
Recommended
More Related Content
Similar to All GIT.pdf
Similar to All GIT.pdf (20)
Recently uploaded
Recently uploaded (20)
All GIT.pdf
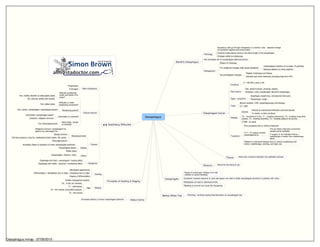
- 1. Oesophagus Barrett's Oesophagus Pathology Squamous cells go through metaplasia to columnar cells - adaptive change for protection against acid environment Could be small patchy areas or the entire length of the oesophagus Changes visible on endoscopy 40x increased risk of oesophageal adenocarcinoma Management Biopsy for histology Pre malignant changes (high grade dysplasia) Oesophageal resection (in younger, fit patients) Mucosal ablation (in other patients) No premalignant changes Regular endoscopy and biopsy Intensive anti-reflux measures (including long term PPI) Oesophageal Cancer Incidence 9 / 100,000 a year in UK Risk factors Diet, alcohol excess, smoking, obesity Achalasia, reflux oesophagitis, Barrett's oesophagus Signs / symptoms Dysphagia, weight loss, retrosternal chest pain Hoarseness, cough Tests Barium swallow, CXR, oesophagoscopy with biospsy CT / MRI Staging Spread Directly by submucosal infiltration and local spread To nodes, or later via blood Tis - carncinoma in situ; T1 - invading submucosa; T2 - invading muscularis propria; T3 - invading adventitia; T4 - invading adjacent structures (T)NM - as usual Treatment Poor prognosis with or without treatment If T1 / T2 radical curative oesophagectomy Pre-op chemo improves survival but causes some morbidity If surgery is not indicated chemo + radiotherapy is better than radiotherapy alone Palliation in advanced disease aims to restore swallowing with chemo, radiotherapy, stenting, and laser use Fistula Abnormal connection between two epithelial surfaces Stricture Abnormal narrowing of gut Oesophagitis Range of endoscopic findings from mild redness to severe bleeding Excessive mucosal exposure to acid and pepsin can lead to distal oesophageal ulceration in patients with reflux Metaplasia can lead to adenocarcinoma Bleeding is common but rarely life threatening Mallory Weiss Tear Retching / vomiting causing haematemesis via oesophageal tear Hiatus hernia Increased patency of lower oesophageal sphincter Principles of Grading & Staging Grading Histological appearance Differentiated > Metaplasia (low to high) > Dysplasia (low to high) Degree of differentiation Staging Guides management options TNM Tis - in situ (on mucosa) T1 - submucosa T2 - into muscle (muscularis propria) T3 - into serosa Swallowing Difficulties Alarm Symptoms Progressive Prolonged Clinical features Difficulty swallowing solids and liquids from onset? Yes: motility disorder or pharyngeal cause No: stricture (solids then liquids) Difficultly to make swallowing movement? Yes: bulbar palsy Swallowing painful? Yes: cancer, oseophagitis, oseophageal spasm Intermittent or constant? Intermittent: oesophageal spasm Constant: malignant stricture Neck bulge / gurgle on drinking? Yes: pharyngeal pouch Causes Mechanical block Malignant stricture: oesophageal Ca, gastric Ca, pharyngeal Ca Benign stricture Extrinsic pressure: lung Ca, mediastinal lymph nodes, AA, goitre Pharyngeal pouch Motility Achalasia (failue of relaxation of lower oesophageal sphincter) Oesophageal spasm Bulbar palsy Others Oesophagitis: infection, reflux Categories Dysphagia with fluid = neurological / muscle deficit Dysphagia with solids = physcial / mechanical deficit Oesophagus.mmap - 07/09/2010 -
- 2. Peptic Ulcer Disease 1 Dyspepsia Symtpoms: epigastric pain, bloating, heartburn Alarm symptoms: Anaemia (iron deficiency), weight loss, anorexia, melaena, haematemesis, swallowing difficulty Management If > 55yrs or alarm symptoms refer for urgent endoscopy Simple anatacids for 4 weeks Test for H. Pylori and eradicate if present; otherwise PPI for 2 weeks Management Lifestyle Avoid food that worsens symptoms Stop smoking (smoking slows healing in GU and increases relapses in DU) Clinical H. Pylori eradication Triple therapy PAC500 regime: PPI, amoxicillin & clarithromycin PMC 250: PPI, metronidazole & clarithromycin Upto 85% effective For 7 days Drugs to reduce acid PPIs Lansoprazole 30mg / 24hrs H2 