin Nasojungal fold and malar fold On lower lid medially and laterally respectively Mark junction between skin and denser tissue of the cheeks – limit spread of blood/fluid downwards from lids to cheek By skin being tethered to underlying periosteum 4
- 5. Palpebral aperture or fissure Elliptical space Between upper and lower eyelid margin At birth 18-21 mm horizontally and 8 mm vertically in the centre In adults its 28-30 mm and 9-11 mm Upper eyelid is more mobile than lower eyelid and can be raised 15 mm by the action of the LPS muscle alone. If frontalis is used, then an additional 2 mm elevation can be achieved 5
- 6. Canthi 2 eyelids meet each other at medial and lateral canthi Lateral canthus lies directly in contact with eyeball Medial canthus is rounded and separated from globe by a small triangular area, the lacus lacrimalis, in the centre of which is a small, pinkish elevation, the caruncula lacrimalis. A semilunar fold – plica semilunaris lies on lateral side of the caruncle. 6
- 7. Normally lateral and medial canthi lie at the same level. Sometimes lateral canthus is slightly elevated (about 2 mm) than medial canthus Mongoloid slant – greater elevation of lateral canthus Antimongoloid slant – lateral canthus placed lower than medial canthus 7
- 8. Eyelid margins Nearly flat, 2 mm wide Each eyelid margin divided into two parts by lacrimal papilla – lacrimal portion and ciliary portion Lacrimal papilla is a small elevation present on medial side ,containing an opening called lacrimal punctum in its centre Lacrimal portion – extending from punctum medially to the medial canthal angle Rounded and devoid of lashes or glands Ciliary portion – lateral part Rounded anterior border and sharp posterior border and an intermarginal strip between the two 8
- 9. Grey line represents line of demarcation between the anterior portion of the eyelid formed by the skin and orbicularis muscle and posterior formed by the tarsus and conjunctiva It divides intermarginal strip into anterior strip bearing lashes and a posterior strip containing meibomian glands arranged in a row and a lipid strip Surgically important for splitting of eyelid with minimal scarring 9
- 10. Eyelashes Arranged in 2 or 3 rows along anterior part of intermarginal strip Longer and more numerous on the upper eyelid(100-150) than on lower one(50- 75) On upper eyelid- forward, upward and backward while on lower eyelid- forward, downward and backward Vary in size ranging from 20-120 mm in diameter and 6-12 mm in length Lifespan – 3 to 4 months 10
- 11. Lash follicles pass obliquely in the lids, lack errectores and are embedded in the fibrous tissue that binds the ciliary margin of the tarsus to the underlying skin The sebaceous gland of Zeis and glands of Moll empty into the infundibulum of each ciliary canal. Each lash follicle is surrounded by a dense plexus of vessels and nerves. 11
- 12. Layers of eyelid From superficial to deep Skin Layer of subcutaneous areolar tissue Layer of striated muscles Submuscular areolar tissue Fibrous layer Layer of non striated muscle fibres Conjunctiva 12
- 13. Skin Elastic having a fine texture Thinnest in the body and folds easily thereby Nasal part of the skin is smooth, shining and greasy in comparison to the temporal part Fine hair are seen on temporal part of the skin 13
- 14. Microscopic structure The epidermis is composed of 6-7 layers of stratified squamous epithelium and have stratum corneum, stratum granulosum, stratum mucosum and stratum germinatum resting on a basement membrane The basal layer of epidermis shows unicellular sebaceous glands and numerous typical eccrine sweat glands At the lid margin epithelium is modified as we go from anterior to posterior and becomes continuous with that of conjunctiva 14
- 15. The dermis or corium is composed of thin layer of dense connective tissue, with rich network of elastic fibres, blood vessels, lymphatics and nerves A variable amount of melanocytes are also present which may increase their pigment production in response to chronic oedema or inflammation 15
- 16. Subcutaneous areolar tissue Lies beneath the skin Loose areolar connective tissue with no fat – readily distended by edema and blood Overlying skin may be easily mobilized during plastic surgery Non existent near ciliary margin, at the lid folds and at the medial and lateral angles where the skin is attached to the underlying ligaments 16