Receptor Antagonists Ranitidine 300mg nocte Cimetidine 800mg nocte Ulcers Duodenal 4x more common than gastric Major risk factors: H. Pylori (90%), drugs (aspirin, NSAIDs, steroids) Minor risk factors: increased gastric acid secretion, increased gastric emptying (lowers duodenal pH), blood group O, smoking, ?stress Symptoms: epigastric pain (before meals / night) relieved by eating or drinking milk, asymptomatic (50%), recurrent Signs: epigastric tenderness Diagnosis: upper GI endoscopy (stop PPI 2 week prior), H. Pylori test Gastric Occur mainly in the elderly Risk factors: H. Pylori (80%), smoking, NSAIDs, duodenal reflux, delayed gastric emptying, stress Symptoms: asymptomatic, epigastric pain (related to meals / relieved by antacids) +/- weight loss Tests: upper GI endoscopy (to exclude Ca), biopsies from ulcer rim and base (histology / H. Pylori) Complications Bleeding Perforation Presenting features depends on how ulcer bursts Malignancy Gastric outflow obstruction H. Pylori Infection Spiral shaped gram negative urease producting bacterium Found in gastric antrum and in areas of gastric metaplasia in the duodenum Pathogenesis Colonisation in the antrum Inflammation of the gastric mucosa (gastritis) Gastric inflammation may lead to gastric or duodenal ulcer formation Diagnosis 13C Urea breath test Very sensitive (98%) and specific (95%) Breath test also used to demonstrate eradication Laparotomy Post-op complications General Pain Pyrexia Confusion Dyspnoea / Hypoxia Hypo / Hypertension Oliguria Nausea / Vomiting Hyponaturaemia Specific Wound breakdown / dehiscence (esp. elderly and malnourished) May lead to burst abdomen A&P Stomach Anatomy Cardia Abundant mucous glands to protect oseophagus Fundus In contact with the diaphragm Body Contains the gastric glands secreting enzymes and acids Pylorus Pyloric antrum and pyloric canal Pyloric sphincter regulates release into duodenum Glands secrete mucous and digestive hormones Glands Gastric Parietal cells Proximal portion of gland Secrete hydrochloric acid (H+ via proton pump along with Cl-) and intrinsic factor (absoprtion of B12) Chief cells Abundant near base of gland Secrete pepsinogen Pyloric Cells primarily produce a mucous secretion G Cells Abundant in gastric pits of pyloric antrum Secrete gastrin (stimulates parietal and chief cells) D Cells Continually release somatostatin, inhibiting gastrin release Overridden by neural and hormonal stimuli Histiology Columnar epithelium Peptic Ulcer Disease.mmap - 07/09/2010 -
- 3. Peptic Ulcer Disease 2 Peritonitis Peritonitis Perforated ulcer Perforated diverticulum Perforated appendix Perforated bowel Perforated gall bladder Signs Prostration; shock; lying still; positive cough test Tenderness; abdo rigidity, guarding, absent bowel sounds Erect CXR may show gas under diaphragm (pneumoperitoneum) Management Usually requires a laparotomy Acute pancreatitis causes these signs but does not require a laparotomy - check serum amylase (massively raised in acute pancreatitis) Endoscopy Pre procedure Stop anti acid therapy 2 weeks before hand (can mask adenocarcinomas) Nil by mouth for 8 hrs; water up till 4 hrs Procedure Sedation Pharynx sprayed wirh local anaesthetic and flexible endoscope passed Suction to prevent aspiration Complications Transient sore throat Amnesia following sedation Perforation (< 0.1%) Consent Consent Patient must have capacity to give consent Before intervention is initiated Intervention is understood by the patient (risks, benefits, complications, alternatives, consequences) Voluntarily given Capacity Adult is assumed to have capacity unless proven otherwise Four parts Understand and accept information is true Remember what has been said Show reason (to weigh up choices) Communicate decision Upper Abdo Pain Dudodenal ulcer Non-ulcer dyspepsia Duodenal Crohn's TB, lymphoma Pancreatic Ca Dyspepsia Non- ulcer dyspepsia Duodenal ulcer Duodenitis Gastritis / Gastric ulcer Gastric malignancy GORD Oesophagitis Pneumoperitoneum Perforation Gas forming infection Iatrogenic (surgery) Per vaginam (water ski-ing, vigorous intercourse) Interposition of bowel between liver and diaphragm Peptic Ulcer Disease 2.mmap - 07/09/2010 -
- 4. Malabsorption IBD Ulcerative Colitis Relapsing / remitting inflammatory disorder of colonic mucosa; never spreads proximal to ileocaecal valve Pathology Hyperaemic / haemorrhagic granular colonic mucosa +/- pseudopolyps Inflammation is normally not transmural Histology Inflammatory infiltrate; goblet cell depletion; glandular distortion; mucosal ulcers; crypt abscesses Epidemiology Prevalence: 100 - 200 / 100,000 Incidence: 10 - 20 / 100,000 a year Most present 15 - 30 yrs; 3 x more common in non-smokers Symptoms / Signs Symptoms Gradual onset of diarrhoea (+/- blood and mucus); crampy abdo pain; increased frequency of bowels; systemic symptoms common during attacks (fever, malaise, anorexia, weight loss) Signs May be none In acute / severe episodes: fever, tachycardia, tender / distended abdo Peripheral Manifestations Clubbing; oral ulcers; erythema nodosum (purple, painful nodules on shins); conjuctivitis; iritis (inflammation of iris); large joint arthritis; fatty liver Tests Usual bloods FBC, ESR, CRP, U&E, LFT, cultures Stool cultures to exclude infection AXR: no faecal shadows, mucosal thickening Sigmoidoscopy: inflamed, friable mucosa Rectal biopsy: inflammatory infiltrate, goblet cell depletion, mucoal ulcers, crypt abscesses Complications Perforation and bleeding Toxic dilatation of colon; venous thrombosis; colonic cancer Management Inducing remission Mild UC (< 4 motions / day) Prednisolone for 2 weeks (oral or retention enemas) Moderate UC (4 - 6 motions / day) Oral Prednisolone for 2 weeks + 5-ASA + steroid enemas Severe UC (> 6 motions / day) Treat as inpatient Maintaining remission 5-ASA Infliximab Surgery 20% will require surgery at some point Proctocolectomy and terminal ileostomy Indications for surgery Perforation; haemorrhage; toxic dilatation; failure of medical therapy Crohn's Disease Chronic inflammatory disease characterised by transmural granulmatoud inflammation; can affect any part of the gut but favours terminal ileum and proximal colon; skip lesions (unaffected bowel areas between areas of disease) differentiate Crohn's from UC Epidemiology Prevalence: 50 - 100 / 100,000 Incidence: 5 - 10 / 100,000 per year Associations: high sugar, low fibre diet, altered cell mediated immunity, smoking, NSAIDs Symptoms / Signs Symptoms Diarrhoea, abdo pain, weight loss Fever, malaise, anorexia (with active disease) Signs Abdo tenderness, right iliac fossa mass, perianal absecess / fistulae / skin tags, anal / rectal strictures Peripheral Manifestations Ahthous ulceration (oral mucous ulcer), clubbing, erythema nodosum, iritis, fatty liver, large joint arthritis Complications Small bowel obstruction; toxic dilatation; abscess formation; fistulae; rectal haemorrhage; colonic cancer (rarer than in UC) Tests Usual bloods FBC, ESR, CRP, U&E, LFT, cultures, serum iron, vit B12 Colonoscopy to assess disease extent Management Mild attacks Prednisolone Severe attacks IV steroids, nil by mouth, IV hydration Hydrocortisone IV, topical steroids for rectal disease Nutrients required for Health Vitamin B12 Absorbed in the terminal ileum Deficiency causes: macrocytic anaemia, neuropathy, glossitis Vitamin C Absorbed in the proximal ileum Deficiency causes: scurvy Malabsorption Common in UK: coeliac disease, chronic pancreatitis, Crohn's Decreased bowel; pancreatic insufficiency; small bowel mucosa; bacterial overgrowth; infection; intestinal hurry Malabsorption Syndromes Coeliac disease T cell mediated autoimmune disease of small bowel in which prolamin intolerance causes villous atrophy and malabsorption Presentation Can occur at any age (peaks in infancy and 50s) One third are asymptomatic Steatorrhoea; abdo pain; bloating; nausea & vomiting; angular stomatitis; weight loss; fatigue; incidental iron def anaemia Diagnosis An IgA antibody, 95% specific Duodenal biopsy via endoscopy: villous atropy and crypt hyperplasia - reversing on gluten free diet Management Lifelong gluten free diet Rice, maize, soya, potatoes, oats and sugar are Ok Gluten free biscuits, flour, bread and pasta are prescribable