- 17. Layer of striated muscles This layer consists of two muscles: 1. Orbicularis oculi (forms a thin oval sheet across eyelids) 2. Levator palpebrae superioris 17
- 18. The orbicularis oculi muscle It can be divided into 2 parts Orbital part Palpebral part (pretarsal and preseptal part) 18
- 19. The orbital part Forms most peripheral fibres of orbicularis Arise from anterior part of the medial palpebral ligament and adjacent bones ( upper orbital margin medial to the supraorbital notch, the maxillary process of frontal bone, frontal process of maxilla and the lower orbital margin medial to infraorbital foramen From orgin muscle fibres sweep superiorly and inferiorly, covering orbital margin in form of large ellipse and meet at the lateral palpebral raphe 19
- 20. Superiorly deep to the eyebrow the orbicularis fibres intermingle with those of the frontalis and thus gain insertion into skin of eyebrow Musculus superciliaris – upper medial fibres which passs to skin of the medial part of eyebrow Musculus malaris – inferior medial and lateral fibres attatched to skin of cheek They help in forced closure of eyelids and thus pull eyebrows downwards 20
- 21. The palpebral part- overlies mobile eyelid from orbital rim to eyelid margins Subdivided into preseptal and pretarsal portions Preseptal fibres – arise from lacrimal fascia, posterior lacrimal crest (deep head) and the anterior part of medial palpebral ligament (superficial head) Fibres pass superiorly and inferiorly in front of orbital septum and unite at the lateral palpebral raphe 21
- 22. Pretarsal fibres – arise from deep head (lacrimal fascia and posterior lacrimal crest) and superficial head (medial palpebral ligament) Fibres pass laterally above and below, overlying the upper tarsus and lower tarsus respectively and join laterally to form a lateral canthal tendon (inserted over lateral orbital tubercle of Whitnall) The fibres of pretarsal portion which arise from lacrimal fascia and upper part of posterior lacrimal crest help in drainage of tears by lacrimal sac and are known as Pars lacrimalis (horner’s muscle) 22
- 23. Fibres which run along the lid margin behind the ciliary follicles form the Pars ciliaris (muscle of Riolan) and these fibres keep lids in close apposition to globe In general the palpebral part helps in gentle closing of eyelids during blinking ,sleep and soft voluntary closure. Supplied by branches of facial nerve Antagonist is LPS 23
- 24. The levator palpebrae superioris muscle Orgin At the apex of the orbit from the undersurface of lesser wing of sphenoid above the annulus of zinn, by a short tendon which is blended with the underlying orgin of superior rectus muscle 24
- 25. Course and Attachments Has a flat ribbon like belly. It overlies superior rectus as it travels anteriorly towards the eyelid and numerous fascial bands connect the two Widens as it courses forward and then descends vertically posterior to orbital fat wedge At orbital septum it fans out into aponeurosis of LPS and forms medial and lateral horn 25
- 26. Lateral horn divides lacrimal gland into orbital and palpebral parts and inserts into superior edge of lacrimal canthal tendon Medial horn passes over reflected tendon of superior oblique and fuses with medial canthal tendon Together the two horns serve to distribute the forces of levator muscle along the aponeurosis and the tarsal plate Fleshy part of LPS muscle runs horizontally while tendinous aponeurosis runs vertically This change of direction occurs at superior transverse ligament of whitnall 26
- 27. The Whitnall ligament (also known as check ligament of LPS) is a thickened band of orbital fascia which extends from trochlear pulley to the capsule of the orbital lobe of lacrimal gland Formed by condensation of superior sheath of levator muscle joined medially by sheath of reflected tendon of superior oblique muscle Cutting of whitnall ligament in ptosis surgery can lead to failure of LPS LPS supplied by superior division of occulomotor nerve Acts elevator of upper lid and is antagonised by palpebral portion of orbicularis oculi muscle 27
- 28. Submuscular areolar tissue Layer of loose connective tissue between orbicularis muscle and fibrous layer Consists of tarsal plate and septum orbitale Contains nerves and vessels of the lids – injection is made here to anaesthetise the lid This layer splits the eyelid into two – anterior lamina and posterior lamina (approached through grey line) 28
- 29. In upper eyelid this layer communicates with dangerous area of scalp (subaponeurotic stratum of scalp) – pus or blood can make its way here In lower eyelid submuscular tissue lies in a single space behind the orbicularis In the upper eyelid ,this space is traversed by levator muscle which divides it into pretarsal space and preseptal space 29
- 30. Pretarsal space Small fusiform area in vertical section Peripheral arterial arcade present Bounded anteriorly by levator aponeurosis and posteriorly by tarsal plate Preseptal space Triangular in vertical section Bounded in front by orbicularis ,behind by septum orbitale and above by preseptal cushion of fat 30
- 31. Fibrous layer Framework of lid and consists of Central thick part of tarsal plate Peripheral thin part of septum orbitale (palpebral fascia) Medial palpebral ligament Lateral palpebral ligaments 31
- 32. Tarsal plates Firm plates of dense fibrous tissue that form skeleton of eyelids giving shape and firmness About 29 mm long and 1 mm thick Upper tarsus 10-11 mm in height and lower tarsus 4-5 mm in height Free borders of tarsi are more or less straight whereas opposite attatched borders are convex Septum orbitale and Mullers muscle are attatced to superior border of upper tarsus The orbital septum, capsulopalpebral fascia and inferior palpebral muscle are attatched to inferior border of lower tarsus 32
- 33. Firm plates of dense fibrous tissue that form skeleton of eyelids giving shape and firmness About 29 mm long and 1 mm thick Upper tarsus 10-11 mm in height and lower tarsus 4-5 mm in height Free borders of tarsi are more or less straight whereas opposite attatched borders are convex Septum orbitale and Mullers muscle are attatced to superior border of upper tarsus The orbital septum, capsulopalpebral fascia and inferior palpebral muscle are attatched to inferior border of lower tarsus 33
- 34. Septum orbitale/ Palpebral fascia Firm plates of dense fibrous tissue that form skeleton of eyelids giving shape and firmness About 29 mm long and 1 mm thick Upper tarsus 10-11 mm in height and lower tarsus 4-5 mm in height Free borders of tarsi are more or less straight whereas opposite attatched borders are convex Septum orbitale and Mullers muscle are attatced to superior border of upper tarsus The orbital septum, capsulopalpebral fascia and inferior palpebral muscle are attatched to inferior border of lower tarsus 34
- 35. Structures piercing through septum orbitale 1. Lacrimal vessels and nerves 2. Supraorbital vessels and nerves 3. Supratrochlear artery and nerve 4. Infratrochlear nerve 5. Anastomosing vein between the angular and ophthalmic vein 6. Superior and inferior palpebral arteries 7. Aponeurosis of LPS in the upper eyelid 8. Expansion of inferior rectus in the lower eyelid 35
- 36. Medial palpebral ligament Triangular band of connective tissue, attached to the frontal process of maxilla from anterior lacrimal crest to suture line of frontal process with the nasal bone It can be divided into 2 parts : anterior and posterior Anterior part fans out laterally from anterior lacrimal crest and at medial canthus splits into upper and lower band that are attached to medial ends of upper and lower tarsal plates respectively Posterior part passes behind lacrimal sac from anterior lacrimal crest to posterior lacrimal crest 36
- 37. Lateral palpebral ligament Thin band of fibrous tissue Laterally attactched to Whitnall’s tubercle on lateral orbital margin Medially attached to lateral ends of upper and lower tarsal plate Upper border of LPL merges with lateral expansion of aponeurosis of levator muscle and the lower border with the lateral expansions of inferior oblique and inferior rectus muscles 37
- 38. Layer of non striated muscle fibres Consists of smooth muscle fibres of Muller which lie deep to septum orbitale in upper and lower lid Orgin : from inferior terminal striated fibres of LPS in upper eyelid and expansion of inferior rectus in lower eyelid Runs vertically and gets inserted in the orbital margin of the tarsal plate Supplied by sympathetic nerves Thus sympathetic irritation leads to retraction of lids and paralysis leads to Horners syndrome 38
- 39. Conjuctiva Posterior most layer of eyelid Extends from mucocutaneous junction at the lid margin to the conjunctival fornix It is firmly adherent to the posterior surface of tarsal plates and Muller’s muscle 39