Complications Anaemia; secondary lactose intolerance; increased risk of malignancy Chronic pancreatitis Causes Typically alcohol Rarely familial, CF. haemochromatosis, pancreatic duct obstruction Presentation Epigastric pain through to pack (relieved by sitting forward or hot water bottles on epigastrium / back) Bloating, steatorrhoea, weight loss, brittle diabetes Symptoms relapse and worsen Tests Ultrasound (pseudocyst), CT, AXR (speckled pancreatic calcification) Management Drugs Analgesia Lipase + fat soluble vitamins Diet No alcohol; low fat diet Surgery Indications: unremitting pain, weight loss Complications Pseudocyst; diabetes; bilary obstruction; local arterial aneruysm; gastric varices Malabsorption.mmap - 07/09/2010 -
- 5. Irritable Bowel Syndrome Clinical features Presentation Typically 20 - 40 years; female predominance Symptoms Abdo pain (relieved by defecation); bloating; altered bowel habit; tenesmus; muscus PR Less commonly: nausea; dyspareunia; pain in back / thigh / chest; change in urinary frequency; depression Chronic > 6 months, exacerbated by stress, menstruation, or gastroenteritis Signs Examination often normal, although generalised tenderness is common Insufflation of air during sigmoidoscopy may reproduce pain Red flags Factors suggesting disease other than IBS Age > 40 yrs; history < 6 months Anorexia; weight loss; waking at night (pain / diarrhoea) Mouth ulcers; abnormal investigations; PR bleeding Management Rarely 100% effective Particularly medical therapy Be pragmatic Food intolerance Try exclusion diets Although may lead to obsessions Constipation Increase fibre intake gradually Non fermentable fibre (Fybogel) is better than fermenting (Lactulose) - increased gas production adds to bloating Diarrhoea Bulking agent +/- loperamide after each loose stool Colic & bloating Anti spasmodics may help Dyspeptic symptoms Antacids Psychological therapy Emphasise positive prognosis 50% improve after one year Tricyclics in low dose can be helpful Diagnosis of Exclusion Aetiology Heterogeneous group of abdo symptoms with no found organic cause Probably due to disorders of intestinal motility or enhanced visceral perception (brain gut axis) Exclude other diagnoses Young with classic history FBC, ESR, LFT, coeliac serology Urinalysis, sigmoidoscopy Patient aged > 45 years or evidence of organic disease Colonoscopy Prominent diarrhoea LFT, stool culture, B12 & folate TSH, antiendomysial antibodies (coeliac) barium follow through Further investigation guided by symptoms Upper GI endoscopy (dyspepsia) Duodenal biopsy (coeliac) Small bowel radiology (CD) ERCP (chronic pancreatitis) or MRCP (active pancreatitis) When to refer Changing symptoms in known IBS To dietician with food intolerance For psych input with pronounced depression For gynae with cyclical pain Irritable Bowel Syndrome.mmap - 07/09/2010 -
- 6. Bowels Bowel Cancer Epidemiology 2nd most common cause of cancer death 32,000 cases per year, 50% mortality More common in urban than rural areas Genetic links / family history No close relative affected CRC risk = 1 / 50 1 close relative CRC risk = 1 / 17 2 close relatives CRC risk = 1 / 10 Predisposing / protective factors Predisposing: neoplastic polyps, UC, Crohn's, FAP, HNPCC, previous Ca, low fibre diet, red meat Protective: NSAIDs and aspirin Presentation Left sided bleeding / mucus PR, altered bowel habits, tenesmus, PR mass Right sided Weight loss, low Hb, abdo pain Either abdo mass, obstruction, perforation, haemorrhage, fistula Significant symptoms Rectal bleeding & change in bowel habit (35% risk of CRC); abdo / rectal mass (30% risk of CRC); iron def anaemia (30% risk of CRC) Tests FBC (microcytic anaemia), FOB Proctoscopy, sigmoidoscopy, barium enema, colonoscopy (can be done virtually via CT) CEA Blood tumour marker for CRC Crude screening method Better for monitoring reoccurence Distribution 15 % caecum & ascending colon, 10% transverse colon 5% descending colon, 25% sigmoid colon, 45% rectum At least half are located in the sigmoid or rectum Staging Dukes A - confined to bowel wall (90% 5 yr survival) B - through bowel wall (65% 5 