- 40. Glands of the eyelids These include Tarsal / Meibomian glands Gland of Zeis Glands of Moll Accessory lacrimal glands of Wolfring 40
- 41. Tarsal / Meibomian Glands Modified sebaceous glands present in posterior part of stroma of tarsal plates They are arranged in single row vertically parallel to each other numbering about 20-30 in each lid Each gland contains central duct which runs straight perpendicular to the lid margin and occupies the entire thickness of tarsal plate Opening of meimobian glands are arranged in a single row on the lid margin between grey line and posterior border of lid 41
- 42. Secretions Secretions are oily in nature The oily marginal tear strip prevents overflow of tears across lid margin Prevents evaporation of tears and allow smooth movements of eyelids over the globe Ensure airtight closure of eyelids 42
- 43. Gland of Zeis Modified sebaceous glands Attached to eyelash follicles (usually 2 glands with each cilium) Unilobar Sebum secretion prevents eyelashes from becoming dry and brittle Also contributes towards oily layer of tear film 43
- 44. Gland of Moll Modified sweat gland Lies between cilia More numerous in lower lid than in upper lid Has unbranched spiral shape 44
- 45. Accessory gland of Wolfring Microscopic accessory lacrimal glands Present along upper border of superior tarsus and along lower border of inferior tarsus About 2-5 in upper eyelid and 2-3 in lower eyelid 45
- 46. Arterial supply Each eyelid mainly supplied by medial and lateral palpebral arteries (branches of dorsal, nasal and lacrimal arteries Anastomoses of medial and lateral palpebral arteries toform Marginal and peripheral arterial arcades 46
- 47. Venous drainage 2 sets of venous plexus on each eyelid Pretarsal venous plexus – drains structures superficial to tarsus. It drains into subcutaneous veins Angular vein on medial side which ultimately drain into internal jugular vein The superficial temporal and lacrimal veins on lateral side ultimately drain into external jugular vein Post tarsal venous plexus – drains structures posterior to tarsal plate and in turn drains into ophthalmic vein 47
- 48. Lymphatic drainage Superficial or pretarsal plexus – drains lymph from skin and orbicularis muscle Deep or post-tarsal plexus – drains lymph from tarsal plate region and conjunctiva 48
- 49. Nerve supply Motor nerves – facial and occulomotor Sensory nerves – branches of 1st and 2nd division of trigeminal nerve Upper lid- supraorbital, suptratrochlear, infratrochlear and lacrimal nerves Lower lid – infraorbital, lacrimal and infratrochlear nerves Sympathetic nerves supply the vessels , glands and mullers muscle 49
- 50. Clinical correlations of eyelid Hordeolum Externum (Stye) – localized suppurative inflammation of gland of zeis at lid margin at ciliary follicle Hordeolum Internum – inflammation of meibomian gland associated with blockage of duct Chalazion – chronic inflammatory granuloma of meibomian gland 50
- 51. Blepharitis Chronic inflammation of lid margin occurring as true inflammation 51
- 52. Meibomitis (posterior Blepharitis) Inflammation and obstruction of meibomian glands. Characterized by diffuse thickening of posterior border of eyelid margin which becomes rounded 52
- 53. Inward rolling and rotation of lid margin towards globe Entropion Out rolling of eyelid margin Ectropion 53
- 54. Incomplete closure of the palpebral aperture when attempt is made to close the eyes Lagophthalmos Drooping of upper eyelid usually due to paralysis or defective development of LPS Ptosis 54 Central thick part of tarsal plate Peripheral thin part of septum orbitale (palpebral fascia) Medial palpebral ligament Lateral palpebral ligaments
- 55. Blepharospasm Involuntary , sustained and forceful closure of the eyelids 55
- 56. Partial or complete adhesion of the palpebral conjunctiva of the eyelid to the bulbar conjunctiva of the eyeball Symblepharon Adhesion of ciliary edges of the eyelid to each other Ankyloblepharon 56
- 57. Extra row of cilia occupies position of meibomian glands Distichiasis Inward misdirection of cilia Trichiasis 57
- 58. Coloboma of lid Notch in edge of the lid Usually situated to the inner side of midline, generally affecting upper lid Sometimes a bridge of skin links coloboma to the globe 58
- 59. Rare condition where skin passes continously from brow over the eye to the cheek Cryptophthalmos Lids are abnormally small Microblepharon 59
- 60. THANKYOU 60