yr survival) C - lymph node involvement (30% 5 yr survival) D - distant mets (<10% 5 yr survival) TNM Tis - in situ (on mucosa) T1 - submucosa T2 - into muscle (muscularis propria) T3 - into serosa Spread Local, lymphatic, by blood (liver, lung, bone), or transcoelomic Management T1 Could use transanal resection 5% chance of leaving behind involved lymph nodes T2 Surgery alone Autonomic nerves can be affected by removal of rectal cancer Risk of sexual and bladder dysfunction T3 Pre-op radiotherapy (due to risk of leaving cancer behind) Then surgery T4 Pre-op radiotherapy + / - chemotherapy Then surgery Diverticular Disease Definitions Diverticulum Outpouching of the gut wall Diverticulosis Diverticula are present Diverticular disease Implies diverticula are symptomatic Diverticulitis Inflammation of diverticulum Pathology Patient has had motions which are hard to pass and becomes constipated Acquired colonic diverticula are the most common type Most occur in the sigmoid colon (95% complication occur at this site) Lack of dietary fibre leads to high intraluminal pressure > forces mucosa to herniate through muscle layers of gut wall 30% of westerners have diverticulosis by 60 yrs Diagnosis PR; sigmoidoscopy, barium enema, colonoscopy; CT Management Symptoms / Signs: altered bowel habit, left sided colic (relieved by defecation, nausea, flatulence High fibre diet Antispasmodics Surgical resection may be resorted to Stool softeners Complications Diverticulitis Features: pyrexia, raised WCC & CRP / ESR, tender colon, localised peritonism Treatment: analgesia, NBM, IV fluids, antibiotics Pain - left iliac fossa Perforation Features: ileus, peritonitis, shock 40% mortality Treated as acute abdo Haemorrhage Usually sudden and painless Common cause of big rectal bleeds Fistulae Enterocolic, colovaginal ir colovesical Treatment is surgical Abscesses Features: swinging fever, leucocytosis, localised signs Treatment: antibiotics with ultrasound guided drainage Post infective strictures May form in the sigmoid colon Investigations Red Flags (for 2 week referral) Rectal bleeding & change in bowel habit for 6 weeks Rectal bleeding without anal symptoms in those over 45 yrs Iron deficiency anaemia without obvious cause Palpable abdo / rectal mass 2 episodes of FOB+ separated by a period of time Value of investigations FOB CRC national screening programme Aged 60 - 69; two yearly 2% FOB + (10% of these will have CRC) Test is not very sensitive, although is used for risk reduction Sigmoidoscopy Screen for left sided lesions 90% sensitivity & 99% specificity Limitations Acceptability and cost Does not pick up right sided lesions Colonoscopy Examines the entire colon Perforation rate (0.2%) is higher than sigmoidoscopy (0.01%) Limitations Costs, need for sedation, acceptability, limited availability of trained staff Bowels.mmap - 21/10/2009 -
- 7. Liver 1 Immunity Vaccine - attenuated strain of virus Innoculation - IgG IgM - immediate release IgG - long term and base line protection Cirrhosis Irreversible liver damage - loss of normal hepatic architecture with fibrosis and nodular regeneration Causes Chronic alcohol abuse HBV and HCV infection Signs May be done other than abnormal LFTs Leuconychia, clubbing, palmar erythema, hyperdynamic circulation Dupuytren contracture, spider naevi, gynaecomastia, parotid enlargement, hepatomegaly Complications Hepatic failure Coagulopathy Encephalopathy Liver flap Confusion / coma Hypoalbuminaemia Oedema Sepsis Spontaneous bacterial peritonitis Hypoglycaemia Portal hypertension Ascites Splenomegaly Oesophageal varices Caput medusae Management General Good nutrition; low salt diet; alcohol abstinence Avoid NSAIDs, sedatives and opiates` Interferon alpha Ascites Bed rest, fluid restriction Spironolactone SBP Common organisms E Coli, Klebsiella and Strept Antibiotics Liver Transplant Increases 5 yr survival in end stage disease from 20% to 70% Prognosis 5 yr survival 50% Hepatitis Hepatic Encephalopathy As liver fails nitrogenous waste builds up and enters the circulation; astrocytes in the brain clear it (involving conversion of glutamate to glutamine - excess glutamine shifts the osmotic balance and fluid enters cells creating cerebral oedema Grade I: altered mood / behaviour, sleep disturbance Grade II: drowsiness, confusion, slurred speech Grade III: stupor, incoherence, restlessness Grade IV: coma Liver Function Tests Enzymes AST / ALP / ALT / Bilirubin ALT - also raised with muscle damage ALP - also raised with renal damage, Paget's disease, children, and fractures Functions Clotting Treat with: FFP / cryoprecipitate, vitamin K, keep warm (clotting less effective when cold) Avoid colloids Colloids can disrupt clotting factors - in worse case can lead to DIC in predisposed patients (septic) Stop warfarin and aspirin Albumin If falls can lead to massive interstitial oedema Treat with human albumin solution Glucose Alcoholic Liver Disease AST ++ ALT + AST : ALT > 2 Hep C AST + or = ALT ++ AST : ALT < 1 Non Alcoholic Fatty Liver Disease AST + ALT ++ AST : ALT < 1 Portal Hypertension Causes Pre-hepatic Portal vein thrombosis; splenic vein thrombosis Hepatic Cirrhosis; schistosomiasis; sarcoidosis; myeloproliferative diseases Post hepatic Budd-Chiari syndrome; right sided heart failure Varices Portal HT causes dilated collateral veins at sites of portosystemic anastomosis Commonly occur in the lower oesophagus, but also around the umbilicus snd in the rectum Develop in patients with cirrhosis when portal pressure > 10 mmHg Variceal bleeding may develop when portal pressure > 12 mmHg (up to 50% mortality) Gallstones Bile contains cholesterol, bile pigments (Hb) and phospholipids Acute Cholecystitis Stone impactation in neck of gallbladder Continuous epigastric pain (referred to R shoulder), vomiting, fever Treatment: NBM, analgesia, antibiotics, cholecystectomy Chronic Cholecystitis Stones cause chronic inflammation +/- colic Abdo discomfort, distension, nausea, fat intolerance Investigate with ultrasound Treatement: cholecystectomy Liver.mmap - 07/09/2010 -
- 8. Liver 2 Hepatitis B (DNA virus) Spread Blood products, IVDU, sexual intercourse, direct contact Risks At risk groups IVDU & sexual partners; health workers; haemophiliacs Haemodialysis; sexually promiscuous; close family members of carriers; staff of long term institutions Endemic in Far East, Africa, Mediterarranean Incubation 1 - 6 months Symptoms & Signs Resembles hep A Extra hepatic features are more common Tests Antigens HBsAg Surface Present 1 - 6 months after exposure Persistent for 6 months implies carrier status HBcAg Core HBeAg DNA material Present after acute illness Implies high infectivity Antibodies Abs Implies vaccine or previous infection Abc Implies previous infection Management Vaccination May be universal or for high risk groups Passive immunisation may be given following high risk exposure Given HBsAg to allow body to produce Abs Treatment Supportive Avoid alcohol Complications Fulminant hepatic failure (rare); relapse; prolonged cholestasis; chronic hepatitis (10%); cirrhosis; hepatocellular carcinoma (upto 60 x increased risk) Hepatitis C (RNA flavivirus) Spread Blood; IVDU; sexual; acupuncture Course Early infection is often mild / asymptomatic 85% develop chronic infection; 25% develop cirrhosis; a few get hepatocellular cancer Tests LFTs; anti-HCV antibodies; HCV-PCR Liver biopsy if HCV-PCR +ive to assess liver damage Management Interferon alpha & ribavirin in chronic infection Interferon alpha in acute stage may reduce progression to chronic disease Hepatitis A (RNA virus) Spread Faecal-oral route Often in travellers / institutions Incubation 2 - 6 weeks Symptoms & Signs Prodrome Fever, malaise, anorexia, nausea, arthralgia Jaundice +/- hepatosplenomegaly Tests Serum transaminases rises 3 weeks after exposure IgM rises from day 25; IgG remains detectable for life Management Prevention Passive immunisation Human Ig gives upto 3 months immunity to those at risk (travellers, household contacts) Active immunisation I year immunisation; extended to 10 years after 6 months booster Treatment Symptomatic relief Prognosis Usually self limiting Fulminant hepatitis occurs rarely; chronic liver disease does not occur Liver 2.mmap - 07/09/2010 -